Karolina Raczkowska-ŇĀabuda, Anna Gorzelnik, Jolanta Jadczyszyn, Monika JabŇāoŇĄska-Jesionowska, *Lidia Zawadzka-GŇāos
Seasonality in the incidence of deep neck space infections in children hospitalized in the Department of Pediatric Otolaryngology of the Medical University of Warsaw
SezonowoŇõńá ropni przestrzeni gŇāńôbokich szyi u dzieci hospitalizowanych w Klinice Otolaryngologii Dziecińôcej Warszawskiego Uniwersytetu Medycznego
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Associate Professor Lidia Zawadzka-GŇāos, MD, PhD
Streszczenie
Wstńôp. Ropnie przestrzeni gŇāńôbokich szyi niezmiennie stanowińÖ wyzwanie diagnostyczne i terapeutyczne dla laryngolog√≥w dziecińôcych. Brak sp√≥jnoŇõci w nazewnictwie polskim wzglńôdem anglosaskiego dodatkowo komplikuje problem rozpoznania. Szerokie spektrum objaw√≥w i skrajnie r√≥Ňľna prezentacja kliniczna pacjent√≥w op√≥ŇļniajńÖ wdroŇľenie odpowiedniego leczenia.
Cel pracy. Celem pracy byŇāa analiza wybranych charakterystyk epidemiologicznych oraz klinicznych ropni przestrzeni gŇāńôbokich szyi u dzieci, takich jak sezonowoŇõńá zachorowaŇĄ, trudnoŇõci diagnostyczne oraz dostńôpne metod leczenia.
MateriaŇā i metody. AnalizńÖ retrospektywnńÖ objńôto dane uzyskane z dokumentacji medycznej chorych leczonych z powodu zapalenia tkanek gŇāńôbokich szyi w latach 2013–2018 w Klinice Otolaryngologii Dziecińôcej Warszawskiego Uniwersytetu Medycznego. W badaniu zwr√≥cono uwagńô na wiek i pŇāeńá dzieci, metody diagnostyczne, florńô bakteryjnńÖ posiewu z ropnia, ale szczeg√≥lnie skoncentrowano sińô na sezonowoŇõci wystńôpowania ropni gŇāńôbokich przestrzeni szyi u dzieci. Wykonano analizńô statystycznńÖ, wyznaczajńÖc wskaŇļnik sezonowoŇõci dla pozyskanych danych oraz symulacjńô prognozy wystńôpowania czynnika dla Ňõredniej ruchomej o okresie odniesienia wynoszńÖcym 2 miesińÖce. W kolejnym kroku przyjńôto tezńô o dyskretnym rozkŇāadzie jednostajnym danych i wykonano testowanie hipotez statystycznych metodńÖ Monte Carlo przy poziomie ufnoŇõci α = 1%. PrawdopodobieŇĄstwo wystńÖpienia 9 zachorowaŇĄ w jednym miesińÖcu wyznaczono na podstawie rozkŇāadu dwumianowego.
Wyniki. W latach 2013–2018 przyjńôto 23 dzieci z ropniem przestrzeni przygardŇāowej i zagardŇāowej, z czego dziewińôcioro w grudniu. W analizowanej grupie obserwuje sińô nieznacznńÖ przewagńô w liczbie chŇāopc√≥w nad dziewczynkami M:K = 1,3:1. Ňöredni wiek pacjent√≥w wynosiŇā 3 lata i 5 miesińôcy. Wszystkie dzieci przed rozpoznaniem ropnia przestrzeni gŇāńôbokich szyi przeszŇāy infekcjńô g√≥rnych dr√≥g oddechowych. U wszystkich pacjent√≥w stwierdzono powińôkszone wńôzŇāy chŇāonne szyi. WskaŇļnik sezonowoŇõci dla miesińÖca grudnia byŇā ponad 3-krotnie wyŇľszy niŇľ dla marca i wynosiŇā 4,696. Przyjńôto hipotezńô o dyskretnym jednostajnym rozkŇāadzie danych (H0) przy poziomie ufnoŇõci α = 1%. Przy pomocy rozkŇāadu jednomianowego uzyskano prawdopodobieŇĄstwo wystńÖpienia 9 przypadk√≥w w jednym miesińÖcu wynoszńÖce P(9) = 0,000141. StńÖd odrzucenie H0 nastńôpuje z bŇāńôdem 0,17% < 1%.
