*Robert Brodowski1, Bogumił Lewandowski1, 2, Mateusz Dymek1, Iwona Gawron3, Hanna Hartman-Ksycińska2
The application of surgical decompression in relieving the symptoms of thyroid-associated ophthalmopathy
1Department of Maxillofacial Surgery, Frederic Chopin Clinical Hospital No.1 in Rzeszów, Poland
Head of Department: Bogumił Lewandowski, MD, PhD, Ass. Prof.
2Department of Emergency Medicine, Faculty of Medicine, University of Rzeszów, Poland
Head of Department: Bogumił Lewandowski, MD, PhD, Ass. Prof.
3Podkarpackie Oncology Centre in Rzeszów, Poland
Head of Department: Jan Gawełko, MD, PhD
Summary
Introduction: Thyroid-associated ophthalmopathy (TAO) is characterized, among others, by exophthalmos in patients with hyperthyroidism. It occurs in approximately 15% of patients with Graves' disease. The incidence rate of women to men is 4.5:1. The eyeballs protrude outside the bony edges of the eye sockets, causing eyelid retraction, dryness of the conjunctival sac, leading to formation of erosions and ulceration of the cornea, and bulbar conjunctiva. Untreated, the condition can lead to serious damage of the eye, including loss of vision.
Case report: The paper presents a case of a 56-year-old female with ophthalmological complications in the form of exophthalmos in the course of Graves' disease. The patient complained of mild pain in and behind the eyeballs increasing upon eyeball movement, the sensation of eye protrusion, difficulty in closing the eyelids causing dryness of the conjunctiva, and photophobia. The severity of the ophthalmic symptoms posed a serious risk of blindness. Surgical decompression of the orbit was performed by removing the medial wall and the floor of the orbit bone in order to protect the patient’s vision. Post-surgical improvement was observed not only in the local condition, but also in the cosmetic effect.
Introduction
Severe thyroid-associated ophthalmopathy (TAO), also known as severe orbitopathy, infiltrative oedematous exophthalmos, or malignant exophthalmos, is one of a triad of ophthalmologic symptoms of thyrotoxicosis, observed in approximately 15% of cases in Graves’ disease. The incidence rate of women to men is 4.5:1 (1-3). The eyeballs protrude outside the bony edges of the eye sockets, causing eyelid retraction, dryness of the conjunctival sac, formation of erosions and ulceration of the cornea, and bulbar conjunctiva. Swelling and infiltration of the muscles interferes with eye movement, potentially leading to double vision and impaired visual acuity including loss of vision. TAO significantly reduces the patients’ quality of life. Benign changes in the eyesight occur in most patients with hyperthyroidism, impairing the ability to see, yet causing no threat of vision loss as they resolve with the relief of hyperthyroidism symptoms. They do not require special treatment and are limited to being an aesthetic defect (4, 5).
The development of the disease is determined by genetic, environmental and endogenous factors. These include: gender, age, with the peak of incidence falling between 50 and 70 years of age, smoking, thyroid disorders, both hyperthyroidism and hypothyroidism, and radioiodine therapy (1).
The pathogenesis of TAO is the presence of THS receptor (TSHR) antigen in the follicular epithelial cells of the thyroid and fibroblasts of the orbits, skin and orbital preadipocytes. It is assumed that T cells are directed against a common antigen, and triggered by the influence of circulating adhesion retrobulbar proteins infiltrate extraocular tissues and oculomotor muscles. The pathogenesis of infiltrative oedematous exophthalmos includes three processes: infiltration, swelling, and subsequent fibrosis (1, 2).
The extraorbital tissue is infiltrated by mononuclear cells, lymphocytes, and activated fibroblasts, cytokines are released (interferon-gamma, tumor necrosis factor, inerleukin-6), production of glycosaminoglycans is increased, and immunomodulatory proteins are released. This process also indirectly affects extraocular muscles. What results is substantially increased content of interstitial tissue and nerve fibers as compared to skeletal muscles. Histopathological changes in oculomotor muscles involve interstitial connective tissue. The process of inflammation in the connective tissue results in a significant change in the volume and function of extraocular muscles. The orbital contents increase as a result of infiltration and tissue oedema, which hinders the venous and lymphatic outflow from the orbit. The intraocular pressure and the pressure on the optic nerve increase. It is the active phase of ocular lesions, leading to a disproportion between the capacity of the orbit and its contents. This results in protrusion of the eyeballs and the impairment of their mobility. The next step is the process of fibrosis, which indicates the transition to the inactive phase (1, 3, 6).
