© Borgis - Postępy Nauk Medycznych 6/2012, s. 534-539
*Andrzej Sionek1, Jarosław Czubak1, Maria Katarzyna Borszewska-Kornacka2, Bartłomiej Grabowski1
Ocena morfometryczna rozwoju stawów biodrowych u dzieci z ciąż wielopłodowych według metody Grafa. Czy ciąża wielopłodowa jest czynnikiem ryzyka rozwojowej dysplazji stawów biodrowych?
Hip joint development in multiple pregnancy infants – Graf method morphometric assessment. Is a multiple pregnancy a risk factor of developmental hip dysplasia?**
1Department of Orthopaedics, Pediatric Orthopaedics and Traumatology, Postgraduate Medical Education Centre, prof. A. Gruca’s Teaching Hospital, Warsaw – Otwock
Head of Department: Jarosław Czubak, MD, PhD, Associate Professor
2Department of Neonatology and Intensive Newborn Care, Medical University of Warsaw, Princess Anna Mazowiecka Teaching Hospital
Head of Department: Prof. Maria Katarzyna Borszewska-Kornacka, MD, PhD
Streszczenie
Wstęp. Etiologia rozwojowej dysplazji stawów biodrowych (R.D.S.B) jest złożona. Nie ma jednoznacznych poglądów dotyczących wpływu ciąży wielopłodowej (c.w.) na powstawanie R.D.S.B. Celem pracy jest ustalenie czy c.w. jest czynnikiem ryzyka R.D.S.B., oraz określenie wpływu c.w. i czasu jej trwania na rozwój stawów biodrowych.
Materiał i metody. Badaniem pierwszorazowym objęto 200 dzieci z c.w. (400 stawów biodrowych), oraz grupę kontrolną 63 dzieci (126 stawów biodrowych), urodzonych z ciąż pojedyńczych. Badanie ultrasonograficzne wykonywane było metodą Grafa. Dzieci badane były trzykrotnie w analogicznych odstępach czasu: pierwsze badanie kontrolne w pierwszych dobach życia, drugie badanie kontrolne w 12 tygodniu życia, trzecie badanie w 6 miesiącu.
Wyniki. W pierwszym badaniu dzieci z c.w. 28 bioder (7%) zakwalifikowano do grupy IIa. W grupie kontrolnej typ IIa odnotowano w 19 biodrach (15,1%). W terminie pierwszego i drugiego badania w obu grupach nie stwierdzono stawów biodrowych dysplastycznych, a typ IIa występował częściej u dzieci z grupy kontrolnej. W kolejnych badaniach dzieci z obu grup stwierdzono zwiększający się odsetek bioder typu Ia. W grupie dzieci z c.w. średnia wartości kąta α wzrastała w kolejnych badaniach, a w badaniu II i III oceniany parametr przyjmował niższe wartości w grupie kontrolnej.
Średnia wartości kąta β w obu badanych grupach zmniejszała się w kolejnych badaniach.
Wnioski. C.w. nie jest czynnikiem zwiększającym częstość występowania stawów biodrowych typu IIa.
Począwszy od około 12 tygodnia życia niemowlęcia, cześć kostna dachów panewek stawów biodrowych dzieci z c.w. była lepiej rozwinięta w porównaniu ze stawami dzieci urodzonych z ciąż pojedynczych.
Summary
The aetiology of the developmental dysplasia of the hip (DDH) is multifactorial. There are no unambiguous views regarding the effect of multiple pregnancy (MP) on DDH development.
The aim of the study is to determine whether MP is a DDH risk factor and to determine the influence of MP on hip joint (HJ) development.
The first examination included 200 MP infants (400 HJ) and a control group of 63 single pregnancy (SP) infants (126 HJ). Graf method hip joint ultrasonography was performed three times at similar intervals. The first examination was performed in the first postnatal days, the second at 12 weeks and the third at 6 months.
