*Michał Nycz1, 2, Wiktor Krawczyk1, 2, Mateusz Mietła1, 2, Michał Święch1, 2, Zbigniew Lorenc1, 2
Gastrointestinal obstruction in the course of incarcerated Richter’s hernia in the peritoneal drainage catheter tunnel – a case report
Niedrożność przewodu pokarmowego w przebiegu uwięźniętej przepukliny brzusznej typu Richtera w kanale po drenie otrzewnowym – opis przypadku
1Clinical Department of General, Colorectal and Multiple-Organ Surgery, Medical University of Silesia in Katowice
2Department of General, Colorectal and Multiorgan Surgery, Medical University of Silesia, Katowice
Streszczenie
Niedrożność przewodu pokarmowego to stan, w którym dochodzi do zatrzymania pasażu jelitowego. W celu postawienia poprawnego rozpoznania należy wykonać pełne badanie fizykalne oraz diagnostykę obrazową i laboratoryjną. Przepuklina typu Richtera jest rzadką odmianą przepukliny brzusznej, w której obserwowane jest uwięźnięcie w kanale przepuklinowym fragmentu ściany jelita.
Pacjentka zgłosiła się do SOR-u z powodu objawów niedrożności przewodu pokarmowego. Po przeprowadzeniu koniecznych badań stwierdzono uwięźniętą przepuklinę brzuszną typu Richtera w kanale po drenie z jamy otrzewnej, którą zaopatrzono operacyjnie.
Uwięźnięte przepukliny brzuszne należą do jednych z najczęstszych przyczyn niedrożności przewodu pokarmowego. Wśród nich wyróżnia się przepuklinę typu Richtera, która pomimo jawnych objawów klinicznych jest trudna do zdiagnozowania i może lokalizować się nawet w niewielkich ubytkach powłok brzusznych.
Summary
Gastrointestinal obstruction is a condition in which the passage of contents through the intestine is arrested. Thorough physical examination as well as imaging and laboratory diagnosis are needed for a correct diagnosis. Richter’s hernia is a rare form of abdominal hernia in which a part of the intestinal wall is entrapped in the hernial sac.
A female patient reported to the Emergency Department (ED) with symptoms of gastrointestinal obstruction. After performing all necessary investigations, Richter-type hernia was found in the peritoneal drainage catheter tunnel, which was surgically treated. Incarcerated abdominal hernias are one of the most common causes of gastrointestinal obstruction. Richter’s hernia, which poses diagnostic difficulty despite overt clinical symptoms, and may be found even in small defects in the abdominal wall, is one of them.

Introduction
Gastrointestinal obstruction is a condition in which the passage of intestinal contents is arrested. According to standard classification, mechanical and paralytic obstruction is distinguished, depending on its aetiology. Mechanical obstruction is most often caused by growing bowel malignancy, external compression, twisted bowel or intestinal entrapment in the hernial sac. Paralytic obstruction usually results from unstable systemic conditions, such as diabetes mellitus or renal failure. Typical symptoms presented by patients with GI obstruction include abdominal pain, persistent vomiting, as well as gas and stool retention. On physical examination, abdominal distension and metallic peristalsis are frequently found.
Case report
An 80-year-old patient was transferred from the Emergency Room (ER) to the Department of General Surgery due to right hypochondriac pain, elevated inflammatory markers and acute urolithic cholecystitis confirmed by ultrasound. Despite intensive pharmacological treatment, the symptoms did not resolve, which resulted in the decision to perform emergency laparotomy with cholecystectomy. Postoperatively, the pain subsided and the inflammatory markers showed a downward trend. In the following postoperative days, drains were removed from the peritoneal cavity. The diet was extended, the patient was mobilised and discharged home in a satisfactory condition on postoperative day 4.
