© Borgis - New Medicine 1/2009, s. 2-6
*Erika Erdősi1, László Papp2, Kornélia Helemba3
The Personality Background of BSc Student Nurses´ Assertiveness in Hungary
1Department of Nursing, Faculty of Health Sciences and Social Studies, University of Szeged, Hungary
2Department of Nursing, Faculty of Health Sciences and Social Studies, University of Szeged, Hungary
3Head of Department
Department of Nursing, Faculty of Health Sciences and Social Studies, University of Szeged, Hungary
Summary
Aim.To assess the profession-specific qualities of assertiveness, and to explore the interaction of the personal traits that significantly define assertiveness during the period of professional training.
Material and method. Quantitative research among BSc student nurses at the Faculty of Health Sciences and Social Studies, University of Szeged between 2004 and 2008. In order to achieve the aims of the research, the following battery of methods was compiled: Rathus Assertiveness Schedule, Empathy Questionnaire, Brengelmann Anxiety Scale, Social Intelligence Test. Descriptive and mathematical statistical methods were employed in the data analyses.
Results. One of the basic dimensions of assertiveness is marked by the simultaneous functioning and successful complementing of the empathy-based „other-centred” attitude and the enforcement of self interest. The other decisive feature, from the aspect of the functioning of the social relation system, has been found to be the quality of reaction types, that is the psychovegetative and emotional harmony.
Conclusions. During training, we have to focus on developing personal traits that highly define assertiveness.
Introduction
Nursing is centred on the nurse-patient/client relationship. Nursing is a profession whose „object” is the human being and thus the success of the work is partly determined by the effective cooperation with patients/clients and other health care professionals.
Assertive behaviour means accepting ourselves and others as well; it is a behaviour that is built on forcefulness, true self-evaluation while the person openly expresses their feelings, thoughts, enforces their rights and reaches their goals at the same time as they consider other people´s feelings, rights and interests [4].
Numerous articles on assertion appearing in nursing journals have conveyed the importance of the personality background of nurses´ assertiveness [2, 3, 11, 17, 18]. In addition, several researchers who studied student nurses found them to be low in assertion and high in submission [1, 6, 8, 13, 15, 19].
Our research that takes place in the setting of a nurse training college is based on an approach of assertiveness that mainly concentrates on which interpersonal traits support assertiveness.
Material and methods
We used the Rathus Assertiveness Schedule (RAS) to evaluate assertiveness [16]. The test measures the following factors: Insecurity, Self-esteem disorder, Self-assertion when being a customer, Saying no, Personal involvement in a relationship, Expressing feelings.
To establish the level of empathy, we used an empathy questionnaire compiled by Deutsch-Madle [7].
In the survey we applied the Brengelmann Anxiety Scale, which covers neuroticism, rigidity and extraversion-introversion [5].
The "Story ending” factor of the "4 Factor Social Intelligence Test” (SIT I.) compiled by O´Sullivan and Guilford measures the recognition of behaviour implications, that is the ability with which we can foresee the consequences of the participants´ attitude in a situation [14].
Statistical analysis covered the frequency distribution, the mean value and the dispersion in the case of each measuring tool.
Correlations were calculated to explore the connections between the factors of the RAS and to establish all the relationships among the factors of each tool used in the survey.
When analysing the empathy questionnaire, we performed a principal components analysis to map out how individual statements can form latent structures, namely what the possible subcomponents of empathy are.
The research was carried out with third year regular (N=48) and correspondent (N=266) nurse students at the Faculty of Health Sciences and Social Studies, University of Szeged. Four consecutive year groups were involved in the survey beginning in the year 2004/2005 and the total number of students was 350. During the years 2004/2005 and 2005/2006 we performed preliminary tests with the aim of exploring the main traits that are important in dealing with the patients effectively and to define the main directions of the research, with analysis of the indicators of the Empathy Questionnaire, the Social Intelligence Test and the Brengelmann Anxiety Scale. On the basis of the results we arrived at in the first two year groups, we included the RAS in our research for the 2006/2007 and 2007/2008 year groups in order to broaden the production surface and to determine the areas that need to be developed in an even more complex way.
Results
First we determined the level of assertiveness among the nurse students and the features of the individual factors of assertiveness.