During the first examination of MP infants 28 HJ (7%) were allocated to group IIa. In the control group there were 19 Type IIa HJ (15.1%). During the first and second examination no dysplastic HJ were reported in both groups with Type IIa occurring more commonly in the controls. In the subsequent examinations there was an increasing percentage of Type Ia HJ in both groups. In the MP infants the mean value of the α angle increased in subsequent examinations and in the control group the values were lower in examination II and III. The mean value of β angle decreased in subsequent examinations in both groups.
MP does not predispose to increased incidence of Type IIa HJ. Starting from approx. the 12th postnatal week the osseous part of HJ acetabular roofs was developed better in MP than in SP infants.

INTRODUCTION
Gemellology is an interdisciplinary domain dealing with the development of twins. Multiple pregnancy is simultaneous development of two or more foetuses in the uterus. The incidence of spontaneous multiple pregnancy is approx. 1.05-1.35% (1). An increasing number of multiple pregnancies have been observed within the last twenty years in developed countries. At the same time, there has been a decrease in the general number of births. The factors contributing to this phenomenon, including assisted reproductive technology (ART), hormonal stimulation and hormonal contraceptives, have not been fully elucidated.
The developmental dysplasia of the hip (DDH) refers to the abnormal formation of this joint, possibly leading to the dislocation of the hip, occurring during intrauterine development, in the perinatal period or within the first postnatal weeks.
The aetiology of the disorder has a complex nature, with the factors contributing to the deformity of the hip joint development subdivided into hormonal, genetic and mechanical (2).
No unambiguous views regarding the effect of multiple pregnancy on DDH development have been presented so far. Some authors indicated twin pregnancy as a factor predisposing to DDH development (3-7). Apparently, the number of DDH risk factors, with intrauterine crowding being the leading one, should increase the risk of DDH development in multiple pregnancy.
Recent decades have faced an increase in the number of multiple pregnancies, but their effect on DDH development has remained unknown and the number of studies (predominantly retrospective ones) has been negligible. Therefore, the present authors have decided to conduct a prospective study concerning this issue. The study aims to refute or confirm the hypothesis that multiple pregnancy is a DDH risk factor and to determine the effect of multiple pregnancy on hip joint development.
MATERIAL AND METHODS
The study group consisted of infants born in the 2nd Department of Obstetrics and Gynaecology of the Medical University of Warsaw. The first examination was performed between 1 June 2003 and 2 December 2004 in the Department of Neonatology and Intensive Newborn Care of the Medical University of Warsaw and involved 200 children (400 hip joints) from 95 multiple pregnancies, including 97 female infants (48.5%) and 103 male infants (51.5%). The study group comprised 172 infants from twin pregnancies, 24 from triplet pregnancies and 4 from a quadruple pregnancy. The mean duration of a multiple pregnancy was 36 weeks (27 to 41 weeks).
The control group consisted of 63 single pregnancy infants (126 hip joints) including 29 female (46.0%) and 34 male infants (54.0%). The study did not involve infants diagnosed with neuroorthopaedic disorders (meningomyelocoele), congenital syndromes or those in poor overall condition placed at the ward of intensive newborn care. Only neonates with a birth weight exceeding 1000 g were enrolled (8).
A unified examination protocol was used for all participants. It involved the following elements:
– history taking to identify factors increasing the risk of DDH,
– a physical examination to assess the presence of clinical manifestations of DDH,
– an ultrasonographic study to evaluate hip joint development using morphometric indices.
The study and control group subjects underwent three examinations at similar intervals. The first examination was performed in the first postnatal days, the second at 12 weeks and the third at 6 months (mean of 25 weeks).
The second and third examination were conducted at the Clinic of Luxation Prevention, Department of Orthopaedics, Centre for Medical Postgraduate Education (CMKP), Prof. A. Gruca Memorial Independent Public Teaching Hospital in Otwock. The clinical and sonographic examinations were carried out by a specialist in orthopaedics and traumatology (the first author of the present paper) with 14 years of professional experience. During the first examination the parents received written information concerning the aim of the study.