Wnioski. W Polsce przyjńôcie dziecka z rozpoznaniem ropnia przestrzeni przygardŇāowej lub zagardŇāowej jest najbardziej prawdopodobne p√≥ŇļnńÖ jesienińÖ – w listopadzie i grudniu. ZakaŇľenia ropne tkanek gŇāńôbokich szyi u dzieci sńÖ powikŇāaniem infekcji g√≥rnych dr√≥g oddechowych. PowyŇľsze infekcje sńÖ trudne do rozpoznania ze wzglńôdu na brak patognomonicznych objaw√≥w. Leczenie wyŇāńÖcznie zachowawcze stanowi alternatywńô dla drenaŇľu chirurgicznego u pacjent√≥w stabilnych z ropniem maŇāych rozmiar√≥w pod warunkiem normalizacji wykŇāadnik√≥w stanu zapalnego i poprawie stanu klinicznego pacjenta.
Summary
Introduction. Parapharyngeal abscesses are invariably a diagnostic and therapeutic challenge for pediatric otolaryngologists. The lack of consistency in the Polish nomenclature in relation to the English terms additionally complicates the problem. The wide spectrum of signs and symptoms, as well as an extremely heterogenous clinical presentation of the disease, also delay the implementation of appropriate treatment.
Aim. The aim of the study was to analyze selected epidemiological and clinical characteristics of the parapharyngeal abscesses in children, such as the seasonality in the incidence, diagnostic difficulties, and available treatment methods.
Material and Methods. A retrospective analysis was conducted on data obtained from medical histories of patients treated for deep neck space infections in the years 2013–2018 in the Department of Pediatric Otolaryngology of the Medical University of Warsaw. The study analyzed the age and sex of the children, as well as diagnostic methods and bacterial culture tests of the abscess. Particular attention was drawn to the seasonality in the incidence of the parapharyngeal abscesses in children. A statistical analysis was performed and seasonality index for the data was calculated, and a simulation of the prognosis of the occurrence of the factor for a moving average with a reference period of 2 months was performed. Next, the thesis on the discrete uniform data distribution was adopted, and Monte Carlo method was used for testing of the hypothesis. The significance level was α = 1%. The probability of 9 cases in one month was calculated based on the binomial distribution.
Results. In the years 2013–2018, 23 children with parapharyngeal and retropharyngeal abscesses were admitted to the Department, 9 of which were admitted in December. In the analyzed group, a slight advantage in the number of boys was observed, with the male to female ratio being M:F = 1.3:1. Mean age of the patients was 3 years and 5 months. All the children had undergone an upper respiratory tract infection before being diagnosed with a deep neck space infection. All the patients had enlarged neck lymph nodes. The seasonality index for December was over 3 times higher than for March and accounted 4.696. The hypothesis on the discrete uniform data distribution was adopted (H0). The significance level was α = 1%. Based on monomial distribution, the probability of the occurrence of 9 cases in one month was calculated and amounted P(9) = 0.000141. Hence, the rejection of H0 occurs with an error of 0.17% < 1%.
Conclusions. In Poland, the admission of a child diagnosed with a retropharyngeal or parapharyngeal abscess is most likely in late autumn – in November and December. Purulent deep neck space infections in children are a complication of upper respiratory tract infections. Deep neck space infections are difficult to diagnose due to the lack of pathognomonic signs and symptoms. The conservative treatment is an alternative to the surgical drainage in stable patients with small-size abscesses under the conditions of normalization of inflammatory marker levels and improvement of the general condition of the patient.
