*Łukasz Nyk1, Michał A. Skrzypczyk2, Stanisław Szempliński2, Mieszko Kozikowski1, Wojciech Michalak1, Sebastian Piotrowicz1, Szymon Kawecki1, Tomasz Dzik3, Maciej Wysocki4, Andrzej Borówka1, Jakub Dobruch1, 2
Comparison of prostate cancer grades after biopsy and radical prostatectomy
Porównanie złośliwości raka stercza ocenione na podstawie biopsji i badania preparatów operacyjnych
11st Unit of Didactics, Department of Urology, Centre of Postgraduate Medical Education, European Health Centre Otwock
Head of Department: Jakub Dobruch, MD, PhD
22nd Unit of Didactics, Department of Urology, Centre of Postgraduate Medical Education, Professor W. Orłowski Independent Public Teaching Hospital, Warsaw
Head of Department: Jakub Dobruch, MD, PhD
3Pathomorphology Division, Międzylesie Specialist Hospital, Warsaw
Head of Division: Tomasz Dzik, MD, PhD
4Pathomorphology Division, Bielany Hospital, Warsaw
Head of Division: Jan Faryna, MD, PhD
Streszczenie
Wstęp. Raka stercza rozpoznaje się na podstawie biopsji mającej z reguły charakter wielomiejscowej biopsji rdzeniowej, wykonanej igłą tru-cut pod kontrolą ultrasonografii przezodbytniczej (TRUScoreBx). Ważnym elementem oceny PCa jest określenie stopnia jego złośliwości, którą definiuje się na podstawie skali Gleasona. Istniej odmienność ocen złośliwości raka określonej na podstawie badania rdzeni tkankowych oraz na podstawie badania materiału operacyjnego.
Cel pracy. Prównanie złośliwości raka stercza ocenione na podstawie biopsji i badania preparatów operacyjnych.
Materiał i metody. Materiał badawczy stanowiły gromadzone prospektywnie dane medyczne dotyczące kolejnych 212 chorych poddanych prostatektomii radykalnej (PR), u których raka stercza (ang. prostate cancer – PCa) rozpoznano na podstawie wielomiejscowej biopsji rdzeniowej stercza wykonanej pod kontrolą ultrasonografii przezodbytniczej (TRUScoreBx).
Wyniki. Złośliwością najczęściej rozpoznawaną na podstawie badania rdzeni tkankowych pochodzących z TRUScoreBx była złośliwość 4 i 5 w skali Gleasona (46,3%). Złośliwość określoną jako Gl.s. > 7 stwierdzono u 32 (15,2%) chorych. Z kolei na podstawie badania specymenów operacyjnych najczęściej rozpoznano pierwotnie złośliwość Gl.s. 7 (34,8%) i Gl.s. 5 (23,3%). Różnice między ocenami złośliwości określonej na podstawie badania rdzeni tkankowych (Gl.s.Bx) i ocenami złośliwości określonej na podstawie badania specymenów operacyjnych (Gl.s.PR) są statystycznie znamienne. Zgodność dotyczyła 34,3% ocen, zaś brak zgodności 65,7% ocen.
Wnioski. Nasze badanie udowadnia, że występują różnice między globalną złośliwością raka stercza (Gl.s.) określoną na podstawie oceny histopatologicznej rdzeni tkankowych pochodzących z biopsji stercza, a określoną na podstawie badania preparatów po operacji.
Summary
Introduction. Prostate cancer is diagnosed on the basis of transrectal ultrasound-guided multiple-core biopsy (TRUScoreBx) done with a tru-cut needle. One of the most important issues in prostate cancer diagnosis is estimation of its malignancy. It is defined according to Gleason score system which grades malignancy according to 5 Gleason patterns, with 1 being the least, and 5 being the most malignant. There are discrepancies between prostate cancer grading in prostate biopsy and after radical prostatectomy.
Aim. To compare prostate cancer grade after biopsy and radical prostatectomy.
Material and methods. Research material consisted of prospectively collected medical data for 212 consecutive patients who underwent radical prostatectomy (RP) at the Urology Department of the CPME, and were diagnosed with PCa based on transrectal ultrasound-guided multiple-core biopsy (TRUScoreBx).
