© Borgis - New Medicine 3/2012, s. 91-94
Júlia Bartos1, *Judit Mészáros2
Dental health behaviour of adolescents and their parents II
1Dentist, Student of Semmelweis University PhD School
Scientific counsellor: dr. Sándor Hollós, PhD
2Psychologist, Dean of the Faculty of Health Sciences, Semmelweis University
Rector of Semmelweis University: prof. dr. Ágoston Szél, MD, PhD
Summary
The aim of the second part of our study is similar to that of the first part: our main target is to get a picture about the adolescents’ and their parents’ self-qualification concerning the status of their teeth and also about their attitude to dental prevention. During the survey including closed and open questions we processed 164 parents’ and 186 adolescents’ questionnaires. In the results statistically proven differences can be seen in the oral hygiene patterns of the parents and their children and also in their attitude towards health education. According to the conclusions the adolescents have greater trust in the possibility of dental prevention, but their parents are more open to dissemination of information on health promotion, so we suggest holistic formation of health behaviour in all age groups.
INTRODUCTION
In the introduction of the first part of this paper we outlined the aggregation of current social and health protection problems that led us to choose this topic – that focuses on health promotion and prevention and is far beyond the boundaries of dentistry – as the subject of our research. We cannot disregard the importance of maintaining healthy teeth, restoring the values of dental care culture and getting them accepted. Besides its medical advantages, healthy, cared, aesthetic – if necessary treated and reorganised – teeth might by all means mean a better, higher quality of life, which increases comfort and self-respect, and is part of the real ‘well-being’ both in child- and adulthood. Beautiful, even, well-cared teeth may help to achieve a confident appearance, and might be a decisive factor in the internal harmony and spiritual and bodily homeostasis of the individual.
The conscious promotion of dietary and oral hygiene culture is slow to develop, while environmental harms and lifestyle anomalies are quick to grow. As a consequence, the number of dental diseases is increasing. Thus there is no other alternative than prevention. Recently, dental health-care has significantly improved, but there has been no parallel improvement in public satisfaction and the dental state of society: the level of health culture is low, private practice is very expensive and dentists and other experts are not really interested in prevention. That is why most people are confined to the services of emergency dental care (e.g. tooth extraction). Teeth capable of chewing functions, which is the prerequisite of healthy nutrition, stable oral hygiene, even the enforcement of aesthetic aspects, are not generally required.
The above-mentioned experiences suggest that the paramedical assisting professionals – in the course of their preventive activity – should call attention to proper dental health behaviour and modern dental hygiene techniques as early as possible.
This means that in the process of health education and health promotion the professional preventive work should be started with children to get dental hygiene practice integrated in their everyday life and not to let them have the neglected dental health status of the present adult population by the time they grow up. Moreover, the real ambition is the creation and interiorisation of necessity in young people to develop and preserve their own dental hygiene and health. The first stage in interiorising this preventive knowledge and becoming a pattern is always in preschool age, while the phase when it becomes conscious and skills get fixed is in the sensitive period of adolescence that we examined.
At the beginning, prevention covered two widespread diseases, dental caries affecting children and periodontal disease, which affects adults as well, but in recent decades the frequency of oral carcinoma has dramatically increased so the focus has been transferred to the prevention of the spread of cancer. Besides the different causes responsible for tumour formation in the cavity of the mouth, e.g. smoking, drinking alcohol or immunological factors, the late detection of carcinomas also worsens the position of prevention. That is why it can happen that in default of proper dental screening more than half of maxillo-facial malignoma cases have been detected in a late, advanced stage. The above mentioned facts and data show the great importance of dental prevention both in adolescence and adult age (1).
In dental preventive work, as in general prevention, three levels of prevention can be distinguished: primary, secondary and tertiary prevention. The conception and practice of health promotion, however, distinguishes a fourth level before the other three that is known as primordial prevention.
In the course of dental preventive activities it is highly important to categorise the target groups – children, adults and elderly people – and also to distinguish special groups: pregnant women, people suffering from systemic diseases, and people with mental, sensory and physical disabilities (2).
Primary prevention
Its target is to prevent the development of dental diseases, possibly before treatment has become necessary, or reverse these processes. In dentistry this activity covers the prevention of the development of caries, gingivitis, as well as periodontitis, dental anomalies and oral malignant tumours – by applying certain preventive interventions, and by developing a suitable individual lifestyle. When speaking about primary prevention we have to mention the so-called primary-primary prevention, which is applied in the case of pregnant women in the prenatal period.
Secondary prevention
Its target is to detect the diseases mentioned in the case of primary prevention early and to prevent their progress, e.g. gingivitis therapy, orthodontic treatment, early filling, diagnosis and care of precancerous lesions. Early diagnoses can be set up in the course of individual examinations or organised screenings.