Introduction
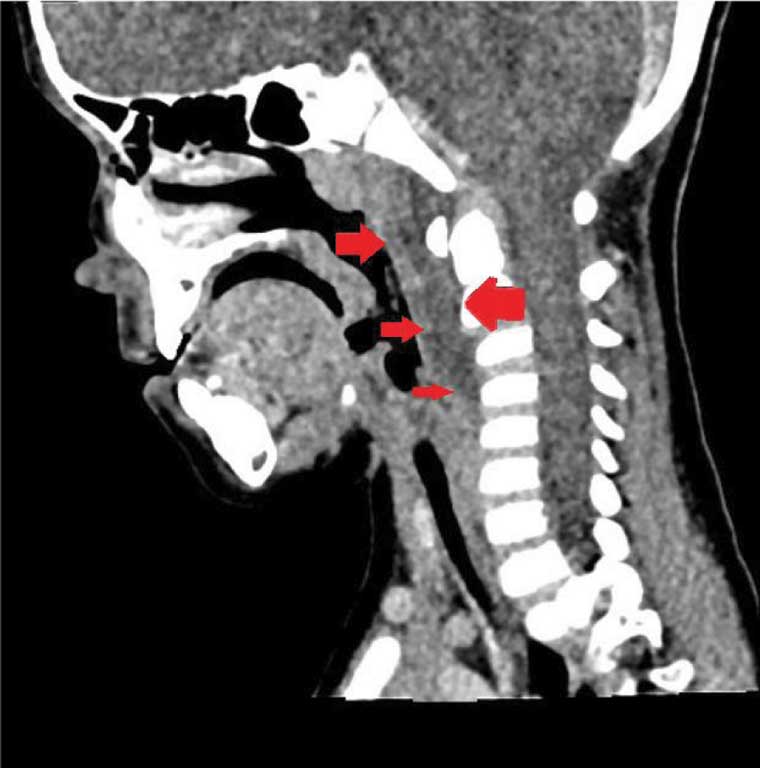
It may seem that in the era of antibiotic therapy, deep neck space infections occur incidentally. Indeed, the disease is rare, although it has always been present in the practice of a pediatric laryngologist. It is still a life-threatening condition which requires hospital treatment. Due to the lack of patognomonic signs, as well as a broad spectrum of symptoms reported by the patients, correct diagnosis is a problem until it is visualized in an imaging study – usually CT (fig. 1, 2) or US. The seasonality in the admission of the patients with this diagnosis is noteworthy.

Fig. 1. Computed tomography scan of a boy with a left parapharyngeal abscess
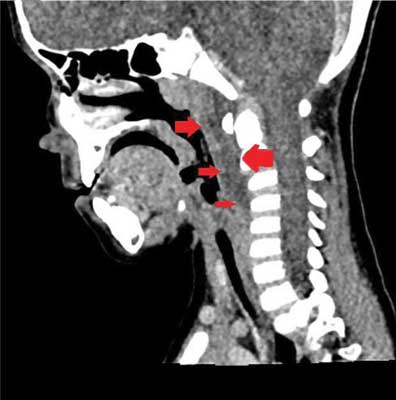
Fig. 2. Computed tomography scan of a boy with a retropharyngeal abscess
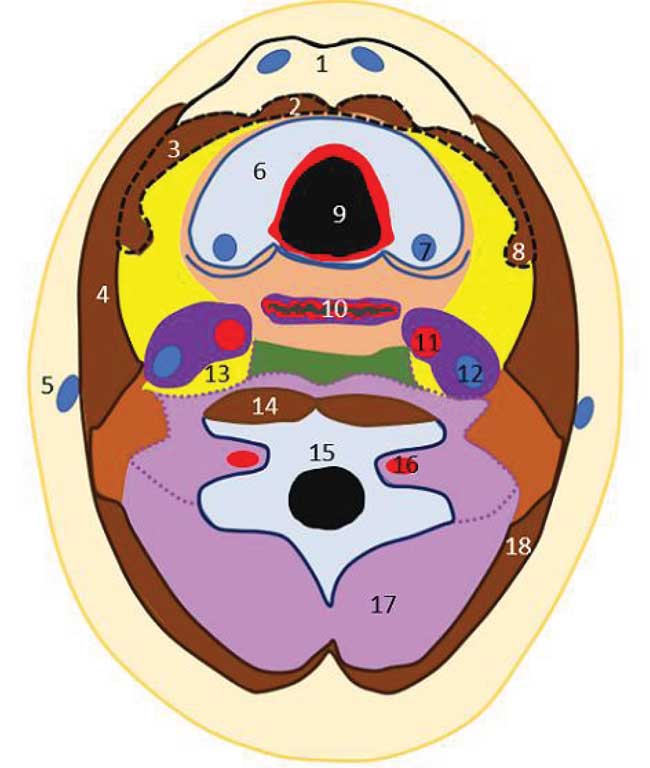
The diagnostic difficulties related to parapharyngeal abscesses are further complicated by linguistic impediments – there are fundamental discrepancies as to the anatomical nomenclature and the descriptions of the boundaries of the parapharyngeal space. The majority of the Polish researchers tend to use the “classical” nomenclature for the neck fascial spaces. Hence the division into superficial, pretracheal, and prevertebral fascia (fig. 3).
