© Borgis - New Medicine 4/2007, s. 91-92
*Lechosław P. Chmielik, Magdalena Frąckiewicz, Mieczysław Chmielik
Operating changes in the media wall of the maxillary sinus children
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Prof. Mieczysław Chmielik, MD, PhD
Summary
Summary
Introduction. The development of diagnostic techniques has allowed us to detect changes which were not noticeable, or were included in a group of more important facts, in the past. . By the sides of the nose, in the classic radical operating method, as well as in cases of severe cancer or a juvenile angiofibroma through a side rhinotomy or Caldwell-Luc method;Roug´a-Denkera method; Moure,a method. Methods of functional endoscopic surgery have been described by Vigand and Stammberger.
Methods. These methods are baased on the use of endoscopes sizes 0, 30, 70 and 120, and the correct set of forceps. In operations on infant sinuses, an especially useful device is a rinsing/suction set, and a microdebrader with a set of angled ends, allowing access to the choden region of the sinuses. The classic route to the maxillary sinus in the FESS operation is to control the sinuses optically. We use a trocar, which is led into the maxillary under inferior turbinated bone. To introduce any additional instruments, it is necessary to make, under the inferior turbinated bone, a flap, using Rettinger´s Method. It is possible to introduce optics and instruments to the maxillary sinuses through a opening ethmoidal infundibulum. When the methods presented above are insufficient, we make a perforation by trocar in the canine fossa, and lead the optics to the maxillary sinuses.
Conclusions. Operations on small patients are greatly eased by the use of the correct instrumentation, but these do not solve all the problemsThe Rettinger´s flap or a opening ethmoidal infundibulum is usually enough to access the median wall of the maxillary sinus.
Acessing the affected area(s) on the median wall of the maxillary sinus is technically difficult
INTRODUCTION
The development of diagnostic techniques has allowed us to detect changes which were not noticeable, or were included in a group of more important facts, in the past. Thanks to CT, we have the possibility of precise locating of changes in the sinuses.
By the sides of the nose, in the classic radical operating method, as well as in cases of severe cancer or a juvenile angiofibroma through a side rhinotomy or Caldwell-Luc method; Roug´a-Denkera method; Moure,a method. Thanks to the development of operative techniques, we have the possibility of removing only specifield changes in the nasal sinuses area. Methods of functional endoscopic surgery have been described by
I Wigand:
– 1 removal of a posterior part of middle nasal concha
– 2 sinusotomy of sphenoid sinus; sinusotomy of anterior and posterior ethmoid sinus
– 3 removal of uncinate process and control of maxillary sinus
II Stammberger:
– 1 removal of uncinate process and control of maxillary sinus
– 2 opening of ethmoidal bulla, sinusotomy of anterior and posterior ethmoid sinus
– 3 sinusotomy of sphenoid sinus
These methods are baased on the use of endoscopes sizes 0, 30, 70 and 120, and the correct set of forceps. In operations on infant sinuses, an especially useful device is a rinsing/suction set, and a microdebrader with a set of angled ends, allowing access to the choden region of the sinuses.
Operations on small patients are greatly eased by the use of the correct instrumentation, but these do not solve all the problems. One of the most difficult locating tasks during the FESS procedure concerns the affected sites on the median wall of the maxillary sinus. In these cases, the surgeon is forced to do the operation on the area "to be on surgeon´s abdomen”. It is because of this the authors have decided to share their experience of FESS operations on children, gained in the children´s otolaryngological clinic in Warsaw.
The classic route to the maxillary sinus in the FESS operation is to control the sinuses optically. We use a trocar, which is led into the maxillary under inferior turbinated bone. To introduce any additional instruments, it is necessary to make, under the inferior turbinated bone, a flap, using Rettinger´s Method. It is possible to introduce optics and instruments to the maxillary sinuses through a opening ethmoidal infundibulum. When the methods presented above are insufficient, we make a perforation by trocar in the canine fossa, and lead the optics to the maxillary sinuses.
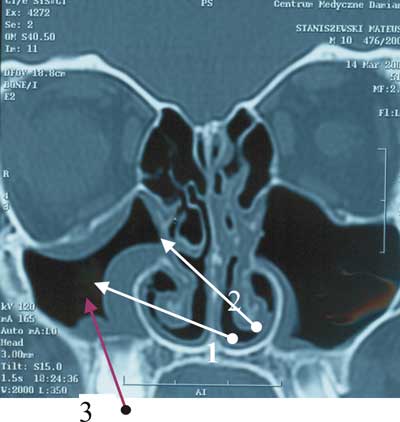
Pic. 1. FESS approche to the maxillary sinus

Pic. 2. Rettinger´s flap
CONCLUSIONS
1. The Rettinger´s flap or a opening ethmoidal infundibulum is usually enough to access the median wall of the maxillary sinus.
2. Acessing the affected area(s) on the median wall of the maxillary sinus is technically difficult.
Piśmiennictwo
1. Chmielik M, et al.: Operacje endoskopowi zatok (mini FESS) u dzieci. Otorynolaryngologia; supl. 1, 2004; 38-41.2. Rettinger G, Gjuric M: Osteoplastic endonasal approach to the maxillary sinus. Rhinology 1994; 32 (1): 42-44.3. Stammberger H, Pasawetz W: Functional endoscopic sinus surgery. Concept, indications and results of the Messerklinger technique. Eur. Arch. Otorhonolaryngol., 1990; 247 (2).4. Wigand ME: transnasale, Endoskopischer Chirurgie der Nasennebenhohlen bie chronischer sinusitis. II Die Endonasale Kieferhohlen-Operation. HNO 1981; 29: 263-269.