Clinical assessment of the multiple and single pregnancy infants was always conducted according to the same examination procedure, which included the evaluation of hip joint compactness, range of motion, asymmetry of thigh skin folds and coexisting skeletal malformations.
Hip joint ultrasonography was performed according to the Graf method (9) with children placed in a Graf cradle and their hips flexed at approx. 35° and rotated internally at approx 10°. On the basis of alpha and beta angle values, hip joints were classified into one of 9 groups using a Graf sonometer. The examination of neonates was performed with a 12.5 MHz linear probe and the examination of infants was performed with a 7.5 MHz probe. The first ultrasonographic examination of multiple pregnancy infants was conducted with ATL Ultrasound HDI 3500 device manufactured by Advanced Technologies Laboratories, Bothell, WA, USA, and subsequent examinations and examinations of single pregnancy infants were conducted with Siemens SL-1 device manufactured by Siemens AG, Erlagen, Germany.
Statistical analysis was conducted with the U-test, Wilcoxon test and the t-student test. The threshold of statistical significance was assumed at p = 0.05. The calculations were performed with StatSoft’s STATISTICA software package.
RESULTS
Hip joint development – Graf method morphometric assessment
Multiple pregnancy infants
Basing on the results of the first sonographic examination of 400 joints in 200 multiple pregnancy infants, 28 joints (7.0%) were assigned to Type IIa group. No pathologically dysplastic hip joints were recorded.
The analysis of hip joint development in multiple pregnancy infants in subsequent studies revealed an increasing percentage of Type Ia joints and a decreasing percentage of Type Ib and IIa joints. Only one male infant had his both hip joints classified as Type IIa in the second examination and Type IIb in the third one. Therefore, it was necessary to apply hip abduction orthosis in this case. Specific numbers of joint types in multiple pregnancy infants are presented in table 1 and figure 1.
Table 1. Graf hip joint types in successive sonographic examinations of multiple pregnancy infants.
| | Graf hip joint type | Total |
| Ia | Ib | IIa | IIb |
| Examination I | 269
67.25% | 103
25.75% | 28
7.0% | | 400
100.0% |
| Examination II | 252
84.9% | 42
14.1% | 3
1.0% | 0
0% | 297
100.0% |
| Examination III | 211
90.5% | 20
8.6% | | 2*
0.9% | 233
100.0% |
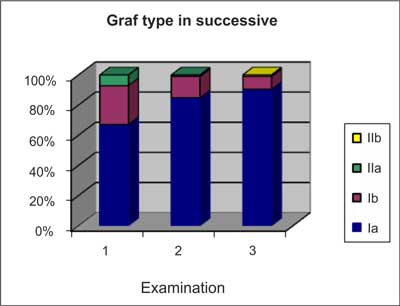
Fig. 1. The percentage of Graf hip joint types in successive sonographic examinations of multiple pregnancy infants.
Control group
The first examination of 126 joints in 63 controls revealed 19 Type IIa joints (15%).
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
24 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
59 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
119 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 28 zł
Piśmiennictwo
1. Bręborowicz G, Kempiak J: Ciąża wielopłodowa. [W:] Położnictwo i ginekologia. Podręcznik dla studentów. Pisarski T. editors PZWL Warszawa 2002; 528-539.
2. Wientrub S, Grill F: Ultrasonography In Developmental Dysplasia of the Hip. The Journal of Bone and Joint Surgery 2000; 82: 1004.
3. Dorn U: Hip screening in neonates. Clinical and sonographic findings. Wien Klin Wschr 1990; 102 [Suppl 181]: 1-22.
4. Hatzmann W, Skowronek B, Hoffken H et al.: Sonographic findings in the hip of newborn infants after pregnancy and labor from breech position. Ultraschall Med 1993; 14: 163-168.
