*Aneta Obcowska-Hamerska1, Jarosław Basaj2
Sexually transmitted diseases causing anorectal symptoms. Part 1. Bacterial infections
Choroby przenoszone drogą płciową powodujące objawy proktologiczne. Część 1. Choroby o etiologii bakteryjnej
1Department of General, Vascular and Oncological. Surgery, Medical University of Warsaw
2Endoscopic Laboratory, Czerniakowski Hospital Sp. z o.o.
Streszczenie
W artykule autorzy omawiają najczęstsze infekcje bakteryjne powodujące objawy proktologiczne przenoszone drogą płciową – STI. Mimo dużego rozpowszechnienia, świadomość występowania tej grupy chorób, trendów w zachowaniach seksualnych i epidemiologii STI jest wśród chirurgów zbyt mała. Autorzy omówili najczęściej występujące infekcje: rzeżączkę, chlamydiozę i kiłę. Wśród patogenów bakteryjnych przyczyną stanów zapalnych w odbytnicy i kanale odbytu mogą być także: Mycoplasma genitalium, Escherichia coli, Salmonella, Campylobacter, Shigella. W pracy z pacjentem podejrzanym o STI istotna, poza wiedzą teoretyczną, jest umiejętność prowadzenia w warunkach intymnych dla chorego rozmowy na temat jego współżycia i preferencji seksualnych, ryzyka infekcji HIV i zasadności przeprowadzania diagnostyki w tym kierunku. Choroby STI mogą mieć także etiologię wirusową, co będzie omówione w drugiej części artykułu.
Summary
The paper discusses the most common bacterial sexually transmitted infections (STIs) causing anorectal symptoms. Despite their high prevalence, the surgeons’ awareness of this group of disorders, trends in sexual behaviours and the epidemiology of sexually transmitted infections is still limited. We discussed the most common infections, i.e. gonorrhoea, chlamydia and syphilis, in this paper. Bacterial pathogens responsible for inflammation of the rectum and anal canal may also include Mycoplasma genitalium, Escherichia coli, Salmonella, Campylobacter, and Shigella. In the case of a patient with suspected sexually transmitted infection, in addition to theoretical knowledge, a conversation about the patient’s sexual history and preferences, the risk of HIV infection and the reasons for performing diagnosis for sexually transmitted infections under intimate conditions is also important. Sexually transmitted infections may also have a viral aetiology, which will be discussed in the second part of the paper.

Introduction
There has been a constant increase in the number of patients treated for sexually transmitted diseases. Over 500,000 cases of sexually transmitted infections (STIs) are reported annually in the EU countries alone (1, 2).
The local manifestation of the infection is not limited to the genitals. The presented symptoms depend on the site of pathogen entry, with possible involvement of the gastrointestinal mucosa, therefore such a diagnosis should also be considered in patients presenting with symptoms of anoproctitis. Despite their high prevalence, the surgeons’ awareness of this group of diseases, trends in sexual behaviours and the epidemiology of STIs is still insufficient. These elements are, however, of key importance for the identification of risk groups, proper diagnosis, treatment and limiting the further spread of infection. These measures are based on the knowledge of the human immunodeficiency virus (HIV), which characterises the high STI risk group and may affect the clinical picture presented by the patient both in the case of co-infection and superinfection.
STIs with anorectal manifestations usually result from receptive anal intercourse, which is practiced by men who have sex with men (MSM), as well as heterosexual persons and transgender women (3). Oral-anal intercourse and, in the case of gonorrhoea, transmission, e.g., via objects covered with infected vaginal discharge, are also possible routes of transmission (4-6).
The reported symptoms will differ, depending on the extent of bowel inflammation. Patients most often mention discomfort, anal pain, fresh blood during bowel movements, a feeling of painful tenesmus, or the presence of mucous and purulent discharge in the stool. These symptoms may vary in intensity or may not occur at all despite active infection (7, 8). This, along with the fact that some symptoms overlap with non-infectious anorectal conditions (such as inflammatory bowel disease, hemorrhoidal disease, anal fissure, anorectal cancers), may delay the diagnosis. It is also important for proper therapeutic management to be aware of frequent co-infections, which affect up to 40% of patients in the high-risk population (9).
In addition to appropriate diagnosis and in the absence of conservative treatment complications, the specific features of this group of pathologies also indicate the need for counselling on pathogen transmission and diagnostic investigations in sexual partners.
The following part of the paper will discuss the most common bacterial STIs, which are the reason for visiting a proctologist.
Gonorrhoea
Gonococcal proctitis, caused by Gram-negative bacilli known as Neisseria gonorrhoeae (N. gonorrhoea), is one of the most common STIs. Epidemiological data in Poland indicate a much higher ratio of infected men to women (14:1) than in other EU countries (10). The fact that at least half of men and up to 95% of women with proctitis are asymptomatic is the reason for a large pool of carriers and contributes to the increasing incidence rates (6).