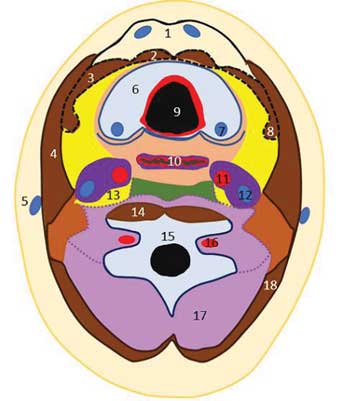
Fig. 3. The “classical” nomenclature of the neck fascial spaces:
Solid line – superficial fascia. Dashed line – pretracheal fascia. Dotted line – prevertebral fascia.
1 – anterior jugular veins; 2 – sternothyroid muscle; 3 – sternohyoid muscle; 4 – sternocleidomastoid muscle; 5 – external jugular vein; 6 – thyroid gland; 7 – parathyroid glands; 8 – sternohyoid muscle; 9 – larynx; 10 – eosophagus; 11 – internal carotid artery; 12 – internal jugular vein; 13 – sympathetic trunk; 14 – longus colli muscle; 15 – cervical vertebra; 16 – vertebral artery; 17 – nuchal muscles; 18 – trapezoid muscle
The anterior cervical space is contained between the superficial and pretracheal fascia, and the middle cervical space is contained between the pretracheal and prevertebral fascia. The anterior part of the parapharyngeal space is limited from the lateral side by the pterygoid muscle, from the medial side – by the pharynx, from the posterior side – by the muscles surrounding the styloid process (stylohyoid muscle, styloglossus muscle, and stylomandibular muscle). It is an upward extension of the middle cervical space. The posterior part of the parapharyngeal space is limited from the posterior side by the prevertebral fascia, from the medial side – by the pharyngeal wall (its extension being the retropharyngeal space), from the lateral side – by the deep lobe of the parotid gland, and from the anterior side – by the muscles surrounding the styloid process. The structures contained in the carotid sheath extend upwards in the posterior part of the parapharyngeal space.
Retropharyngeal space extends from the base of skull to the tracheal bifurcation in the mediastinum. It is contained in the midline of the neck, posterior to the posterior pharyngeal wall. Prevertebral fascia separates it from the spine. This space contains several lymph nodes, including the nodes of Henle or the nodes of Gilette (1-6). English literature suggests a different division of the cervical spaces, and consequently, of the boundaries of the parapharyngeal space. The matter is further complicated by the Polish radiology textbooks that had been translated from English, mixing these two approaches.
Inflammatory infiltrates and abscesses of these spaces are the result of the lack of treatment or delayed treatment of the upper respiratory tract: pharyngitis, tonsillitis, sinusitis, otitis media, and otitis externa (5, 7). The gold standard for management in case of parapharyngeal abscesses is broad spectrum antibiotic therapy and surgical drainage with external incisions or surgical drainage throughout the oral cavity (4, 5).
Aim
The aim of the study was to analyze selected epidemiological and clinical characteristics of the parapharyngeal abscesses in children, such as the seasonality in the incidence, diagnostic difficulties, and available treatment methods.
Material and methods
A retrospective analysis was conducted on data obtained from medical histories of patients treated for deep neck space infections from January 2013 to February 2018 in the Department of Pediatric Otolaryngology of the Medical University of Warsaw. The analysis excluded patients who developed inflammatory infiltration of the neck in the form of a reddened, fluctuant lesion, thus suggesting a superficial location (mainly abscesses of the submandibular region), as well as patients who were diagnosed with mononucleosis during hospitalization. The study analyzed the age and sex of the children, diagnostic methods, and bacterial culture tests of the abscess. Particular attention was drawn to the seasonality in the incidence of the parapharyngeal abscesses in children. A statistical analysis was performed and seasonality index for the data was calculated, and a simulation of the prognosis of the occurrence of the factor for a moving average with a reference period of 2 months was performed. Next, the thesis on the discrete uniform data distribution was adopted, and Monte Carlo method was used for testing of the hypothesis. The significance level was α = 1%. The probability of occurrence of 9 cases in one month was calculated based on the binomial distribution.
Results
Between January 2013 and February 2018, 23 patients with parapharyngeal and retropharyngeal abscesses were hospitalized in the Department of Pediatric Otolaryngology of the Medical University of Warsaw. The group included 13 boys and 10 girls. Mean age of the patients was 3 years and 5 months. The youngest patient was 5 months old, and the oldest was 9 years old.