Results. The most frequent Gleason score in TRUScoreBx was 4 and 5 (46.3%), while Gleason score > 7 was found in 32 (15.2%) patients. The most frequent Gleason score in post prostatectomy material was 7 (34.8%) and 5 (23.3%). The differences between Gleason score in TRUScoreBx and post prostatectomy material were statistically significant. Concordance was found in 34.3% whereas a lack of it in 65.7%.
Conclusions. Our study demonstrates that there are differences between the global malignancy of prostate cancer (Gl.s.) determined on the basis of histopathological examination of tissue cores obtained in prostate biopsy and examination of surgery specimens.

INTRODUCTION
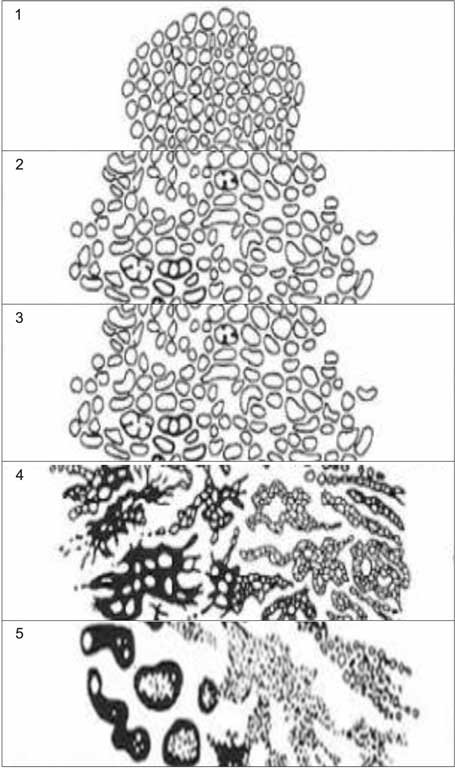
9273 prostate cancer (PCa) diagnoses were registered in Poland in 2010. Analysis of epidemiological data indicates a gradual increase in PCa incidence and PCa-associated mortality in Poland over the last decades, with mortality climbing slower than incidence (fig. 1, 2). Prostate cancer is predominantly found in the peripheral zone (70%), particularly in the apex area. 10-15% of patients develop PCa in the transitional, and 15-20% in the central zone (fig. 3) (1-3). PCa is diagnosed based on the examination of biopsy specimens, typically transrectal ultrasound guided multiple-core biopsy performed with tru-cut needle (TRUScoreBx). Finger-guided multi-core biopsy (FGcoreBx) or fine-needle aspiration multicore biopsy (FNABx) that is also a finger-guided type of biopsy are justified only in patients with clinically evident PCa that requires solely histo- or cytopathological verification, without the need to accurately determine features assessable in TRUScoreBx (4-7). The key element of PCA evaluation is malignancy assessment, i.e. its grading. The malignancy is defined with Gleason score (Gl.s.) developed by Donald Gleason (1920-2008), in common use since 1978 (8, 9). According to this system, PCa is associated with 5 Gleason patterns ranging from the least (1) to most malignant (5), differing mostly by their architecture, and to a lesser degree by the features of the cancerous cells (fig. 4) (6). When grading a tumour, the dominant (primary) pattern within a given tumour is identified, along with the next-most frequent (secondary) one, and both are assigned numerical grades. The sum of these two numbers (referred to as Gleason numbers) reflects the cancer’s global malignancy, and is known as Gleason sum or Gleason score (Gl.s.), e.g. Gl.s. 7 (Gl.n. 4 + Gl.n. 3) means that 4 is the predominant malignancy pattern, with 3 being the next-most common one, with a reverse sequence of numbers (3 + 4) being prognostically more favourable. Discrepancies in the malignancy scores identified on the basis of tissue core samples and surgical specimens (removed prostate) have already been widely researched (10), with numerous urological studies worldwide devoted to the accuracy of grading. Both intraobserver and interobserver variability have been determined to be of substantial significance here (11-13). Polish urological literature, however, has so far not included publications on this subject, except for studies by the author of this paper (14-17).

Fig. 1. Incidence of prostate cancer and prostate cancer-related mortality in Poland between 2001-2010. Data according to www.onkologia.org.pl
Fig. 2. Prostate cancer incidence rate and mortality rate in Poland between 2001-2010. Data according to www.onkologia.org.pl
Fig. 3. McNeal’s zonal anatomy of the prostate: a – transverse section, b – longitudinal section
TZ – transition zone; PZ – peripheral zone; AFS – anterior fibromuscular stroma; CZ – central zone; U – urethra; ED – ejaculatory ducts (1)

Fig. 4. The 5 malignancy patterns in Gleason system of prostate cancer grading (6)
AIM
To compare prostate cancer grade after biopsy and radical prostatectomy.
