© Borgis - Postępy Nauk Medycznych 4/2017, s. 206-209
*Piotr Trojanowski1, Krzysztof Pyra2, Michał Sojka2, Michał Górnik2, Agnieszka Trojanowska3, Janusz Klatka1, Tomasz Jargiełło2
Incidence of the peroneal magnus artery in patients planned for free fibula transfer
Częstość występowania dominującej tętnicy strzałkowej u chorych planowanych do przeszczepu wolnego płata strzałkowego
1Department of Otolaryngology and Head and Neck Surgery, Medical University in Lublin
Head of Department: Professor Janusz Klatka, MD, PhD
2Department of Interventional Radiology and Neuroradiology, Medical University in Lublin
Head of Department: Professor Małgorzata Szczerbo-Trojanowska, MD, PhD
3Department of Radiology and Nuclear Medicine, Medical University in Lublin
Head of Department: Professor Andrzej Drop, MD, PhD
Streszczenie
Wstęp. Wolny płat strzałkowy jest podstawowym płatem wykorzystywanym do rekonstrukcji żuchwy. Występuje wiele odmian anatomicznych tętnic goleni i wiedza na ten temat ma bardzo istotne znaczenia kliniczne. Chirurdzy przeprowadzający zabiegi rekonstrukcyjne przy użyciu wolnego płata strzałkowego u chorych z dominującą tętnicą strzałkową (ang. peroneal magnus artery) powinni brać pod uwagę możliwość powikłań niedokrwiennych związanych z pobraniem tej tętnicy do przeszczepu.
Cel pracy. Celem prcy jest przedstawienie włanych doświadczeń z wykonania 65 wolnych przeszepów strzałkowych z podkreśleniem znaczenia odmiany anatomicznej w postaci dominującej tętnicy strzałkowej.
Materiał i metody. Sześćdziesięciu pięciu chorych z Kliniki Otolaryngologii UM w Lublinie zostało zaplanowanych do zabiegu rekonstrukcji żuchwy z powodu ubytku po resekcji raka płaskonabłonkowego (ang. squamous cell cancer). W badaniu fizykalnym u wszystkich chorych oceniono tętno na stopie jako prawidłowe. Przed zabiegiem chirurgicznym u chorych wykonano angiografię tętnic kończyn dolnych. Po wybiórczym podaniu 15 ml środka cieniującego do tętnic podkolanowych w obu kończynach uwidoczniono tętnice goleni.
Wyniki. Spośród 65 chorych u dwóch w badaniu angiograficznym stwierdzono rozległe zmiany miażdżycowe pod postacią licznych przewężeń światła i odcinkowych niedrożności. U kolejnych dwóch chorych – 48-letniego mężczyzny w obu kończynach i 64-letniej kobiety w lewej kończynie dolnej – wykryto anomalię naczyniową tętnicy goleni. U obu chorych stwierdzono hypoplastyczne tętnice piszczelowe przednie i tylne. Rozpoznano u obu chorych wariant anatomiczny w postaci dominującej tętnicy strzałkowej.
Wnioski. Wykorzystanie wolnego płata strzałkowego do rekonstrukcji żuchwy i ubytków w innych obszarach anatomicznych jest bardzo często wykorzystywane. Chirurdzy wykonujący operacje rekonstrukcyjne z użyciem tego płata powinni brać pod uwagę ewentualne wady naczyniowe w obrębie goleni. Nawet u chorych z zachowanym prawidłowym tętnem na stopie przed pobraniem wolnego płata strzałkowego powinna być wykonana angiografia tej kończyny, by uniknąć ewentualnych powikłań niedokrwiennych w obrębie kończyny.
Summary
Introduction. Free fibula flap is recognised as the workhorse ?ap for mandible reconstruction. There are several anatomical variations of the crural arteries and its branches and knowledge of these has important clinical implications for fibula ?ap harvest. Surgeons performing free fibula flap transfer in patients with dominating peroneal artery should be aware of high risk of leg ischaemic complication.
Aim. The aim of this study was to report our experience on 65 free fibula ?aps, highlighting a type of anatomical variation of the peroneal artery – peroneal magnus artery in patients undergoing osteocutaneous free fibula ?ap transfer for mandible reconstruction.