All the patients had undergone upper respiratory tract infection before being diagnosed with parapharyngeal abscess. All the patients had enlarged neck lymph nodes. Other signs and symptoms are summarized in table 1.
Tab. 1. Signs and symptoms in patients with retro- and parapharyngeal abscesses
| Symptoms | Number of patients | Percentage of patients |
| Neck pain during palpation | 17 | 74% |
| Fever | 15 | 65% |
| Dysphagia | 20 | 87% |
| Dyspnea | 2 | 9% |
| Signs | Number of patients | Percentage of patients |
| Enlarged lymph nodes | 23 | 100% |
| Fluctuant lymph nodes | 9 | 39% |
| Trismus | 1 | 4% |
| Impaired neck mobility | 12 | 52% |
Due to the specificities of the Department, neck US was the preferred diagnostic method. US was supplemented with computed tomography in case of the absence of correlation between the general condition of the patient and the US results, or in the case of qualification for the surgical drainage of the abscess. US examination was also used to assess the efficacy of both the conservative treatment (in 11 patients – 48%) and surgical management (12 patients – 52%). In all the patients, toxoplasmosis, mononucleosis, cytomegaly, and Lyme disease were excluded.
Microbiological culture of the drained purulent content was performed in 12 patients. In 3 cases (25%), the growth of the Prevotella spp. was observed. In another 3 cases, the growth of the Streptococcus spp. (pyogenes, viridans, mitis, oralis) was observed, coexistent with Candida albicans in one patient. In 2 cases, staphylococci (MSSA and S. epidermidis) were grown. In the remaining 4 patients (33%), the culture was negative.
The highest percentage of patients was admitted to the Department in December (n = 39.1%). The second month in terms of the highest number of hospitalized children was March (n = 13.0%). The data is summarized in figure 4.
Fig. 4. Number of patients hospitalized in subsequent months of the year
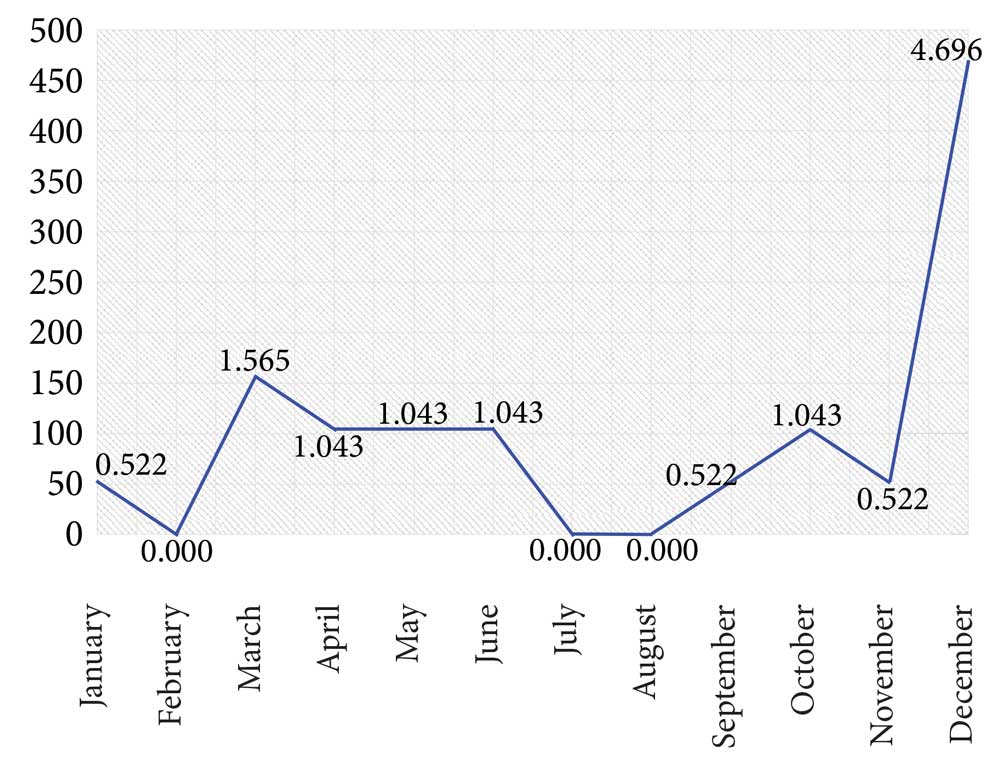
The seasonality index for December was over 3 times higher than for March and accounted 4.696 (fig. 5).