The score range of the test is between -90 and +90: the higher the score the more assertive the person is. Comparing the results with other tests that examined samples with similar features, we can establish that the mean score (M=7.95) of our sample was below that of the others and the dispersion (SD=14.3) was lower [9, 10, 13]. So the sample is consistently low in reference to the assessed factor and it can be described as a near average assertiveness level.
In order to describe the five factors statistically, we chose the basic statistical indicators, which are summarised in the table (1) below.
Table 1. The scores of assertiveness factors (N=185).
| Factors | Mean | Dispersion | Minimum | Maximum |
| Insecurity, disorder in self-esteem | 3.52 | 7.08 | -12 | 19 |
| Expressing feelings | 0.41 | 3.5 | -7 | 9 |
| Self-enforcement in consumer situations | -0.79 | 3.02 | -6 | 6 |
| Saying no | 1.03 | 2.82 | -6 | 8 |
| Personal involvement in relationships | 3.63 | 3.38 | -8 | 9 |
The students reached the highest scores in the factor of Personal involvement in relationships. Thus we can make a conclusion that in this sample the inclination to participate in partnership is high, which corresponds to the nature of their profession. The lowest mean score was attained in the factor of Self-enforcement in consumer situations, which shows that students handle situations with uncertainty where individual interests are offended.
In the second phase we assessed the factors which are closely connected to assertiveness and have a great significance in patient management, with special attention to the features of controlling internal tensions.
We analysed three factors from the battery of tests: Neuroticism, Rigidity, and Extraversion-Introversion.
The scores are as follows: Neuroticism M=19.79, SD=8.3; Rigidity M=18.59, SD=5.38; Extraversion-Introversion M=17.95; SD=7.42. Comparing the mean scores with the standardised means of the anxiety scale, we can draw the conclusion that the sample reached a score that is close to the standardised means in Neuroticism and Extraversion-Introversion. However, the mean score of Rigidity is significantly, 4 points higher than the average adult score, and this means that rigidity is a characteristic trait among the students (Figure 1).
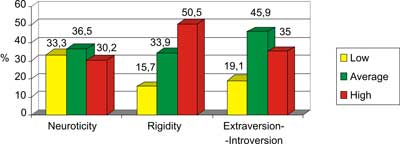
Fig. 1. Tension control (N = 350).
Concentrating on the connections among the factors, it can be established that a significant negative correlation exists between the factors of Neuroticism and Extraversion-Introversion (r=-0.381, p<0.001). A high score in one indicator entailed a low score in the other factor, namely a high score in Neuroticism led to introversion and a low score resulted in extraversion. Therefore we can state that both a highly introvert and a highly extravert personality incline to emotional instability because in the case of the Neuroticism factor a balanced emotional reaction is most possible in the mean area of neuroticism.
In the third phase we explored the functioning of assertiveness in connection with empathy and social intelligence, which serves as a basis for empathy.
The empathy questionnaire determines the value of empathy with 25 items so the maximum score is 25. Figure 2 shows the total scores of the sample.
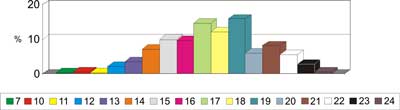
Fig. 2. The Scores of the Empathy Questionnaire (N = 350).
The scores were between 7 and 24 on the scale. The typical indicators are favourable for assertiveness: the mean values were high (M=17.59) and the dispersion was low (SD=2.83) so the sample is consistently high in reference to the assessed factor, and it can be described as a near average empathy level.
As a result of the principal component analysis, ten factors emerged as subcomponents. These factors were also examined focusing on high and low empathy level (Table 2).
Table 2. The distribution of empathy by the factors (N=350).
| Factor 1 | Passive reception of emotions | 90.77% |
| Factor 2 | The influence of people around | 52.87% |
| Factor 3 | The influence of strong (negative) impulses | 46.70% |
| Factor 4 | Annoying factors | 17.15% |
| Factor 5 | Social sensitivity | 76.95% |
| Factor 6 | Emotional independence | 75.35% |
| Factor 7 | Emotional suggestibility | 72.46% |
| Factor 8 | Readiness to meet people | 85.10% |
| Factor 9 | Perception of other people´s emotions | 93.90% |
| Factor 10 | Emotions against others | 79.40% |
The sample reached the highest percentage in the Perception of other people´s emotions and the Passive reception of emotions was also outstanding among the factors. The latter refers mainly to situations where the individual – while contemplating passively – takes over and experiences a mood brought about by external factors.