Symptoms, if present, usually appear within 5-10 days of infection and include pruritus, sometimes rectal pain, a feeling of incomplete bowel movement, and mucopurulent discharge. Some patients report slight bleeding during bowel movements. Proctoscopy in the range of up to 10 cm may reveal indistinct vascular pattern, hyperaemia and contact bleeding of the mucous membrane, which is covered with mucopurulent secretion to a varying degree.
Diagnostic workup involves collecting samples for culture on a selective medium or for N. gonorrhoeae DNA detection assays, especially in the case of oligo- or asymptomatic gonorrhoea (11, 12). Infection limited to the anorectal region is observed in more than 70% of MSM cases compared to only a small percentage of women (6). Therefore, samples for testing should be taken from the urethra or urine, rectum and pharynx, i.e. sites involved in sexual practices (13).
In addition to reaching the diagnosis, microbiological testing allows for assessing the pathogen’s drug susceptibility, which is important in view of the increasing resistance of the diplococcus to other antibiotics (14). Samples are obtained by inserting a swab to a depth of about 3 cm into the anal canal, and then rubbing it against the epithelium around the circumference of the anorectal ring for about 10 seconds. Visual anoscopic inspection or taking a swab from the rectum are not required (15, 16). Once diplococcal infection is confirmed, the diagnosis should be extended with tests for other STIs (syphilis, chlamydia, HIV, hepatitis B, hepatitis C). To prevent further spread of the disease, testing should be recommended in persons who had sexual intercourse with the patient in the month preceding the diagnosis (this period is extended to 90 days in sexual partners of asymptomatic patients). In addition, patients are advised to abstain from sexual intercourse from the time of diagnosis until 14 days after treatment completion.
The most common therapeutic regimen consists of a single intramuscular injection of 1 g of ceftriaxone with 2 g of oral azithromycin.
Molecular testing to confirm eradication 2 weeks after antibiotic therapy is recommended in patients whose symptoms have resolved, and if positive, a microbiological test with antimicrobial susceptibility testing (AST) should be performed. In the case of persistent symptoms, culture and AST are performed 3-7 days after treatment completion (17).
Chlamydia
The intracellular bacterium Chlamydia trachomatis is the cause of two clinical entities, which differ, e.g. in severity. As with gonorrhoea, asymptomatic infections contributing to the spread of infection are observed. The route of transmission is also common for both pathogens.
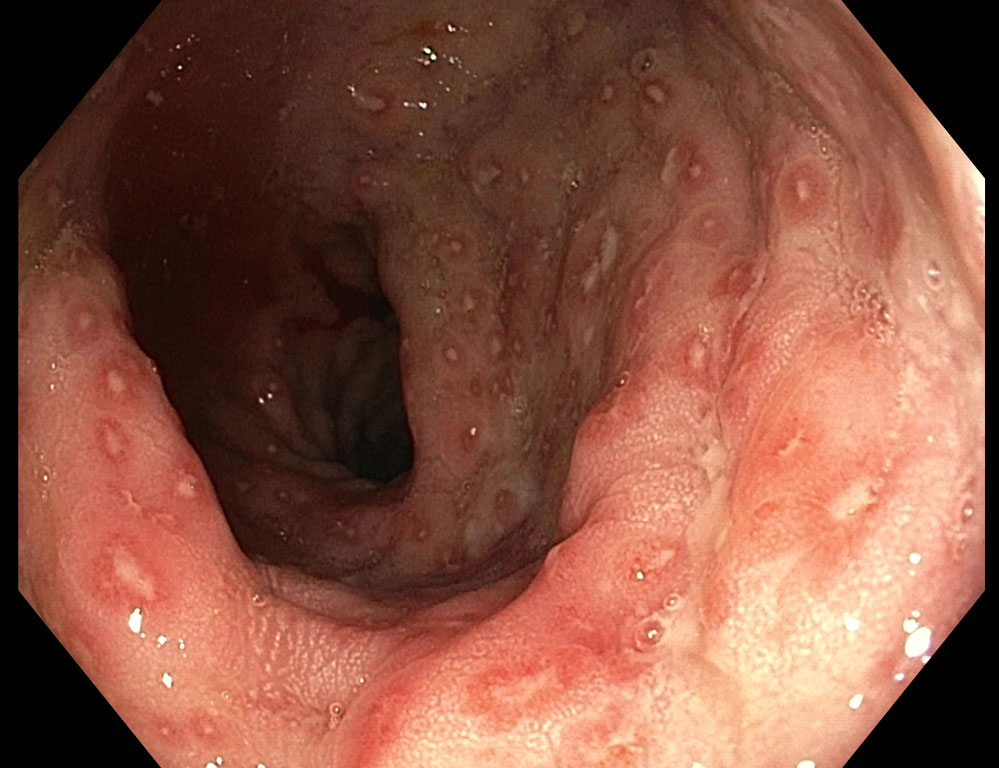
In addition to urethritis and cervicitis, serotypes A-K are the etiological factor of benign proctitis. This type of infection is the most prevalent and is usually asymptomatic. Rarely reported symptoms include anal pain, the feeling of straining during bowel movement and fever. The macroscopic picture of the mucosa can vary from normal to non-specific signs of inflammation, with hyperaemia and mucosal fragility (fig. 1).