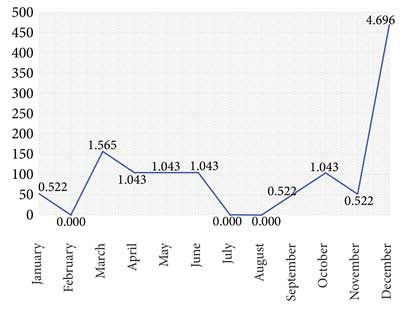
Fig. 5. Seasonality index
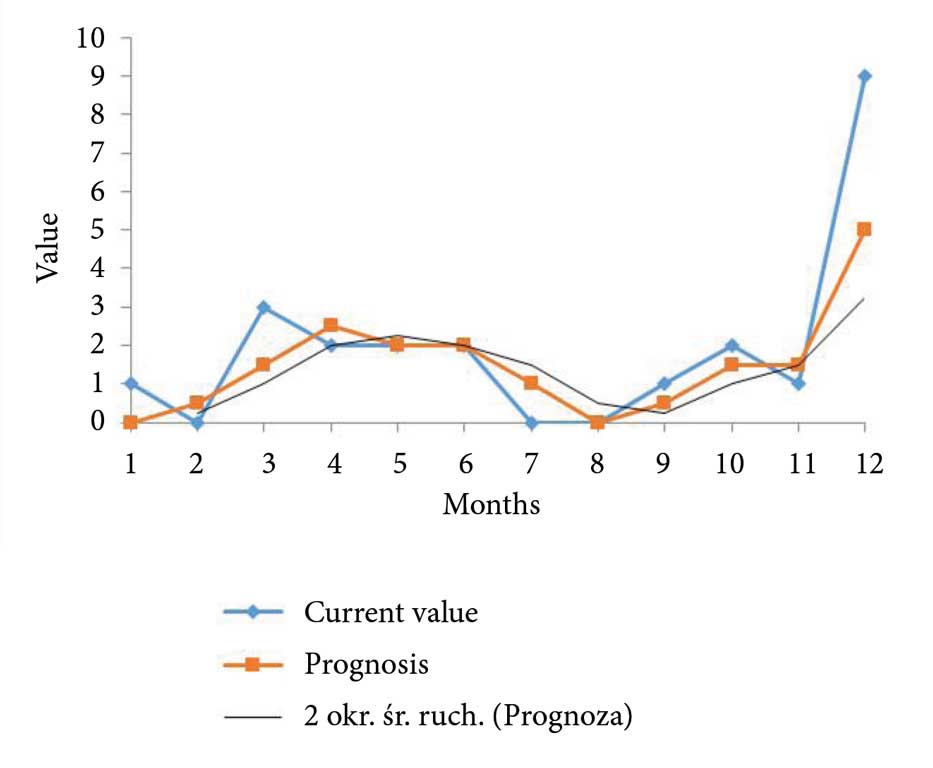
Due to the small number of patients, a simulation of the prognosis of the occurrence of the factor was performed. It was proven that the tendency for infections in December cannot be considered random (fig. 6).
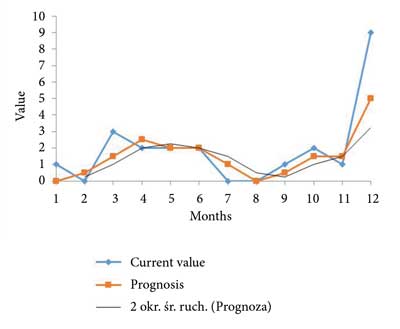
Fig. 6. Prognosis of the occurrence of the factor
In the next step, based on the research by Woods et al. (8), it was assumed that the incidence of retropharyngeal abscess in children was 3.5 (per 100,000 children/year), and of the parapharyngeal abscess – 1.4. Based on the information collected for this analysis, it was assumed that the coexistence of these two types of abscess occurs with a frequency not higher than 3 to 23 cases (fig. 7). Hence, it was established that the weighted index of the incidence of the parapharyngeal or retropharyngeal abscess in the pediatric population was 4.717 per year. In consequence, assuming a discreet monomial distribution, the probability of the occurrence of an abscess in every month was 3.93 x 10-6, which in turn means that the probability of the occurrence of 23 cases per year is possible for a population of 487,598.05. Hence, 100 Monte Carlo simulations were performed on a matrix of 487,600 x 12, where the expected value was 23. It was proven that the probability of hospitalization of 2 patients with retropharyngeal or parapharyngeal abscess in one month is P(2) = 0.25; the probability of hospitalization of 3 patients – P(3) = 0.19, 7 patients in the same month – P(7) = 0.0017, and 9 patients – P(9) = 0.000141 (tab. 2).