Mangement of infiltrative oedematous exophthalmos is in the first place symptomatically-pharmacological treatment intended to reduce infiltration and swelling of the tissues filling the orbit. A three-stage method of treatment is required: immunosuppressive therapy combined with corticosteroids are recommended in the first stage. Radiotherapy is used in the second stage of treatment. Another method of reducing the pressure on the optic nerve, and increasing the capacity of the orbit is a surgical removal of the wall of the orbit and intraorbital fat called orbital decompression (3, 6). Surgical orbital decompression is applied both in the active and inactive phase, and is used in emergency situations threatening with loss of vision (6, 7). Adjunctive therapy is helpful, which involves the use of topical anti-inflammatory drops and ointments and, where appropriate, drops reducing intraocular pressure, diuretics, higher position of the head during night, darkened or prismatic glasses, and cornea protection. In any case of thyroid dysfunction, treatment aimed at balancing the thyroid function is necessary: thyreostatics in the phase of hyperthyroidism and thyroxine in hypothyroidism (1, 2, 6).
Case report
A 56-year-old female was referred to the Clinical Department of Maxillofacial Surgery from the Ophthalmology Department of Provincial Specialist Hospital in Rzeszów for a surgical decompression of the orbits in the course of severe infiltrative oedematous ophthalmopathy posing a serious risk of blindness. The patient had a 28-year history of Graves’ disease, hypertension, and following strumectomy in 2014 underwent adjuvant therapy.
On admission, the patient complained of mild pain in and behind the eyeballs which increased upon eyeball movement, the sensation of eye protrusion, difficulty in closing the eyelids causing dryness of the conjunctiva, and a gritty sensation under the eyelids. She suffered from photophobia, which manifested, among other things, in her reluctance to leave enclosed rooms. The patient did not report double vision. She was a nonsmoker. The patient complained of unsightly appearance of the face causing her insecurities in social contacts, thus making her fell confined to her home, avoiding family, friends and neighbors, which resulted in a deterioration of the patient’s quality of life.
Swelling and redness of both upper eyelids, redness of the conjunctiva in both eyes, swelling of the lacrimal caruncle in the right eye, and eyelid retraction were found upon clinical examination. The palpebral fissure's length in the right eye was 14 mm, in the left eye – 11 mm. Exophthalmos was unsymmetrical, the examination with Hertel exophthalmometer showed the forward displacement in the right eye to be 32 mm, and in the left eye – 30 mm. Lesions within the corneas were limited to few erosions in the stage of healing, with greater intensity in the right eye, as a result of the treatment of corneal ulcers which was the reason for her admission into the ophthalmology department. Initial optic neuropathy was observed, which was more pronounced in the right eye.
MRI revealed significant thickening of the patient's extraocular muscles, particulary of the superior and medial rectus (superior rectus RE – 13 x 12 mm, medial rectus RE – 8 x 14 mm, superior rectus LE – 11 x 11.5 mm, medial rectus LE – 8 x 11 mm).
Due to the lack of satisfactory improvement after endocrine therapy, the patient was referred for surgical treatment, ie. for orbital decompression, to reduce exophthalmos, improve the outflow of venous blood and lymph from the orbits, and decrease the pressure of orbital tissues on the optic nerve. A major issue for the patient was the aesthetic aspect, which was taken into account while planning the operation.
Under general anesthesia, floor-medial orbital decompression was performed through conjunctival incisions, protecting and saving suborbital nerves. Excess of orbital fat was removed, mainly from the area below the eye. The surgery was completed by applying tarsorrhaphy on the eyelid of the right eye. The patient did well during the surgery. The postoperative course was uneventful, there were no complications in the local wound healing.
Ophthalmological examination on the seventh day after the surgery showed significant reduction in exophthalmos: RE – 27 mm, LE – 24 mm. Slight swelling of the eyelid and conjunctival redness persisted. The patient was discharged from the clinic on the eighth day after the surgery. Continued treatment at the Clinic of Ophthalmology and Endocrinology and periodical follow-up examination at Maxillofacial Surgery Outpatient Centre were recommended.