Fig. 1. Inflammatory lesions in the rectum in the course of chlamydia infection
Among all anatomical sites of chlamydia in the MSM group, rectal infection is reported in almost 10%. A similar percentage is seen among women, with common coexistence with urogenital tract infection (18, 19).
A much more aggressive course has been reported for L1-L3 genotypes, which, by translocation from the mucosa to deeper tissues, penetrate into regional lymph nodes, causing lymphogranuloma venereum (LGV).
Compared to 20 years ago, when LGV cases were reported almost exclusively in tropical regions, it is now also observed in highly developed countries and mainly affects the MSM population, who are usually HIV-positive (20). It is likely that HIV itself is a factor promoting infection with L1-L3 genotypes, although this has not yet been fully confirmed (21).
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
24 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
59 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
119 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 28 zł
Piśmiennictwo
1. Miles AJ, Mellor CH, Gazzard B et al.: Surgical management of anorectal disease in HIV-positive homosexuals. Br J Surg 1990; 77: 869-871.
2. https://www.ecdc.europa.eu/en/publications-data/infographic-sexually-transmitted-infections-long-standing-and-ongoing-threat.
3. Tian LH, Peterman TA, Tao G et al.: Heterosexual anal sex activity in the year after an STD clinic visit. Sex Transm Dis 2008; 35: 905-909.
4. Wexner SD: Sexually transmitted diseases of the colon, rectum, and anus. The challenge of the nineties. Dis Colon Rectum 1990; 33: 1048-1062.
5. Halperin DT: Heterosexual anal intercourse: prevalence, cultural factors, and HIV infection and other health risks, Part I. AIDS Patient Care STDS 1999; 13: 717-730.
6. Beck D: Sexually transmitted diseases. The ASCRS Textbook of Colon and Rectal Surgery. 2nd ed. Springer, New York 2011: 295-307.
7. Kent CK, Chaw JK, Wong W et al.: Prevalence of rectal, urethral, and pharyngeal chlamydia and gonorrhea detected in 2 clinical settings among men who have sex with men: San Francisco, California, 2003. Clin Infect Dis 2005; 41: 67-74.
8. de Vries HJC, Nori AV, Kiellberg Larsen H et al.: 2021 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. J Eur Acad Dermatol Venereol 2021; 35: 1434-1443.
9. Gambotti L, Batisse D, Colin-de-Verdiere N et al.: Acute hepatitis C infection in HIV positive men who have sex with men in Paris, France, 2001-2004. Euro Surveill 2005; 10: 115-117.
10. European Centre for Disease Prevention and Control: Gonorrhoea. [In:] ECDC. Annual epidemiological report for 2017. ECDC, Stockholm 2019.
11. Whiley DM, Garland SM, Harnett G et al.: Exploring ‘best practice’ for nucleic acid detection of Neisseria gonorrhoeae. Sexual Health 2008; 5: 17-23.
12. Bachmann LH, Johnson RE, Cheng H et al.: Nucleic acid amplification tests for diagnosis of Neisseria gonorrhoeae and Chlamydia trachomatis rectal infections. J Clin Microbiol 2010; 48: 1827-1832.
13. Jin F, Prestage GP, Mao L et al.: Incidence and risk factors for urethral and anal gonorrhoea and chlamydia in a cohort of HIV-negative homosexual men: the health in men study. Sex Trans Infect 2007; 83: 113-119.
14. Whiley DM, Goire N, Lahra MM et al.: The ticking time bomb: escalating antibiotic resistance in Neisseria gonorrhoeae is a public health disaster in waiting. J Antimicrob Chemother 2012; 67: 2059-2061.
15. Deheragoda P: Diagnosis of rectal gonorrhoea by blind anorectal swabs compared with direct vision swabs taken via a proctoscope. Br J Vener Dis 1977; 53: 311-313.
16. Kolator B, Rodin P: Comparison of anal and rectal swabs in the diagnosis of anorectal gonorrhoea in women. Br J Vener Dis 1979; 55(3): 186-187.