Tertiary prevention
The task of tertiary prevention is to replace the lost tissue sets and to rehabilitate the patients. This level of prevention means the treatment of the already developed diseases, by applying interventions such as preserving dental treatments (filling, root canal treatment), prosthetic treatments (fixed or removable prostheses) and oral surgical restorative treatments (tooth extraction, other operations).
Primordial prevention
Primordial prevention is the fourth level of prevention which involves all health policy, general public health activities and measures that can prevent the development and spread of mass-threatening social, environmental etc. factors on a social level.
Aim
The aim of the survey was to analyse the self-qualification and self-image of two tested age-groups (12-14-year-old adolescents and their on average 43-year-old parents) about the status of their teeth. Another research target was to find out whether there was a significant difference between the two samples in the question of dental attitude and health behaviour. Besides the above the attitude of the respondents toward dental prevention and health promotion is also worth exploring.
RESULTS
To the question about the frequency of tooth ache of the respondents, 43.6% selected the answer ‘rarely’ while a majority of the students (51.6%) selected the answer ‘never’. More respondents in the parents’ group (5.8%) had tooth ache frequently, and approximately the same number of people did not remember their tooth aches: 17.2-19.4% (fig. 1).
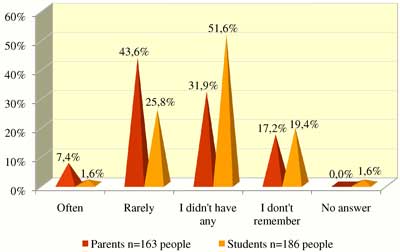
Fig. 1. Frequency of tooth ache.
According to the results of the diagram presenting the self-qualification concerning the status of their teeth 53% of the young people declared all of their teeth healthy while 11.7% of the parents declared the same. 31.9% of the parents and 8.1% of the adolescents have cavities or caries to be treated (fig. 2).
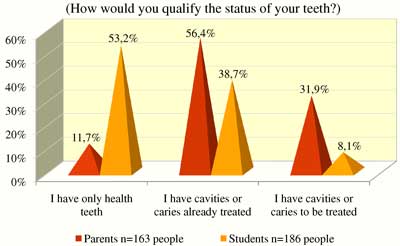
Fig. 2. Self-qualification of the status of their own teeth I.
A further diagram about the self-qualification shows that a significant proportion of both the adults and the adolescents (56.5-43.6%) think their own teeth somehow beautiful. 12.3% of the parents and 32.3% of the adolescents regard their own teeth as very nice, while 4.9% of the parents are not satisfied with the look of their teeth at all (fig. 3).
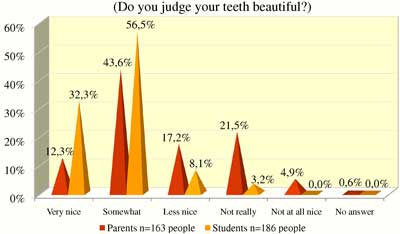
Fig. 3. Self-qualification of the status of their own teeth II.
30.1% of the parents do not smile, do not laugh with pleasure because of the current status of their teeth. This proportion is 11.3% in the students. 68.7% of the adults and 88.7% of the adolescents are not inhibited from smiling or laughing (fig. 4).
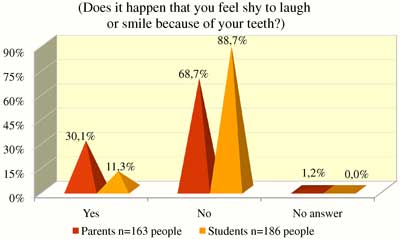
Fig. 4. Self-qualification of the status of their own teeth III.
As regards the questions about prevention 75.7% of the young people think that caries can be prevented with an adequate way of life, attention and conscious health preservation, against the parents’ opinion, 48.5% of whom thought the same. Roughly the same proportion of the adult and young respondents are unsure (18.4-16.1%). 32% of the adults think that they cannot do too much for the genetically determined status of their teeth while only 4.8% of the adolescents think the same (fig. 5).
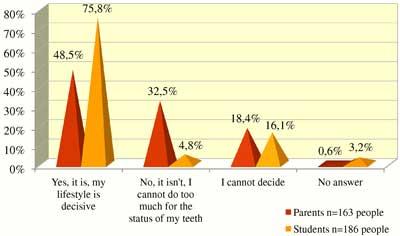
Fig. 5. Is it possible to prevent caries and tooth deterioration in chlidhood?
52.5% of the parents and 54.8% of the adolescents would consider a dental health promoting presentation unnecessary, but a greater proportion of parents selected the answer ‘Yes, I would be interested’ than the adolescents (30.7-14.5%). 16% of the adults and 24.2% of the adolescents are not really interested in this topic (fig. 6).