Check-up examination was conducted to assess the outcome of the operation during the follow-up 4 months after the orbital decompression. The patient did not report any pain around the orbits or sensation of eye protrusion. Closing of the palpebral fissures eliminated conjunctival dryness and the symptoms of photophobia. Improved local condition was observed. Swelling and redness of the conjunctiva decreased significantly. The palpebral fissure's length was RE – 11 mm, LE – 9 mm.
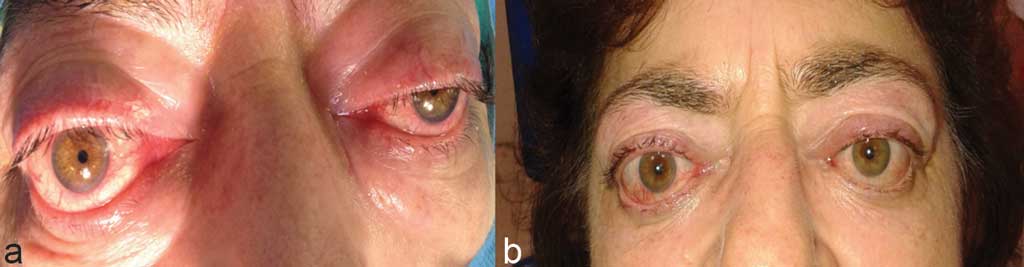
The follow-up after 6 months showed an improvement in the patient's general well-being, resulting from further subjective improvement of the local condition. Swelling and hyperaemia of the conjunctiva remained only slight. The patient was able to close the eyes freely, the palpebral fissures were normal. Exophthalmos was 24 mm in the right eye and 23 mm in the left eye (fig. 1a, b, 2a, b).

Fig. 1a, b. Exophthalmos before surgical treatment (a) and exophthalmos 4 months after surgery (b)

Fig. 2a, b. Unclosing the eyelids before surgical treatment (a) and free closing the eyelids 4 months after surgery (b)
Conclusions
Treatment of patients with thyroid-associated orbitopathy poses a difficult therapeutic problem that requires multidisciplinary approach and cooperation. The symptoms of moderate to severe orbitopathy are long-lasting, distressing, and lower the patient's quality of life (2, 4-6). Despite considerable progress in the field, causal treatment is still not possible, therefore surgery is one of the options available for symptomatic treatment. Generally, the patients tend to avoid surgery. The presented case of the patient who sought “radical” ways to improve her quality of life by consenting to orbitotomy confirms the desirability of surgical treatment in selected patients. Not only does orbital decompression prevent loss of vision in severe cases, but also improves the appearance and aesthetics of the face, thus significantly improving the quality of life of the affected patients.
Piśmiennictwo
1. Sewerynek E: Rozpoznanie i leczenie objawów ocznych w przebiegu chorób tarczycy o podłożu autoimmunologicznym. Forum Med Rodz 2007; 1: 143-151. 2. Baldeschi L, Wakelkamp MJ, Lindeboom R et al.: Early versus late orbital decompression in Graves’ orbitopathy. A retrospective study in 125 patients. Ophthalmology 2006; 113: 874-878. 3. Babiński D, Skorek A, Nałęcz A, Stankiewicz C: Dekompresja oczodołu w przypadku orbitopatii tarczycowej. Otolaryngol Pol 2011; 65(4): 262-265. 4. Goldberg RA: The evolving paradigm of orbital decompression surgery. Arch Ophthalmol 1998; 116: 95-98. 5. Bałdys-Waligórska A, Gołkowski F, Kusnierz-Cabala B et al.: Graves’ ophthalmopathy in patients treated with radioiodine 131-I. Endokrynol Pol 2011; 62: 214-219. 6. Sellari-Franceschini S, Berrettini S, Santoro A et al.: Orbital decompression in Graves’ ophthalmopathy by medial and lateral wall removal. Otolarymgol Head and Neck Surg 2005; 133: 185-189. 7. Pecold K, Krawczyński M: Chirurgia oczodołu. [W:] Pecold K, Krawczyński M (red.): Oczodół, powieki i układ łzowy. Urban & Partner, Wrocław 2005: 115-123.