© Borgis - New Medicine 4/2012, s. 114-115
*Monika Jabłońska-Jesionowska, Małgorzata Dębska, Lidia Zawadzka-Głos
Congenital lateral fistulae on the neck in 8-years girl
Department of Pediatric Otolaryngology, Medical University of Warsaw
Head of Department: Lidia Zawadzka-Głos MD, PhD
Summary
Introduction. Congenital lateral fistulae, the anomaly of the branchial second cleft derivatives is the most common anomalies of branchial apparatus (1, 3, 4).
Material and methods. In Department of Pediatric Otolaryngology Medical University of Warsaw 8-years girl was treated because of the congenital lateral fistulae. The ultrasound image of the neck and radiography with barium (into the external opening) was done.
Results. The surgical procedure was performed in general anesthesia. The excision of whole duct of fistulae through the two incisions was made. No recurrence was observed.
Conclusions. 1. The complete excision of the entire fistulae duct is preferable treatment of choice. 2. The surgery procedure should be done as soon as possible before inflammation occurs because of high risk of adhesions (5).
INTRODUCTION
Congenital lateral fistulae is the anomaly of the branchial second cleft derivatives. There are the most common anomalies of branchial apparatus (1, 3, 4). The external opening of the fistulae is on the 1/3 lower part of the neck on anterior border of the sternicleidomastoid muscle. The internal opening (not ever observed) is in the fossa of tonsillae palatine. The duct of fistulae goes between the external and internal carotid artery and above the hypoglossal and glosso-pharyngeal nerve (1).
MATERIAL AND METHODs
In Department of Pediatric Otolaryngology Medical University of Warsaw 8-years girl was treated because of the congenital lateral fistulae.
The external opening of the fistulae was on the neck, above the clavicle, on anterior border of the right sterno-cleido-mastoid muscle. Since early childhood the parents occasionally observed the discharge from the external opening of the fistulae. It was clear and no pus and unpleasant smell was noticed. The girl never had high fever because of this discharge. She never presented inflammatory swelling of the neck, dyspnea and dysphagia.
The ultrasound image of the neck and radiography with barium (into the external opening) was done.
RESULTS
The ultrasound image showed a duct of the fistulae diameter 2-3 mm going to the top of the neck and penetrating deeply into the soft tissue. The radiography with barium showed the duct of the fistulae going to the palatine tonsil on the right (fig. 1). On the figure 2 is shown barium in the pharynx and next in esophagus. No elevated inflammation parameters was detected in blood tests.
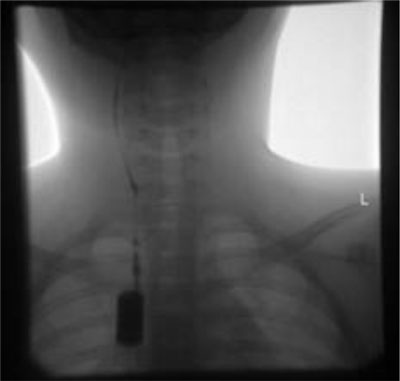
Fig. 1. The duct of fistulae.
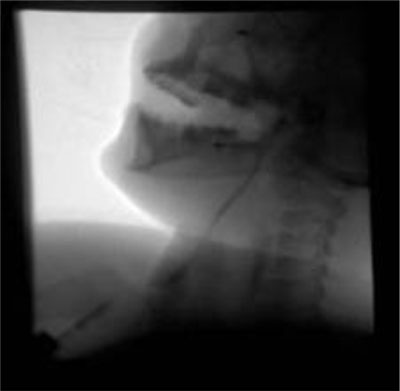
Fig. 2. The barium in the fistulae and next in pharynx and esophagus.
The surgical procedure was performed in general anesthesia. The excision of whole duct of fistulae through the two incisions was made: first incision around the external opening on the neck and second on the level of the larynx. The fistulous duct was 8 cm long. Ligation and removal of fistulae near the palatine tonsil was done (1, 2). The course of the fistulous duct was typical, between the external and internal carotid artery and near the hypoglossal and gloss-pharyngeal nerves. Tonsillectomy was needless because of lack of history of tonsillitis (1). The histological check identified a cystis branchiogenes. No recurrence was observed with the mean follow-up of 11 months (3).
CONCLUSIONS
1. The complete excision of the entire fistulae duct is preferable treatment of choice.
2. The surgery procedure should be done as soon as possible before inflammation occurs because of high risk of adhesions (5).
Piśmiennictwo
1. Gryczyńska D: Otolaryngologia dziecięca. Alfa – Medica Press 2007; 456-457. 2. Błajszczak A, Grabowski L, Łach P: The cystis and fistulas of the Neck in material of ENT Department of Rydygier District Hospital in Cracow. Otolaryngol Pol 2009; 63(5): 429-431. 3. Nicollas R, Guelfucci B, Roman S, Triglia JM: Congenital cysts and fistulas of the neck. Int J Pediatr Otorhinolaryngolog 2000; 55(2):117-124. 4. Marsot-Dupuch K, Levret N, Pharaboz C et al: Congenital neck masses. Embrionic origin and diagnosis. Report of the CIREOL. J Radiolog 1995; 76(7): 405-415. 5. Schroeder JW Jr, Mohyuddin N, Maddalozzo J: Branchial anomalies in the pediatric population. Otolaryngol Head Neck Surg 2007; 137(2): 289-295. 6. Nicollas R et al; Congenital Lateran cysts and fistulas of the Neck. International Congress Series 2003; 1254: 419-4125. 7. Walocha J, Skawina A, Gorczyca J, Skrzat J: Anatomia prawidłowa człowieka. Szyja i głowa. Wydawnictwo Uniwersytetu Jagiellońskiego, Kraków 2003; 237-244.
otrzymano: 2012-10-08
zaakceptowano do druku: 2012-10-31
Adres do korespondencji:
*Monika Jabłońska-Jesionowska
Department of Pediatric Otolaryngology Medical University of Warsaw
24 Marszałkowska St., 00-576 Warsaw
tel./fax: +48 (22) 628-05-84
e-mail: laryngologia@litewska.edu.pl
New Medicine 4/2012Strona internetowa
czasopisma New Medicine