MATERIAL AND METHODS
Research material consisted of prospectively collected medical data for 212 consecutive patients who underwent radical prostatectomy (RP) at the Urology Department of CPME, diagnosed with prostate cancer (PCa) based on transrectal ultrasound-guided multiple-core biopsy (TRUScoreBx). The tissue samples collected in prostate biopsy and the RP specimens were consecutively evaluated by the same experienced pathologist.
RESULTS
Comparison of prostate cancer grades based on histopathological examination of tissue cores from TRUScoreBx and of removed prostate and seminal vesicles specimens
The most common malignancy identified by the urologic pathologist in TRUScoreBx (UP-11) was Gleason score 4 and 5 (46.7%). Malignancy grade identified as Gl.s. > 7 was found in 32 patients (15.2%). The scores most frequently identified in radical prostatectomy specimens were Gleason scores 7 (34.8%) and 5 (23.3%).
Malignancy scores based on tissue core evaluation and examination of RP specimens (UP-11) are shown in table 1. The data were tested with Stuart-Maxwell test of marginal homogeneity, showing the discrepancies between malignancy scores based on examination of multiple core biopsy (Gl.s.Bx) samples and postoperative specimens (Gl.s.RP) to be statistically significant (p < 0.0001), thus evidencing a significant lack of concordance to exist between the scores. Similarly, kappa coefficient calculated for these scores (κ = 0.20) showed a considerable discrepancy between the scores (with κ = 1.0 there is full concordance = 100%, whereas κ = 0.20 means that statistically there is concordance in one in five cases). Hence, concordance was determined for 34.3% of the scores, and a lack thereof for 65.7% (tab. 2).
Tab. 1. Gleason scores assigned by the urologic pathologist (UP-11) based on multiple-core biopsy samples (Gl.s.Bx) and on radical prostatectomy specimens (Gl.s.RP)
| | Gl.s.Bx | Gl.s.RP |
| Gl.s. | Number (N) | Percentage (%) | Number (N) | Percentage (%) |
| 2 | 3 | 1.43 | 77.61 | 0 | 0 | 49.99 |
| 3 | 7 | 3.33 | 7 | 3.33 |
| 4 | 53 | 25.24 | 18 | 8.57 |
| 5 | 57 | 27.14 | 49 | 23.33 |
| 6 | 43 | 20.48 | 31 | 14.76 |
| 7 | 32 | 15.24 | 15.24 | 73 | 34.76 | 34.76 |
| 8 | 12 | 5.71 | 7.14 | 18 | 8.57 | 15.24 |
| 9 | 2 | 0.95 | 13 | 6.19 |
| 10 | 1 | 0.48 | 1 | 0.48 |
| Total | 210 | 100 | | 210 | 100 | |
| Data for 210 patients, comprising 99% of the cohort |
Tab. 2. Comparison of Gleason scores assigned by the urologic pathologist (UP-11) based on multiple-core biopsy samples (Gl.s.Bx) and on radical prostatectomy specimens (Gl.s.PR)
| Gl.s. | Number (N) | Percentage (%) | |
| Gl.s.Bx = Gl.s.PR | 72 | 34.29 | 34.29 | Concordance |
| Gl.s.Bx > Gl.s.PR | 19 | 9.05 | 65.71 | Lack of concordance |
| Gl.s.Bx < Gl.s.PR | 119 | 56.67 |
| Data for 210 patients, comprising 99% of the cohort |
The comparison of PCa scores identified by the urologic pathologist (UP-11) based on multiple core biopsies (Gl.s.Bx) and on examination of RP specimens (Gl.s.RP) has been collectively presented in table 3.
