© Borgis - New Medicine 3/2003, s. 69-72
Marek Zak1, Tomasz Grodzicki2
Falls of female patients suffering from cardiovascular diseases – assessment of potential risk factors and individual ability to cope after an accidental fall
1 Faculty of Clinical Rehabilitation, Academy of Physical Education, Cracow, Poland
Head: prof. Krzysztof Spodaryk, MD, PhD
2 Faculty of Internal Medicine and Gerontology,
Jagiellonian University School of Medicine, Cracow, Poland
Head: prof. Tomasz Grodzicki, MD, PhD
Summary
Background: Accidental falls are feared by an increasing number of elderly persons as a symptom of ageing, giving them a fear of becoming care-dependent as a result of a serious fall.
Materials and methods: The study group comprised 40 female patients (aged 65-94) in the Geriatric Ward, of the Municipal Medical & Nursing Facility, Krakow, under treatment for cardiovascular diseases. Each of them was reported to have sustained at least one fall prior to hospitalisation.
The study focused upon assessing the risk of falls and individual functional abilities, in accordance with Pilet and Swine´s method. A 3-week long rehabilitation programme included an individually structured exercise programme, designed to assist in reducing the risk of falls, and offering practical guidance on how to cope after a fall.
Results: In the test assessing risk of falls, 15-35% of patients were reported to experience improvement; statistical significance ranged from 0.007 to 0.04.
In the test assessing ability to cope after a fall, 15-23% of patients experienced improvement; statistical significance ranged from 0.008 to 0.04.
Conclusions: A specifically structured programme of physical rehabilitation was effective in preventing accidental falls in elderly females with hypertension, as well as increasing individual ability to cope effectively after an accidental fall.
BACKGROUND
Accidental falls are seen by an increasing number of elderly persons as a definite symptom of ageing, giving them a fear of becoming care-dependent after any serious fall. Admittedly, the risk of sustaining a fall increases with age. For every 100 fall events every year, 47 are sustained by people aged 70-74 years. This percentage seems to rise rather sharply amongst octogenarians (1, 2). The majority of falls are sustained during such simple activities as getting out of bed, change of posture (e.g. bending down to pick something up), or just walking along (2, 3, 4, 5). Only ca. 5% of falls are reported to occur when potentially dangerous tasks are being attempted, e.g. climbing a ladder, standing on a chair, etc. (6, 7). Falls that do not result in a serious trauma nevertheless often lead to the development of post-fall syndrome in the victim, and consequently to a much reduced physical capability and overall anxiety.
Minimising the risk of accidental falls and resulting complications depends upon gaining an insight into the accompanying circumstances, to establish the nature of potential risks and develop effective measures aimed at their prevention. Detailed reconstruction of the circumstances is a practical way of establishing all key risk factors, facilitates subsequent monitoring of patients´ mobility, and effectively prevents them from taking risks (8, 9, 10, 11, 12).
Numerous reports on the subject, and clinical observations give, ample grounds for believing that rehabilitation is an essential component in any fall prevention programme for the elderly, and when offered with targeted medical therapy, may reduce the risk of fall by over 30% (13).
However, reports focused on assessing the significance of physical rehabilitation in fall prevention programmes remain scarce. In view of this, the authors wished to make such an assessment and address the following research issues:
? Is a specifically designed physical rehabilitation programme capable of reducing the risk of falls in female patients suffering from hypertension, and if so, by how much?
? Can such a specifically designed physical rehabilitation programme assist such patients in coping effectively after an accidental fall?
MATERIALS AND METHODS
The study group comprised 40 female patients (aged 65-94) from the Geriatric Ward of the Municipal Medical & Nursing Facility, Krakow, under treatment for hypertension. Each of them was reported to have sustained at least one fall prior to admission.
The following criteria were applied in placing patients in the study:
1. Patient´s informed written consent for participation.
2. At least one fall sustained within a 3-month period immediately preceding admission.
3. Diagnosed hypertension.
4. Overall fitness allowing participation.
5. Mental condition allowing consent to participation in the study and the attendant physical rehabilitation programme.
6. Consent of the patient´s physician to participation in the study in view of the on-going hypertension therapy.
The criteria required that each patient (under treatment for hypertension) should have sustained at least one accidental fall in the period preceding the study (July – December 2000). Out of 220 patients 40 (aged 65-94) were eventually enrolled into the study. The study focused upon assessing the risk of accidental falls and individual functional abilities, in full compliance with the method of Pilet and Swine (14). A 3-week-long (average) rehabilitation programme embraced, e.g. individual counselling on the potential risk of falls, kinesitherapy, practical exercises on safe change of posture, and guidance on how to cope effectively after sustaining an accidental fall.
The study consisted of two parts. The first focused on assessing the risk of fall during routine daily activities, and the second addressed individual ability to cope effectively after sustaining a fall.
Both assessments were repeated for each patient after the physical rehabilitation programme.