Fig. 7. Computed tomography imaging of a boy with a retro- and parapharyngeal abscess
Tab. 2. Binomial distribution
| p | 3.93E-06 |
| n | 487598 |
| k | |
| 0 | 0.147096 |
| 1 | 0.281935 |
| 2 | 0.270188 |
| 3 | 0.17262 |
| 4 | 0.082714 |
| 5 | 0.031707 |
| 6 | 0.010128 |
| 7 | 0.002773 |
| 8 | 0.000664 |
| 9 | 0.000141 |
| 10 | 2.71E-05 |
| 11 | 4.73E-06 |
| 12 | 7.55E-07 |
In the light of the above results, the thesis on the discrete monomial distribution of the data was considered untrue, which leads to the conclusion that December is a highly probable month for the occurrence of deep neck infection in children.
Discussion
Upper respiratory tract infection is the most common cause of deep neck abscess in children (5, 9). According to Coticchia et al. (10), such a relationship is established in 67% of children with deep neck space infections. Daya et al. (11) reports that 26 out of 54 patients with deep neck space infections (48%) had a history of an upper respiratory tract infection. In our analysis, all the children hospitalized in the Department for deep neck space infections had been previously diagnosed with an upper respiratory tract infection. Such a large discrepancy of results is a result of differences in the inclusion criteria. In this study, all patients with submandibular space infections were excluded, which resulted in the lack of the odontogenic cause for infection, which is, according to the literature, the second most common cause for deep neck space infections (12, 13).
Based on the collected data, it was concluded that the majority of the deep neck space infections affected patients under 6 years of age. This observation is supported by both domestic (5, 14, 15) and international reports (16-18). In our study, children under 6 years of age consisted 91.3% of the study group. In spite of the lack of unambiguous data on the gender differences in prevalence of the disease, most reports seem to indicate higher prevalence in boys (55.8–63%) (16, 18, 19). In the material of our Department, the boys to girls ratio was 1.3:1 (13 boys; 66.5%).
In all the patients, conservative treatment (initially empirical) consisted of clindamycin and a second- or third-generation cephalosporin depending on the general condition of the patient and whether or not the children had undergone previous antibiotic therapy. Intravenous treatment was modified after antibiotic susceptibility testing results from the bacterial culture of the drained purulent content. Similar approach was applied by McCley et al. (20), who proved that intravenous treatment with clindamycin or clindamycin in combination with cefuroxime resulted in a positive outcome in 10 out of 11 patients with radiologically confirmed retropharyngeal abscess. Similar conclusions are reported by Wong et al. (21), who stated that initial empirical antibiotic therapy in children in good clinical condition and small abscesses may provide an alternative for surgical drainage.
The seasonality in the incidence of the parapharyngeal abscesses in children is not discussed in the literature. Only few authors present the conclusions from their observations. Woods et al. (8) reported a significant increase in the number of hospitalizations due to a retro- or parapharyngeal abscess between December and May, with the highest incidence in February and March. Lander et al. (16) also reported an increase in the number of admissions of children with this diagnosis in March. Schweinfurth (17) indicated that it is typical for the patients with deep neck space infection to be diagnosed in spring. Both our simulations prove beyond doubt that it is December that is the most probable month for the hospitalization of a patient with a para- or retropharyngeal abscess. However, it should be noted that the month with the second highest number of hospitalizations is indeed March. Generally speaking, the seasonality of the occurrence of deep neck space infections is a problem that is difficult to be discussed in the international scientific community because of the differences in the nomenclature between the countries. It cannot be denied that the period of higher incidence of the upper respiratory tract infections results in a higher occurrence of deep neck abscess in children (5, 9).
Conclusions
1. In Poland, the admission of a child diagnosed with a retropharyngeal or parapharyngeal abscess is most likely in late autumn – in November and December.
2. Purulent deep neck space infections in children are a complication of upper respiratory tract infections.
3. Deep neck space infections are difficult to diagnose due to the lack of pathognomonic signs and symptoms.
4. The conservative treatment is an alternative to the surgical drainage in stable patients with small-size abscesses under the conditions of normalization of inflammatory marker levels and improvement of the general condition of the patient.