Material and methods. Sixty-five patients from the Department of Otolaryngology and Head and Neck Surgery Medical University in Lublin were planed to free osteocutaneous fibula ?ap harvest for the mandibular reconstruction due to the defects after oncological resections (squamous cell cancers). Patients underwent clinical examination, they all had normal distal pulse. Before operations angiography of lower extremities was performed in all patients. After selective injection of 15 ml of contrast media to the popliteal artery in both legs crural arteries were visualised.
Results. Out of 65 patients, in two, angiography reviled diffuse arteriosclerotic changes in all tree crural arteries. In two next patients one 48y old male in both extremities and in one 64y old female in left lower extremity an anatomical anomaly of peroneal artery was detected. In both patients anterior and posterior tibial arteries were hypoplastic. Anatomical variant, the peroneal magnus artery was diagnosed.
Conclusions. The free fibula ?ap is the gold standard for microsurgical reconstruction of bone defects involving the mandible and other anatomical regions. Surgeons conducting reconstructive surgery should be aware of possible vascular anomalies of crural arteries. Even in patients with normal distal pulses, before harvesting of fibula flap angiographic investigations should be considered to avoid foot ischaemia at the donor site.

Introduction
The introduction of microsurgical flaps for osseous reconstruction had a major role in the clinical practice. The free fibula flap was first described by Taylor et al. (1) in 1975 for the reconstruction of post-traumatic bone defects where an osteocutaneous fibula ?ap for mandibular reconstruction was developed by Hidalgo in 1991 (2). From that time the free fibula flap is recognised as the workhorse ?ap for mandible reconstruction. The length of the bone and the thin, pliable, cutaneous island allow extensive reconstruction not only of the mandible but also of the surrounding soft tissues. The fibula flap offers usually 25 cm or more of straight cortical bone and a vascular pedicle up to 12-15 cm length, with perforators of the adequate caliber to supply the skin island (3-5).
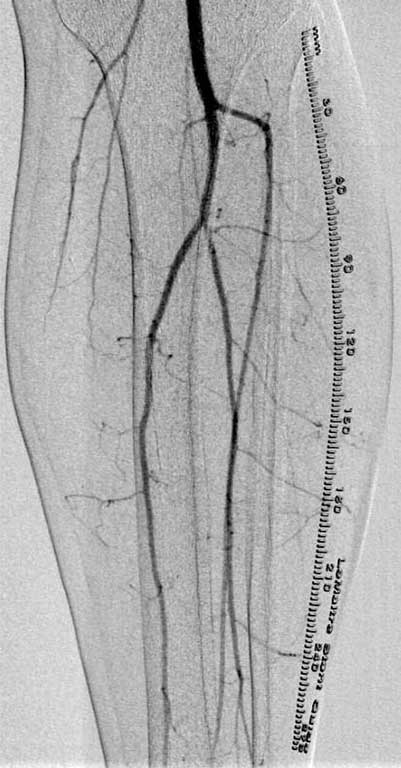
Crural vascularisation originates from the popliteal artery, which crosses the popliteal fossa and gives origin to the Anterior Tibial Artery (ATA), and the tibio-peroneal trunk that gives rise to the Posterior Tibial Artery (PTA) and the Peroneal Artery (PA) (fig. 1) (6). There are several anatomical variations of the crural arteries and its branches, and knowledge of these has important clinical implications for free fibula ?ap harvest. As the number of patients with microsurgical fibula transfers increase every year surgeons are more often confronted with anatomical variants that may complicate the operating plans.
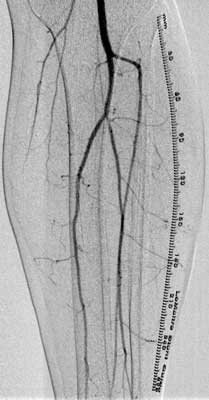
Fig. 1. Angiography of the crural arteries. Type A – normal division of the popliteal artery
Aim
The aim of this study was to report our experience on 65 free fibula ?aps, highlighting a type of anatomical variation of the peroneal artery – peroneal magnus artery in patients undergoing osteocutaneous free fibula ?ap for mandible reconstruction.