PHYSICAL REHABILITATION PROGRAMME
? Individually tailored kinesitherapy – pursued for 3 weeks, 3 times a week at 30-min. sessions (average length of hospitalisation), was designed to:
– improve or at least maintain, the functioning of a patient´s circulatory, respiratory and nervous systems,
– improve and/or maintain a patient´s posture and sense of balance,
– improve and/or maintain a patient´s muscle strength and range of joint movement.
? The therapy also aimed to:
– teach a patient how to change posture safely (from a sitting position to a fully upright position and vice versa),
– teach a patient how to get up effectively after sustaining a fall,
– determine the appropriate type of walking aids to be used if needed,
– provide practical advice on how to avoid undue exposure to a risk of potential fall.
The patients´ blood pressure and pulse were routinely monitored during the therapeutic sessions, as well as prior to their commencement.
RESULTS
Since all parameters under investigation were assessed with the aid of the 0-2 scale, a non-parametric Wilcoxon test was used to compare the paired variables, to determine the statistical significance of any differences. All data were subsequently processed by the Statgraphic for Windows v. 3.1. software package.
In the test assessing individual risk of falls, 30-35% of patients were reported to experience improvement (Graphs 1-2). Statistical significance ranged from 0.007 to 0.008.
In the test assessing individual ability to cope after sustaining a fall, 15-23% of patients experienced improvement (Graphs 3-5). Statistical significance ranged from 0.008 to 0.04.
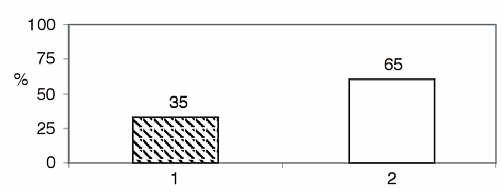
Graph 1. Results of the test on walking a 5-metre distance across two threshold-imitating obstacles.
in 14 subjects (35 %) improvement was observed
in 26 subjects (65%) no improvement was observed
Sign test:
Number of values below the hypothesized median = 14
Number of values above the hypothesized median = 0
Anticipated number of values = 7
Large sample test statistics (continuity correction applied) = 2.75
P-Value = 0.008
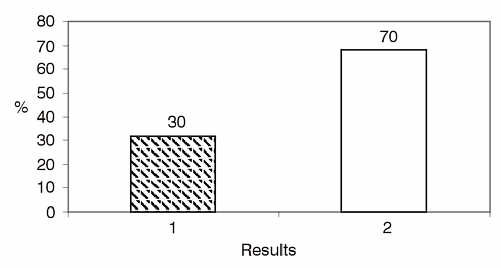
Graph 2. Results of the test on lifting an object off the floor.
in 9 subjects (30%) improvement was observed
in 19 subjects (70%) no improvement was observed
Sign test:
Number of values below the hypothesized median = 12
Number of values above the hypothesized median = 0
Anticipated number of values = 6
Large sample test statistics (continuity correction applied) = 3.17
P-Value = 0.007
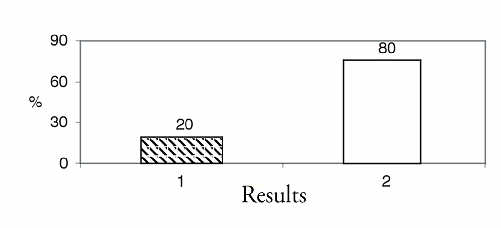
Graph 3. Results of the test on regaining an upright position from a laying down position.
in 8 subjects (20%) improvement was observed
in 32 subjects (80%) no improvement was observed
Sign test:
Number of values below the hypothesized median = 8
Number of values above the hypothesized median = 0
Anticipated number of values = 4
Large sample test statistics (continuity correction applied) = 2.32
P-Value = 0.04
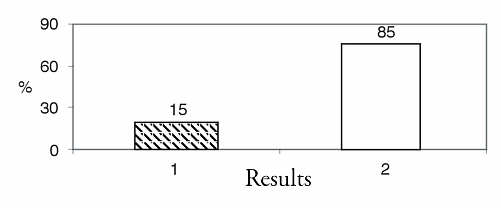
Graph 4. Results of the test on regaining an upright position from a kneeling position, supported with both hands.
in 6 subjects (15%) improvement was observed
in 34 subjects (85%) no improvement was observed
Sign test:
Number of values below the hypothesized median = 6
Number of values above the hypothesized median = 0
Anticipated number of values = 3
Large sample test statistics (continuity correction applied) = 2.34
P-Value = 0.008

Graph 5. Results of the on test regaining an upright position from kneeling on one knee only.
in 9 subjects (23%) improvement was observed
in 31 subjects (77%) no improvement was observed
Sign test:
Number of values below the hypothesized median = 9
Number of values above the hypothesized median = 0
Anticipated number of values = 4,5
Large sample test statistics (continuity correction applied) = 2,84
P-Value = 0,04
Comparative analysis was done by a non-parametric Wilcoxon test. Results confirmed the statistical significance of all parameters under investigation, which in turn gave ample grounds for believing that an appropriately designed and structured physical rehabilitation programme might be instrumental in further fall prevention.
