© Borgis - Postępy Nauk Medycznych 2/2010, s. 147-152
Marcin Błoński, Waldemar Rylski, *Stanisław Pomianowski
Intramedullary Nailing of Femoral Shaft Fractures – Review of Locking Techniques
Leczenie złamań trzonu kości udowej gwoździem śródszpikowym blokowanym – omówienie sposobów ryglowania
Department of Orthopaedics and Traumatology, the Medical Centre of Postgraduate Education, Professor Adam Gruca Hospital in Otwock
Head of the Department: prof. Stanisław Pomianowski, M.D., Ph.D.
Streszczenie
Operacyjne leczenie złamań trzonu kości udowej opiera się na opracowanej przez Kempfa i Grosse'a technice zespolenia gwoździem śródszpikowym ryglowanym. Zespolenia gwoździem śródszpikowym ryglowanym jest stosunkowo mało inwazyjną techniką, zapewniającą stabilne zespolenie umożliwiające wczesne usprawnianie i prawidłowy zrost złamania. Dodatkowo istnieje możliwość rozwiercenia kanału szpikowego. W zależności od wskazań można gwóźdź wprowadzić zarówno od końca dalszego kości udowej, jak i od jej części proksymalnej. W zależności od postaci złamania stosuje się zespolenie statyczne lub dynamiczne. Jedynie w przypadku złamania poprzecznego można zastosować gwoździowanie bez śrub ryglujących. W przypadku złamania poprzecznego w części bliższej trzonu kości udowej, gwóźdź należy ryglować powyżej szczeliny złamania. Analogicznie w przypadku złamania poprzecznego w obrębie części dalszej trzonu kości udowej, ryglowanie wykonuje się poniżej szczeliny złamania. W przypadku wszelkich złamań niestabilnych, ryglowanie należy wykonać powyżej i poniżej poziomu złamania, bez względu na jego lokalizację. W przypadku wykonania zespolenia z ryglowaniem statycznym, należy celem stymulacji powstania prawidłowego zrostu kostnego, wykonać jego wtórną dynamizację. Nie wszyscy operatorzy są jednak przekonani o zasadności wykonywania wtórnej dynamizacji.
Summary
Surgical treatment of femoral shaft fractures has been based on locked intramedullary nailing since the introduction of its current principles by Kempf and Grosse. Locked intramedullary nailing is a low-invasive technique which allows stable fixation permitting early ambulation and proper fracture union. Intramedullary canal can be additionally reamed depending on the surgeon's decision. If desired, nailing may be performed in both antegrade and retrograde manner. The nail is locked either statically or dynamically using bolts located at its ends according to the fracture type. Only transverse fractures of the middle third of the femur may be treated without locking the nail or with locking only one of its ends. In case of transverse fractures of the proximal part of femoral shaft locking the nail above the fracture is required. Conversely, in case of transverse fractures of the distal part of femoral shaft the nail should be locked below the fracture. All unstable femoral shaft fractures require locking the nail at its both ends regardless of the fracture level. When static locking is done, the nail should be dynamized secondarily after 8-10 weeks in order to enhance proper fracture healing, however this view is not unanimously shared by all surgeons.

Surgical treatment of femoral shaft fractures should permit fast resumption of ambulation and proper fracture union. Locked intramedullary nailing is the mainstay of treatment (1, 2). This technique is a low-invasive, one allowing to shorten the time of hospitalization. Intramedullary nailing permits good fixation of the fracture with proper limb alignment and preservation of periosteal vascularization. Reaming of the intramedullary canal has an additional effect of spongious bone autografting which may stimulate fracture healing (3, 4). Antegrade techniques in which the nail is inserted through the piriformis fossa on the tip of the greater trochanter are less traumatic for the patient and more simple to perform for the surgeon. Obesity, pregnancy, ipsilateral acetabular fractures, ipsilateral lower extremity fractures are among indications for retrograde nailing (5).
Historically one of the most important techniques was the one described by Kuntscher in 1940. It was subsequently upgraded first in 1952 when he adopted elastic reamers and then in 1968 when he started to employ locked nailing. This method was developed in 1972 by Grosse and Kempf working in Strasbourg and has been promoted since then.
Two types of nail locking are currently in use, static and dynamic one. In case of dynamic locking the nail is inserted without bolts or with one or more bolts located in either proximal or distal bone fragment, depending on the fracture type. When this type of locking is used, weight-bearing on the affected limb results in compression of the bone fragments. Rotational movements of the fragments must not occur which explains why this type of locking can be applied only when there is full contact between the fragments. Static locking with bolts on both ends of the nail allows complete stabilization of the fragments (6).
Classic Kuntscher technique is used for treatment of transverse fractures of the middle third of femoral shaft (fig. 1). The nail is inserted without any locking bolts or with the bolts only in the distal fragment when there is a threat of a rotational displacement (7).
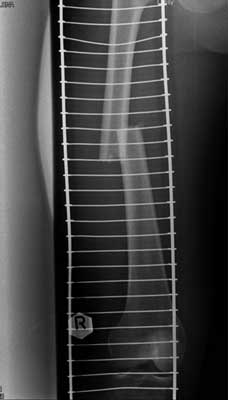
Fig. 1. Transverse midshaft femoral fracture.
Transverse fractures of the proximal part of femoral shaft (fig. 2) require locking of the nail above the fracture. Conversely, in case of transverse fractures of the distal part of femoral shaft (fig. 3) the nail should be locked below the fracture.