Tab. 3. Concordance of Gleason scores assigned by the urologic pathologist (UP-11) based on multiple-core biopsy samples (Gl.s.Bx) and on radical prostatectomy specimens (Gl.s.PR): the number of concordant scores (Gl.s.Bx = Gl.s.RP) is shown in coloured fields, with the number of undergraded Gleason scores shown to the right (Gl.s.Bx < Gl.s.PR), and the number of overgraded Gleason scores (Gl.s.Bx > Gl.s.PR) shown to the left
| Gl.s.Bx | Gl.s.RP | Total |
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 2 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 3 |
| 3 | 0 | 2 | 0 | 3 | 0 | 1 | 1 | 0 | 0 | 7 |
| 4 | 0 | 1 | 14 | 20 | 7 | 10 | 1 | 0 | 0 | 53 |
| 5 | 0 | 0 | 2 | 17 | 13 | 21 | 2 | 2 | 0 | 57 |
| 6 | 0 | 2 | 1 | 7 | 10 | 15 | 5 | 3 | 0 | 43 |
| 7 | 0 | 0 | 0 | 1 | 0 | 23 | 4 | 4 | 0 | 32 |
| 8 | 0 | 1 | 0 | 0 | 0 | 2 | 5 | 4 | 0 | 12 |
| 9 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 2 |
| 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| Total | 0 | 7 | 18 | 49 | 31 | 73 | 18 | 13 | 1 | 210 |
| Data for 210 patients, comprising 99% of the cohort |
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
24 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
59 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
119 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 28 zł
Piśmiennictwo
1. McNeal JE: Origin and development of carcinoma in the prostate. Cancer 1969; 23(1): 24-34.
2. Byar D, Mostofi F: Carcinoma of the prostate: Prognostic evaluation of certain pathologic features in 208 radical prostatectomies. Cancer 1972; 30(1): 5-13.
3. Epstein JI, Walsh PC, Carmichael M et al.: Pathologic and clinical findings to predict tumor extent of nonpalpable (stage T1c) prostate cancer. JAMA 1994; 271(5): 368-374.
4. Antoniewicz AA: Jak poprawić jakość biopsji stercza? [W:] Antoniewicz AA (red.): Biopsja stercza. Komitet Edukacji PTU Top Kurier, Toruń 2002; tom I: 73-81.
5. Bostwick DG, Meiers I: Prostate biopsy and optimization of cancer yield. Eur Urol 2006; 49(3): 415-417.
6. Gleason DF, Mellinger GT. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. J Urol 1974; 111: 58-64.
7. Ficarra V, Novella G, Novara G et al.: The potential impact of prostate volume in the planning of optimal number of cores in the systematic transperineal prostate biopsy. Eur Urol 2005; 48: 932-937.
8. Schmidt C: Gleason Scoring system Faces Change and Debate. J Natl Cancer Inst 2009 May 6; 101(9): 622-629.
9. Phillips JL, Sinha AA: Patterns, Art, and Context: Donald Floyd Gleason and the Development of the Gleason Grading System. Urology 2009; 74(3): 497-503.
10. Dobruch J, Borówka A, Grotthuss G et al.: Comparison of clinical and pathological stage and grade of prostate cancer. Urol Pol 2007; 60: 30-37.
11. Griffiths DFR, Melia J, McWilliam LJU et al.: A study of Gleason score interpretation in different groups of UK pathologists; techniques for improving reproducibility. Histopathology 2006; 48: 655-662.
12. Montironi R, Mazzuccheli R, Scarpelli M et al.: Gleason grading of prostate cancer in needle biopsies or radical prostatectomy specimens: contemporary approach, current clinical significance and sources of pathology discrepancies. BJUInt 2005; 95: 1146-1152.
13. Brimo F, Schultz L, Epstain J: The value of mandatory second opinion pathology review of prostate needle biopsy interpretation before radical prostatectomy. J Urol 2010; 184: 126-130.
14. Nyk Ł: Sprawozdanie z 2. Spotkania Europejskiego Towarzystwa Urologicznego Europy Północno-Wschodniej. Przegląd Urologiczny 2008; 6(52).
15. Nyk Ł, Dzik T, Dobruch J et al.: Badanie stopnia rozbieżności między pierwszą i powtórną oceną cech onkologicznych raka stercza dokonaną przez tego samego patomorfologa. Urologia Polska 2008; 61 (supl. 1).
16. Nyk Ł, Dzik T, Wysocki M et al.: Study on interobserver variability of prostate cancer grading. European Urology Suppl. 2010; 9(6): 656.
17. Nyk Ł, Dzik T, Wysocki M et al.: Intra and interobserver variability in diagnosing clinically important variables after radical prostatectomy: positive surgical margins (PSM), extracaopsular extension (ECE), seminal vesicle invasion (SVI). European Urology Suppl 2011; 10(9): 629.