DISCUSSION
The therapeutic efficiency of the structured physical rehabilitation programme applied in the study was confirmed by the significantly reduced number of falls sustained after its conclusion, compared to the number of falls experienced in the period prior to its commencement. Similar findings are reported by Campbell et al. (15, 16) who, having assessed a group of 233 women (mean age 80 years), concluded that individually structured rehabilitation exercise programmes were indeed instrumental in bringing down significantly the number of falls and the resultant complications.
The findings of Campbell et al. matched the reports of Wolf et al. (17), who assessed the influence of Tai Chi exercises upon the incidence of falls amongst a group of 200 nursing home residents aged over 70. The results obtained by Zak et al. (18), who pursued an individually structured physical rehabilitation programme in a group of 28 nursing home residents were very similar. Both investigators established that consistent pursuit of such a programme accounted for a drop of over 40% in the incidence of falls. Hauer et al. (7), in a randomised trial on 57 subjects (aged 75-90 years), concluded that the incidence of falls was reduced by ca. 25% through diverse and individually structured exercise programmes. Tinetti et al. (13), pursuing a multi-factorial intervention, which consisted of reducing the risk factors and implementing a specifically structured exercise programme, reported a reduction of over 30% in the incidence of falls.
The results also proved encouraging in enhancing individual ability to cope effectively after sustaining a fall. Apart from efforts aimed at reducing the risk of falls, it is of at least equal importance to prepare an elderly person for a situation when he becomes the victim of an accidental fall. He should be reasonably capable of copying on his own (unless it was an injurious fall), by relying on specific practical advice provided by the supervising physiotherapist. Individual anxiety related to a risk of fall is not always focused on the adverse consequences of a potential accident, but far more often it results from a deep seated fear that it may prove too hard to cope unassisted afterwards. As reported by Reece and Simpson (19), many of the elderly find themselves quite incapable of picking themselves up successfully after a fall, despite not having sustained any injuries whatever during such an adverse event.
CONCLUSIONS
1. A specifically structured programme of physical rehabilitation proved effective in preventing accidental falls in elderly female patients diagnosed with hypertension.
2. The programme also proved instrumental in increasing individual capability to cope effectively after an accidental fall.
Piśmiennictwo
1. Simpson J.M.: Eldery people at risk of falling: the role of muscle weakness. Physiother. 1993; 79:12-18. 2. Studenski S. et al.: Predicting falls: the role of mobility and nonphysical factors. J. Am. Geriatr. Soc. 1994; 42:297-302. 3. Lord S.R. et al.: Physiological factors associated with injurious falls in older people living in the community. Gerontology 1992; 38:338-46. 4. Rigler S.K.: Preventing falls in older adults. Hospit. Pract. 1999; 34:8-12. 5. Żak M.: Ocena ryzyka upadków u osób starszych i możliwości prewencji. Gerontol. Pol. 2000; 8:18-21. 6. Galus K., Kocemba J. (Red.): MSD Podręcznik Geriatrii. Wydawnictwo Urban & Partner, Wrocław 1999; p. 70-84. 7. Hauer K. et al.: Exercise training for rehabilitation and secondary prevention of falls in geriatric patients with a history of injurious falls. J. Am. Geriatr. Soc. 2001; 49:10-20. 8. Buchner D.M. et al.: The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J. Gerontol. A. Biol. Sci. Med. Sci.1997; 52:218-24. 9. Thornby M.A.: Balance and falls in the frail older person: a review of the literature. Top. Ger. Rehbil. 1995; 11:35-43. 10. Żak M.: Rehabilitacja w procesie leczenia osób starszych. Gerontol. Pol. 2000; 8:18-21. 11. Tinetti M.E.: Performance – oriented assessment of mobility problems in elderly Patients. J. Am. Geriatr. Soc. 1986; 34:119-26. 12. Leipzig R.M. et al.: Drugs and falls in older people: A systematic review and meta-analysis: II. Cardiac and analgesic drugs. 1999; 47: 40-50. 13. Tinetti M.E. et al.: A multifactorial intervention to reduce the risk of falling among elderly people living in the community. N. Engl. J. Med. 1994; 331:821-7. 14. Pilet J.M., Swine Ch.: Kinesitherapie geriatrique et prevention des risques de chute. Temp. Med.1998; 6:11-16. 15. Campbell A.J. et al.: Fall prevention over two years: a randomised controlled trial in women 80 years and older. Age Ageing 1999; 28: 513-18. 16. Campbell A.J. et al.: Randomized controlled trial of a general practice programme of home-based exercise to prevent falls in elderly women. Br. Med. J. 1997; 315:1065-9. 17. Wolf S.L. et al.: Reducing frailty and falls in older persons; an investigation of Tai Chi and computerized balance training. J. Am. Geriatr. Soc. 1996; 44: 489-97. 18. Żak M., Melcher U.: Rehabilitacja jako element programu zapobiegania upadkom osób starszych. Przegl. Lek. 2002; 59: 308-13. 19. Reece A.C., Simpson J.M.: Preparing older people to cope after a fall. Physiother. 1996; 82:227-35.