The two lowest scores appear in factor 3 and 4. Both of them measure empathy in situations which try one´s empathy to a great extent (aggression, self-centeredness).
Behaviour recognition is an aspect of social intelligence that forms the basis of empathy and by social sensitivity it helps the individual to foresee a person´s or people´s answer to other people´s emotions, thoughts and intents.
The total score of SIT I. was between 9 and 28 with the maximal attainable score being 29 (M=18.15; SD=3.82). The average score is more than 3 points less than the average given in the handbook of the test (M=21.37) while the dispersion value is nearly the same (SD= 3.85). Thus we can state that our students reached a weaker score than their peers uniformly.
The data were compared with the standard categorical distribution compiled by Guilford and O´Sullivan [14]. We can see that over two thirds of our students (15.8% + 55.8%) have more difficulties than the average to assess behavioural implications (Table 3).
Table 3. The distribution of SIT I. Scores by Categories (N=350).
| Category | Category boundaries | % Standard % score (%) |
| 1. | 0-14 | 15.80 > 4.80 |
| 2. | 15-20 | 55.80 > 24.00 |
| 3. | 21-23 | 21.50 < 35.80 |
| 4. | 24-26 | 5.30 < 25.37 |
| 5. | 27-29 | 1.60 < 7.00 |
Since empathy has a major role in social intelligence, we examined the connection between the two tools and we found a negative correlation (r=-0.18, p<0.05). We believe that the more accurately one can read one´s partner´s non-verbal signs, that is the higher the score one obtains in the social intelligence test, the more likely one is to meet negative impulses that one cannot interpret adequately (e.g. annoying factors, aggressive signs) and it can cause the level of empathy to drop.
In the fourth stage, we examined the connections among the factors considered important in the background of assertiveness.
Empathy questionnaire and tension control: only the high category of the neuroticism factor correlated with the total score of empathy (r=0.217, p<0.01); in other words, concentrating on the other person´s feelings resulted in an unbalanced, unstable state in our students.
SIT I. and tension control: based on the correlation of the mean area of neuroticism and the total score of SIT I. (r=0.174; p<0.01) we can state that in our sample the interpretation and predictions of the role partner´s behaviour were supported by emotional stability.
In the fifth stage, we aimed at examining the influencing effect of assertiveness factors and establishing connections among the influencing factors.
The assertiveness factors were also compared with the scores gained in the Empathy questionnaire. We found a connection in only one factor, namely Saying no (r=-0.154; p<0.05). The connection shows that the more empathic a person is, the less they can say no, so in this sense a conscious attention to the other person makes it harder to refuse a role partner´s request in situations that hurt one´s interests.
Examining the correlation between the scores obtained in assertiveness factors and the SIT I., we can find a connection between the value of Self-enforcement in consumer situations and that of social intelligence (r=-0.244; p<0.01). The negative significant correlation shows that enforcing one´s own interest hinders the interpretation of the other person´s feelings and the prediction of their possible behaviour.
The indicators of the RAS and tension control: each factor of assertiveness indicated a close connection with the factor of extraversion-introversion, which means the behaviour of people defined by social reality is more assertive in the sense of significant positive correlations. The Insecurity and the self-assessment disturbance factor proved to be significant for both neuroticism and rigidity. In the case of both factors emotional instability and rigid behaviour increased the degree of insecurity and self-assessment disturbance.
Discussion
In the aspect of the functioning of interpersonal relationships, the main factors were the quality of psychovegetative and emotional harmony. The more extraverted person could manage better interpersonal relationships, which manifests in self-confidence, positive self-assessment, self-enforcement while also considering other people´s interests, saying no if necessary, expressing emotions openly and the willingness to take part in relationships personally. Based on our results, we can draw the conclusion that the average value of neuroticism is definitely favourable for interpersonal effectiveness because emotional stability creates a good basis to successfully utilise the behaviour recognition ability based on empathy. The degree of behavioural rigidity proved to be an important factor in the successful working of relationships. Behavioural flexibility enhances the concentration on the partner´s feelings; however, using rigid behavioural patterns is mainly unfavourable because of the presence of the associated insecurity and self-assessment disturbance.