17. Unemo M, Ross J, Serwin A et al.: 2020 European guideline for the diagnosis and treatment of gonorrhoea in adults. Int J STD AIDS 2020 Oct 29; 956462420949126.
18. van Liere GA, Hoebe CJ, Wolffs PF et al.: High co-occurrence of anorectal chlamydia with urogenital chlamydia in women visiting an STI clinic revealed by routine universal testing in an observational study: a recommendation towards a better anorectal chlamydia control in women. BMC Infect Dis 2014; 14: 274.
19. Pinsky L, Chiarilli DB, Klausner JD et al.: Rates of asymptomatic nonurethral gonorrhea and chlamydia in a population of university men who have sex with men. J Am Coll Health 2012; 60: 481-484.
20. de Barbeyrac B, Laurier-Nadaliè C, Touati A et al.: Observational study of anorectal Chlamydia trachomatis infections in France through the lymphogranuloma venereum surveillance network, 2010-2015. Int J STD AIDS 2018; 29(12): 1215-1224.
21. Tinmouth J, Gilmour MW, Kovacs C et al.: Is there a reservoir of sub-clinical lymphogranuloma venereum and non-LGV Chlamydia trachomatis infection in men who have sex with men? Int J STD & AIDS 2008; 19(12): 805-809.
22. de Vrieze NH, de Vries HJC: Lymphogranuloma venereum among men who have sex with men. An epidemiological and clinical review. Expert Rev Anti Infect Ther 2014; 12: 697-704.
23. de Vries HJC, Shiva Nagi Reddy B, Khandpur S: Lymphogranuloma Venereum. [In:] Gupta S, Kumar B (eds.): Sexually Transmitted Infections. 2nd edn. Elsevier, New Delhi 2012: 506-521.
24. Klint M, Löfdahl M, Ek C et al.: Lymphogranuloma venereum prevalence in Sweden among men who have sex with men and characterization n of Chlamydia trachomatis ompA genotypes. J Clin Microbiol 2006; 44(11): 4066-4071.
25. Lanjouw E, Ouburg S, de Vries HJ et al.: 2015 European guideline on the management of Chlamydia trachomatis infections. Int J STD AIDS 2016; 27: 333-348.
26. Soni S, Srirajaskanthan R, Lucas SB et al.: Lymphogranuloma venereum proctitis masquerading as inflammatory bowel disease in 12 homosexual men. Aliment Pharmacol Ther 2010; 32: 59-65.
27. de Vries HJC, de Barbeyrac B, de Vrieze NHN et al.: 2019 European guideline on the management of lymphogranuloma venereum. J Er Acad Dermatol Venereol 2019; 33(10): 1821-1828.
28. de Vries HJ, Zingoni A, White JA et al.: 2013 European Guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. Int J STD AIDS 2013; 25: 465-474.
29. Martin-Iguacel R, Llibre JM, Nielsen H et al.: Lymphogranuloma venereum proctocolitis: a silent endemic disease in men who have sex with men in industrialised countries. Eur J Clin Microbiol Infect Dis 2010; 29(8): 917-925.
30. Cha JM, Choi SI, Lee JI: Rectal syphilis mimicking rectal cancer. Yonsei Med J 2010; 51(2): 276-278.
31. Smith D: Infectious syphilis of the anal canal. Dis Colon Rectum 1963; 6: 7-10.
32. Mindel A, Tovey SJ, Timmins DJ, Williams P: Primary and secondary syphilis. Dis 1994; 18: 358-363.
33. Akdamar K, Martin RJ, Ichinose H: Syphilitic proctitis. Dig Dis Sci 1977; 22: 86.
34. Janier M, Unemo M, Dupin N et al.: 2020 European guideline on the management of syphilis. J Eur Acad Dermatol Venereol 2021; 35(3): 574-588.
35. Workowski KA, Berman S; Centers for Disease Control and Prevention (CDC): Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep 2010; 59(RR-12): 1-110.
36. Workowski KA, Bachmann LH, Chan PA et al.: Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep 2021; 23: 1-187.
37. Phipps W, Kent CK, Kohn R, Klausner JD: Risk factors for repeat syphilis in men who have sex with men, San Francisco. Sex Transm Dis 2009; 36: 331-335.
38. Fleming DT, Wasserheit JN: From epidemiological synergy to public health policy and practice: the contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect 1999; 75: 3-17.
39. Schwarcz SK, Kellogg TA, McFarland W et al.: Characterization of sexually transmitted disease clinic patients with recent human immunodeficiency virus infection. J Infect Dis 2002; 186: 1019-1022.
40. Kofoed K, Gerstoft J, Mathiesen LR, Benfield T: Syphilis and human immunodeficiency virus (HIV)-1 coinfection: influence on CD4 T-cell count, HIV-1 viral load, and treatment response. Sex Transm Dis 2006; 33: 143-148.