18. Cohen M, Hanley R, Kurteva T et al.: Comparing the Gleason Prostate Biopsy and Gleason Prostatectomy Grading System: The Lahey Clinic Medical Center Experience and an International Meta-Analysis. Eur Urol 2008; 54: 371-381.
19. Grossfeld GD, Chang JJ, Broering JM et al.: Under staging and under grading in a contemporary series of patients undergoing radical prostatectomy: results from the Cancer of the Prostate Strategic Urologic Research Endeavor database. J Urol 2001; 165: 851-856.
20. Derweesh IH, Kupelian PA, Zippe C et al.: Continuing trends in pathological stage migration in radical prostatectomy specimens. Urol Oncol 2004; 22: 300-306.
21. DiMarco DS, Blute ML, Zincke H et al.: Multivariate models to predict clinically important outcomes at prostatectomy for patients with organ-confined disease and needle biopsy Gleason scores of 6 or less. Urol Oncol 2003; 21: 439-446.
22. Steinberg DM, Sauvageot J, Piantadosi S, Epstein JI: Correlation of prostate needle biopsy and radical prostatectomy Gleason grade in academic and community settings. Am J Surg Pathol 1997; 21: 566-576.
23. King CR: Patterns of prostate cancer biopsy grading: trends and clinical implications. Int J Cancer 2000; 90: 305-311.
24. Johnstone PA, Riffenburgh R, Saunders EL, Willison FW: Grading inaccuracies in diagnostic biopsies revealing prostatic adenocarcinoma: implications for definitive radiation therapy. Int J Radiation Oncology, Biology, Physics 1995; 32: 479-482.
25. Robein JA: Results of radical prostatectomies for cancer: a retrospective multicenter study on 918 cases. Journal d Urologie 1994; 100: 121-127.
26. Ogura Y, Sakata Y, Wakita T et al.: Treatment results of radical prostatectomy in clinical stage B and C prostate cancer: comparison of the neoadjuvant therapy group versus the surgery group; retrospective analysis of 80 cases. Acta Urologica Japonia 2003; 49.
27. Montironi R, Mazzuccheli R, Scarpelli M et al.: Gleason grading of prostate cancer in needle biopsies or radical prostatectomy specimens: contemporary approach, current clinical significance and sources of pathology discrepancies. BJU Int 2005; 95: 1146-1152.
28. Carlson GD, Calvanese CB, Kahane H, Epstein JI: Accuracy of biopsy Gleason scores from a large uropathology laboratory: use of a diagnostic protocol to minimize observer variability. Urology 1998; 51: 525-529.
29. Brimo F, Schultz L, Epstain J: The Value of mandatory second opinion pathology review of prostate needle biopsy interpretation before radical prostatectomy. J Urol 2010; 184: 126-130.
30. Melia J, Moseley R, Ball RY et al.: A UK based investigation of inter- and intra- observer reproducibility of Gleason grading o prostatic biopsies. Histopathology 2006 May; 48(6): 644-654.
31. William C, Allsbrook WC Jr, Johnson MH et al.: Interobserver reproducibility of Gleason grading of prostatic carcinoma: general pathologists. Hum Pathol 2001; 32: 81-88.
32. Svanholom H, Mygind H: Prostatic carcinoma. Reproducibility of histologic grading. Acta Path Microbiol Immunol Scand 1985; 93; 67-71.
33. Ozdamar SO, Sarikaya S, Yildiz L et al.: Intraobserver and interobserver reproducibility of WHO and Gleason histologic grading system in prostatic adenocarcinomas. Int Urol Nephrol 1996; 28: 73-77.
34. McLean M, Srigley J, Banerjee D et al.: Interobserver variation in prostate cancer scoring: are there implications for the design of clinical trials and treatment strategies? Clin Oncol 1997; 9: 222-225.
35. di Loreto C, Fitzpatrick B, Underhill S et al.: Correlation between visual clues, objective histologic features, and interobserver agreement in prostate cancer. Am J Clin Pathol 1991; 96: 70-75.
36. de las Morenas A, Siroky MB, Merriam J et al.: Prostatic adenocarcinoma: reproducibility and correlation with clinical stages of four grading systems. Hum Pathol 1988; 19: 595-597.