Material and methods
Sixty-five patients from the Department of Otolaryngology and Head and Neck Surgery Medical University in Lublin were planed to free osteocutaneous fibula ?ap harvest for the mandibular reconstruction of defects after oncological resection (squamous cell cancer). There were 47 male (72%) with a mean age of 53 years and 19 female (28%) with a mean age of 57 years. Patients underwent clinical examination, they all had normal distal pulse. Before surgery patients were referred to angiography of lower extremities. Angiography of the lower legs was performed in the Department of Interventional Radiology and Neuroradiology Medical University in Lublin. When the harvest of the left fibula flap was planed access for angiography was from the right femoral artery. In patients who were prepared for reconstruction with the use of the right fibula flap angiography was performed with the puncture of the left femoral artery.
Under local anaesthesia using Seldinger technique a puncture of the common femoral artery was performed. After puncture of the femoral artery in the groin the 5F catheter was introduced to the iliac artery and then to the contralateral femoral artery. Then catheter was selectively guided into the popliteal artery. Angiography was performed with a use of 20 ml of contrast media (Visipaque 350, GE HealthCare). The catheter was then placed in the ipsilateral iliac artery and angiography was carried in the same manner. Crural arteries and the foot arteries were visualised. After angiography the patient remained in bed for 24 h.
Results
In all patients diagnostic angiography was obtained.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
24 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
59 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
119 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 28 zł
Piśmiennictwo
1. Taylor GI, Miller GD, Ham FJ: The free vascularised bone graft: a clinical extension of microvascular techniques. Plast Reconstr Surg 1975; 55: 533-534.
2. Hidalgo DA: Fibula free ?ap: a new method of mandible reconstruction. Plast Reconstr Surg 1989; 84: 71-79.
3. Wei FC, Chen HC, Chuang CC, Noordhoff MS: Fibula osteoseptocutaneous ?ap: anatomic study and clinical application. Plast Reconstr Surg 1986; 78: 191-200.
4. Cross L, Hall J, Howdieshell TR et al.: Clinical anatomy of the popliteal blood vessels. Clin Anat 2000; 13: 347-353.
5. Anand R, Mourouzis R, Wilbourn M et al.: An unreported variation of the course of peroneal artery during fibula ?ap harvest. Brit J Oral Maxillofac Surg 2007; 45: 588-589.
6. Jones SA, Roberts DC, Clarke NM: Popliteal vasculature injuries in paediatric trauma patients. Injury 2012; 43: 1709-1711.
7. Lippert H, Pabst R: Arterial variations in man: classification and frequency. J. F. Bergmann Verlag, Munchen 1985.
8. Kim D, Orro DE, Skillman JJ: Surgical significance of popliteal arterial variants – a unified angiographic classification. Ann Surg 1989; 210: 776-781.
9. Anand R, Mourouzis R, Wilbourn M et al.: An unreported variation of the course of peroneal artery during fibula ?ap harvest. Brit J Oral Maxillofac Surg 2007; 45: 588-589.
10. Young DM, Trabulsy PP, Anthony JP: The need for preoperative leg angiography in fibula free ?aps. J Reconstr Microsurg 1994; 10: 283-287.
11. Abou-Foul AK, Borumandi F: Anatomical variants of lower limb vasculature and implications for free fibula flap: Systematic review and critical analysis. Microsurgery 2016; 36: 165-172.
12. Disa JJ, Cordeiro PG: The current role of preoperative arteriography in free fibula flaps. Plast Reconstr Surg 1998; 102: 1083-1088.
13. Oxford L, Ducic Y: Use of fibula-free tissue transfer with preoperative 2-vessel runoff to the lower extremity. Arch Facial Plast Surg 2005; 7: 261-265.
14. Young DM, Trabulsy PP, Anthony JP: The need for preoperative leg angiography in fibula free flaps. J Reconstr Microsurg 1994; 10: 283-287.
15. Lorenz RR, Esclamado R: Preoperative magnetic resonance angiography in fibular-free flap reconstruction of head and neck defects. Head Neck 2001; 23: 844-850.
16. Lutz BS, Wei FC, Ng SH et al.: Routine donor leg angiography before vascularised free fibula transplantation is not necessary: a prospective study in 120 clinical cases. Plast Reconstr Surg 1999; 103: 121-127.
17. Lohan DG, Tomasian A, Krishnam M et al.: MR angiography of lower extremities at 3 T: pre-surgical planning of fibular free flap transfer for facial reconstruction. AJR 2008; 190: 770-776.
18. Rosson GD, Singh NK: Devascularising complications of free fibula harvest: peronea arteria magna. J Reconstr Microsurg 2005; 21: 533-538.