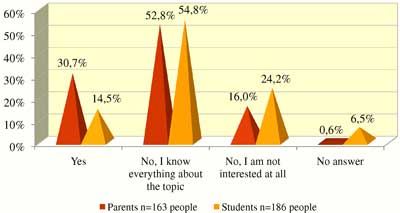
Fig. 6.Would you be interested in participating in a presentation or demontstration schowing the right tooth brushing technique, oral hygiene?
In the range of information sources on oral hygiene, and educating- socialising patterns family has the first place, since 93.5% of the respondent adolescents mentioned family and relatives as the most important health promoting factor. About half of the young people (54.8%) have also obtained information on oral hygiene in the dental surgery. The role of teachers and media in information means 33.9% i.e. 30.6%. Adolescents have obtained the least information about dental hygiene from newspapers (9.7%) and friends (11.3%) (tab. 1).
Table 1. Who told you about the importance of dental hygiene?
| | People | % |
| Parents, relatives | 174 | 93.5% |
| Dentist, dental assistants | 102 | 54.8% |
| TV, radio | 63 | 33.9% |
| Teachers | 57 | 30.6% |
| Other physicians, nurses | 27 | 14.5% |
| Friends | 21 | 11.3% |
| Newspapers, magazines | 18 | 9.7% |
| Other | 12 | 6.5% |
When comparing the answers given by the parents and the students to the questions of the questionnaire we can find significant differences between the data of the adults (parents) and adolescents (students) in three questions: as regards the frequency of toothache (t = 0.007; p < 0.05), the intention to participate in a presentation on dental hygiene (t = 0.01; p= < 0.05) and the possibility of preventing dental diseases (t = 0.007; p < 0.05).
DISCUSSION
1. In the self-qualification concerning the status of their teeth – probably due to their different age – the young people judge their own status more positively, their teeth to be nicer, in better condition. It is notable, however, that almost one third of the respondent adults feel disinclined to laugh or to smile because of the status of their teeth, which means that the status of teeth can affect the metacommunicative expression of emotions.
2. It is regrettable that one third of the parents have bad, untreated teeth, which sets a negative example for their adolescent children.
3. The fact that health education presentations on dental hygiene were considered unnecessary by more than half of the adults and the adolescents as well should be underlined, because they do not trust in their ability to learn new things and to acquire new skills. As regards openness, the adults show significantly higher interest in information of this kind.
4. The adolescents are more optimistic about the prevention of frequent dental diseases, while – quite interestingly – their parents consider the status of their teeth as their genetic heritage.
5. Most young people heard about oral hygiene patterns in their families. In front of their peers it is not typical to mention this issue. This can be explained by the special developmental psychological quality of adolescents that they feel too shy and timid to talk about dental hygiene issues with their friends.
CONCLUSIONS
1. In the course of dental pycho-educational activities it is the adolescents who should be first of all convinced, since – as our results show – they are not open enough to the latest dental knowledge (‘we know everything about the topic’). At the same time they recognise the possibilities of prevention, which might be the base for health educational, health-promotion activities.
2. In the range of dental prevention possibilities and scenes the development of health behaviour in school – either individually or in groups – and by the media should be more emphasised, since this type of dissemination of knowledge seems to be rather unexploited in health promotion.
3. The self-qualification of the adolescents is not influenced negatively or worsened by the status of their teeth since their self-qualification concerning the status of their teeth is rather favourable.
4. On the basis of our results we can conclude that family is the primary setting for health promotion, since adolescents get the most information and the strongest patterns there. The parents, however, should be convinced that dental health can be formed and promoted by means of health-conscious lifestyle and attention.
5. Based on the above, it can be concluded that in adolescence the long-term aim of dental health promotion is to transmit health culture and being cultured, to consciously develop the desired way and style of life, to strengthen the health-related values and norms and complex oral hygiene and to associate them with other capabilities, such as real self-knowledge, autonomy, decision-making capability and responsibility. ‘Positive health is of holistic character, a concept related to the whole human being and is in connection with the quality of life; it is not restricted to only one quality of the individual but is characteristic for the whole of his life, i.e. pervades the entirety of his life. Consequently health promotion should be accomplished in the system of these effects – on a field bordered by individual capabilities and skills' (4).
Piśmiennictwo
1. Papphalmi Zs: Tennivaló a fogászati megelőzés terén Magyarországon. Egészségnevelés 1993; 34: 249-250. 2. Nyárasdy I, Bánóczy J: Preventív fogászat. Medicina Könyvkiadó, Budapest 2009. 3. Kertai P: Megelőző orvostan – A népegészségügy elméleti alapjai. Medicina Kiadó, Budapest 1999. 4. szerk. Gritz A, Sipos K: Egészségfejlesztési szöveggyűjtemény. SE – Testnevelési és Sporttudományi Kar, Budapest 2007; 34.