The other important basic dimension of assertiveness is the simultaneous functioning of an other-centred attitude and the enforcement of self-interest. Nursing is a profession in which partners can achieve results by paying attention to each other, and only this way can they avoid the emotional fatigue that threatens their personality and iatrogenesis. It has to be clear for the nurse that throughout the client-centred approach, the use of empathy serves as a personality defence as well because by reading others´ non-conscious signals the threat of emotional drifting and the need for energy wasting self-defence decreases. The development of nurse-patient/client rapport is a mutual interest and its establishment and maintenance that can lead to good results is the responsibility of the professional in her and the help seekers´ interest.
Conclusions
Professional skills development training should focus on the central dimensions of assertiveness, and we think there should be a lot of practice built on own experience to map out and develop personal traits. Work placements provide the opportunity to try and experience the successful treatment of role partners, so we believe we should exploit work placements more than before, e.g. by defining interpersonal competency levels, and by the mentors´ continuous training.
Piśmiennictwo
1. Adams A, Bond S: Hospital nurses´ job satisfaction: individual and organizational characteristics. Journal of Advanced Nursing 2000; 32(3): 536-542. 2. Adams J, Klein LR: Students in nursing school consideration in assessing personality characteristics. Nursing Research 1970; 19(4): 362-366. 3. Addis J, Gamble C: Assertive outreach nurses´ experience of engagement. Journal of Psychiatric and Mental Health Nursing 2004; 11: 452-460. 4. Alberti RE, Emmons ML: Your Perfect Right: A Guide to Assertive Living. California, San Louis: Impact Publishers 1978; 2. 5. Brengelmann JC, Brengelmann L: Deutsche Validierung von Fragebogen der Extraversion, neurotischen Tendenz und Rigiditat. Zeitschrift für Experimentelle und Angewandte Psychologie 1960. 6. Castledine G: Nurses must stop themselves being used by doctors. British Journal of Nursing 1997; 4(6): 234. 7. Deutsh F, Madle R: Empathy, historic and current conceptualizations, measurement and a cognitive theoretical perspective. Human Development 1975; 18: 267-287. 8. Farrel GA: From tall poppies to squashed weeds: why don´t nurses pull together more? Journal of Advanced Nursing 2001; 35(1): 26-33. 9. Gerry EM: An investigation into the assertive behavior of trained nurses in general hospital settings. Journal of Advanced Nursing 1989; 14: 1002-1008. 10. Kilkus SP: Assertiveness among professional nurses. Journal of Advanced Nurses 1993; 18: 1324-1330. 11. Kukulu K et al.: The effects of locus control, communication skills and social support on assertiveness in female nursing students. Social Behavior and Personality 2006; 34(1): 27-40. 12. Lee H: Assertiveness techniques are useful in conflict situations. Nursing Standard 2007; 22(13): 33. 13. McCartan PJ, Hargie ODW: Assessing assertive behaviour in student nurses: a comparison of assertion measures. Journal of Advanced Nursing 1990; 15: 1370-1376. 14. O´Sullivan M, Guilford JP, de Mille R: The measurment of social intelligence. Reports from the psychological laboratory. Los Angeles: University of Southern California 1965; 34. 15. Poroch D, McIntosh W: Barriers to assertive skills in nurses. Australien and New Zealand Journal of Mental Health Nursing 1995; 4: 113-123. 16. Rathus AA: A 30-item schedule for assessing assertive behavior. Behavior Therapy 1973; 4: 398-406. 17. Reece MM: Personality Characteristics and Success in a Nursing Program. Nursing Research 1981; 10: 172-176. 18. Suliman WA, Halabi J: Critical thinking, self-esteem, and state anxiety of nursing students. Nurse Education Today 2007; 27: 162-168. 19. Timmins F, McCabe C: Nurses´ and midwives´ assertive behaviour in the workplace. Journal of Advanced Nursing 2005; 51(1): 38-45.