Fig. 2. Transverse proximal femoral shaft fracture.

Fig. 3. Transverse distal femoral shaft fracture.
All unstable femoral shaft fractures require locking the nail at its both ends regardless of the fracture level (fig. 4, 5 and 6).

Fig. 4. Midshaft spiral fracture of the femur.

Fig. 5. Spiral fracture of the proximal femoral shaft.

Fig. 6. Multifragmentary distal femoral shaft fracture.
When static locking is done, the nail should be dynamized secondarily after 8-10 weeks after initial surgery in order to enhance proper fracture healing. Some surgeons decide to perform this procedure only when there is no full contact of bone fragments basing on their experience with patients who had not agreed for nail dynamization and whose fractures had healed with no complications (6). When the nail is dynamized, it is important always to remove the bolts which are more distant to the fracture.
In our centre locked intramedullary nailing has become the standard of treatment of femoral shaft fractures to which other treatment methods are now compared. Below are some of the clinical cases of patients treated in our hospital.
Patient M. L. 22 years old, case no. 1633/2007, motor vehicle injury (fig. 7). The surgery was postponed to the 19th day after the accident due to an upper airways bacterial infection. This femoral shaft fracture was fixed with an intramedullary nail which was locked dynamically (fig. 8 and 9). The radiograph taken 2 years after surgery shows full fracture healing (fig. 10), the next one shows the same patient after the hardware removal (fig. 11).

Fig. 7. Transverse femoral shaft fracture, 8 days after injury.

Fig. 8. Transverse femoral shaft fracture, 19 days after injury.

Fig. 9. Transverse femoral shaft fracture, 19 days after injury.

Fig. 10. Transverse femoral shaft fracture, 13 months after injury.

Fig. 11. Transverse femoral shaft fracture, 18 months after injury.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
24 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
59 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
119 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 28 zł
Piśmiennictwo
1. Winquist RA, Hansen ST Jr, Clawson DK: Closed intramedullary nailing of femoral fracture: a report of five hundred and twenty six cases. J Bone Joint Surg Am 1984; 66: 529-539.
2. Brumback RJ, Ellison PS Jr, Poka A et al.: Intramedullary nailing of femoral shaft fractures, I: Decision making errors with interlocking fixation. J Bone Joint Surg Am 1988; 1441-1452.
3. Shepherd LE, Shean CJ, Gelalis ID et al.: Prospective randomized study of reamed versus unreamed femoral intramedullary nailing: an assessment of procedures. J Orthop Trauma 2001; 15: 28-33.
4. Tornetta P 3rd, Tiburzi D: Reamed versus nonreamed antegrade femoral nailing. J Orthop Trauma 2000; 14: 15-19.
5. Ostrum RF, DiCicco I, Lakatos R et al.: Retrograde intramedullary nailing of femoral diaphyseal fractures. J Orthop Trauma 1998; 12: 464-468.
6. Kempf I: Gwoździowanie śródszpikowe ryglowane w leczeniu złamań kości długich. From materials of „IV Śląskie Sympozjum Traumatologiczne”, Katowice 1997.
7. Semenowicz J: Operacyjna technika śródszpikowego zespalania złamań trzonu kości udowej gwoździem Grosse i Kempfa. From materials of „IV Śląskie Sympozjum Traumatologiczne”, Katowice 1997.