PiŇõmiennictwo
1. Aleksandrowicz R, Ciszek B: Anatomia Kliniczne GŇāowy i Szyi. PZWL. Warsaw 2007: 535-538.
2. Kanzaki S, Nameki H: Standardised method of selecting surgical approaches to benign parapharyngeal space tumours, based on pre-operative images. J Laryngol Otol 2008; 122: 628-634.
3. ŇĀasiŇĄski W: Anatomia GŇāowy dla stomatolog√≥w. 2nd ed., PZWL. Warsaw 1970: 364-367.
4. Rysz M, Ciszek B, StaroŇõciak S et al.: Anatomia i dostńôpy chirurgiczne do przestrzeni przygardŇāowej. Otolaryngol Pol 2011; 65(6): 428-435.
5. JabŇāoŇĄska-Jesionowska M, Zawadzka-GŇāos L: TrudnoŇõci diagnostyczne w rozpoznawaniu ropni gŇāńôbokich szyi: przestrzeni przygardŇāowej i zagardŇāowej u dzieci. Nowa Pediatr 2014; 04: 115-118.
6. Chmielik M: Otolaryngologia Dziecińôca. 1st ed., PZWL. Warsaw 2001: 120-122.
7. Phillipott CM, Selvadurai D, Banerjee AR: Pediatric retropharyngeal abscess. J Laryng Otol 2004; 118: 919-926.
8. Woods ChR, Cash ED, Smith AM et al.: Retropharyngeal and Parapharyngeal Abscesses Among Children and Adolescents in the United States: Epidemiology and Management Trends, 2003-2012. J Pediatric Infect Dis Soc 2016; 5(3): 259-268.
9. Brook I: Microbiology and management of peritonsillar, retropharyngeal, and parapharyngeal abscesses. J Oral Maxillofac Surg 2004; 62(12): 1545-1550.
10. Coticchia JM, Getnick GS, Yun RD, Arnold JE: Age-, site-, and time-specific differences in pediatric deep neck abscesses. Arch Otolaryngol Head Neck Surg 2004; 130(2): 201-207.
11. Daya H, Lo S, Papsin BC et al.: Retropharyngeal and parapharyngeal infections in children: the Toronto experience. Int J Pediatr Otorhinolaryngol 2005; 69(1): 81-86.
12. Garca MF, Budak A, Demir N et al.: Characteristics of Deep Neck Infection in Children According to Weight Percentile. Clin Exp Otorhinolaryngol 2014; 7(2): 133-137.
13. Vieira F, Allen SM, Stocks RM, Thompson JW: Deep neck infection. Otolaryngol Clin North Am 2008; 41(3): 459-483.
14. Dńôbska M, JabŇāoŇĄska-Jesionowska M, Chmielik M: Parapharyngeal abscesses in children – symptoms, diagnosis, treatment. New Medicine 2008; 3: 50-51.
15. Dńôbska M, BroŇľek-MńÖdry E, Gorzelnik A et al.: Management of the parapharyngeal space infection – symptoms, diagnostic and therapeutic issues. New Medicine 2011; 4: 122-124.
16. Lander L, Lu S, Shah RK: Pediatric retropharyngeal abscesses: a national perspective. Int J Pediatr Otorhinolaryngol 2008; 72(12): 1837-1843.
17. Schweinfurth JM: Demographics of pediatric head and neck infections in a tertiary care hospital. Laryngoscope 2006; 116(6): 887-889.
18. Grisaru-Soen G, Komisar O, Aizenstein O et al.: Retropharyngeal and parapharyngeal abscess in children – epidemiology, clinical features and treatment. Int J Pediatr Otorhinolaryngol 2010; 74(9): 1016-1020.
19. Huang Ch-M, Huang F-L, Chien Y-L, Chen P-Y: Deep neck infection in children. J Microbiol Imm Inf 2017; 50: 627-633.
20. McClay JE, Murray AD, Booth T: Intravenous antibiotic therapy for deep neck abscesses defined by computed tomography. Arch Otolaryngol Head Neck Surg 2003. 129(11): 1207-1212.
21. Wong DK, Brown C, Mills N et al.: To drain or not to drain – management of pediatric deep neck abscesses: a case-control study. Int J Pediatr Otorhinolaryngol 2012; 76(12): 1810-1813.