5. Őmero?lu H, Koparal S: The role of clinical examination and risk factors in the diagnosis of developmental dysplasia of the hip: a prospective study in 188 referred young infants. Arch Orthop Trauma Surgery 2001; 121: 7-11.
6. Psenner K, Ortore P, Fodor G, Struefer J: Echography of the hip of the newborn infant. Radiol Med 1990; 79: 575-581.
7. Zwierzchowski H, Synder M, Garncarek P: Ultrasonografia dziecięcego stawu biodrowego. Wydawnictwo Folium, Lublin 1994; 48-49.
8. Kornacka MK: Ciąża wielopłodowa. [Bręborowicz G. H., Malinowski W, Ronin-Walknowska E. red.], Ośrodek Wydawnictw Naukowych. Poznań 2003; 363-371.
9. Graf R, Farkas P, Lercher K et al.: Kompendium sonografii biodra. Wydawnictwo Stolzalpe 1999.
10. Graf R: New possibilities for the diagnosis of congenital dislocation by ultrasonography. Journal of Pediatric Orthopaedic 1983; 3: 354-359.
11. Graf R, Schuler P: Guide to sonography of the infant hip. Congenital Dislocation and Dysplasia of the Hip. Edited by D. Tönnis. New York, Springer 1987.
12. Graf R: Clasification of hip joint dysplasia by means of sonography. Arch Orthop Trauma Surgery 1984; 102: 248-255.
13. Graf R: Fundamentals of sonographic diagnosis of infant hip dysplasia. J Pediat Orthop 1984; 4: 735-740.
14. Hensinger R: Australian Pediatric Orthopaedic Society [APOS] Meeting; Royal Children’s Hospital, Melbourne, Australia: June 14-15, 1997. J Pediat Orthop 1998; 18,2: 275-278.
15. Rühman O, Lazovič: Sonographisches Hüftgelenk-Screening bei Neugeboren. Ist die Zwillingsschwangerschaft ein Dysplasie-Risikofaktor. Ultraschall in Medizin 1998; 19: 64-69.
16. Rühman O, Lazovič D, Bouklas P et al.: Ultrasound examination of neonatal hip: correlation of twin pregnancy and congenital dysplasia. Twin Research 2000; 3: 7-11.
17. Witt HJ, Weickert H, Merk H, Woltersdorf JP: Studies of hip dislocation in twins. Beitr Ortop Traumatol 1989; 36: 259-263.
18. Psenner K, Ortore P, Fodor G, Struefer J: Echography of the hip of the newborn infant. Radiol Med 1990; 79: 575-581.
19. De Pellegrin M: Ultrasound screening for congenital dislocation of the hip. Italian J of Orthopaedics and Traumatology 1991; 17: 547-553.
20. Barlow TG: Early diagnosis and treatment of congenital dislocation of the hip. J Bone Joint Surg [Br.] 1962; 44: 292-301.
21. Czubak J, Kotwicki T: Ultrasound measurments of the newborn hip. Comparison of two methods in 657 newborns. Acta Orthpopedica Scandinavica 1998; 69: 550-551.
22. Czubak J, Kotwicki T: Analiza diagnostyki ultrasonograficznej stawów biodrowych w pierwszych miesiącach życia – jak wybrać właściwy program badań przesiewowych? [W:] XII Sympozjum Sekcji Ortopedii Dziecięcej PTOiTr. Lublin/Nałęczów, 6-8.06.2002, s. 70.
23. Marks DS, Clegg J, Al-Chalabi AN: Routine ultrasound screening for neonatal hip instability. J Bone and Joint Surg 1994; 76-B: 534-538.
24. Boeree NR, Clarke NMP: Ultrasound imaging and secondary screening for congenital dislocation of the hip. J Bone and Joint Surg 1994; 76-B: 525-533.
25. Clarke NM: Diagnosis congenital dislocation of the hip. British Med J 1992; 305: 435-436.