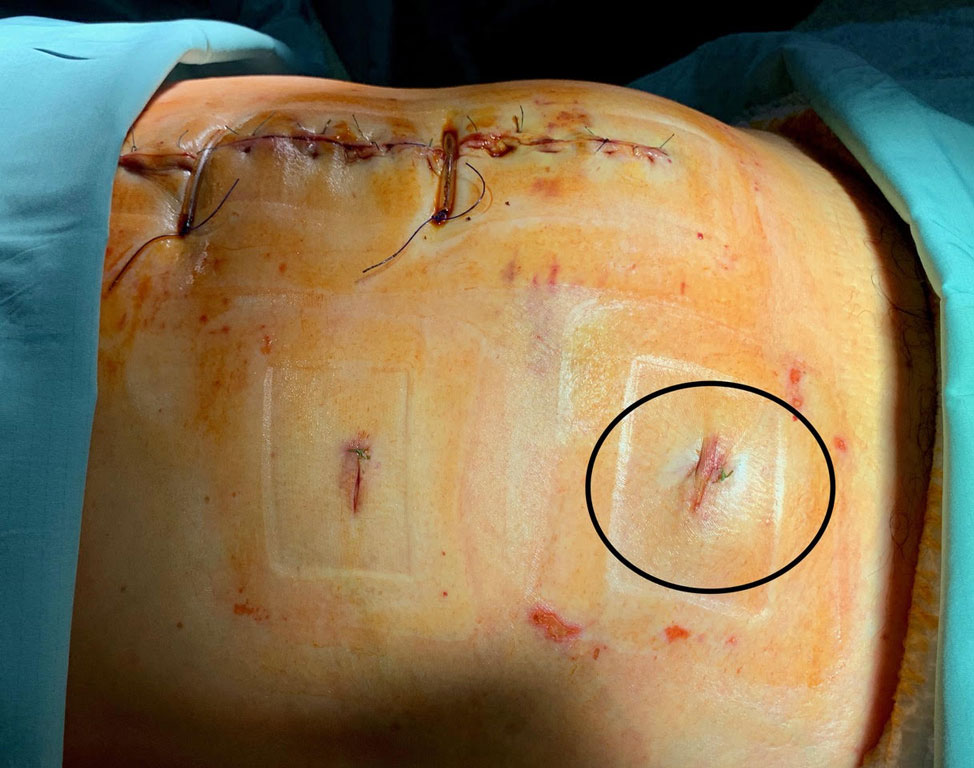
On day 5 after discharge, the patient returned to ER due to persistent vomiting accompanied by gas and stool retention. Physical examination revealed a tender bulging in the right lower abdomen (fig. 1).

Fig. 1. A tender bulging in the right lower abdomen
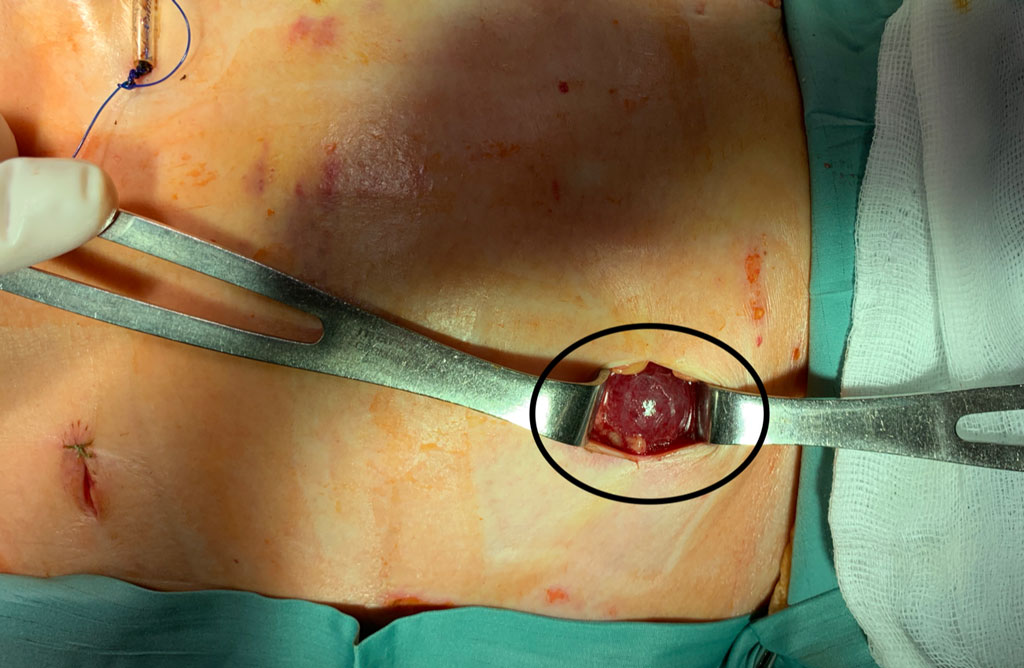
For the purpose of a thorough evaluation, the diagnosis was extended with abdominal and pelvic CT, which showed an incarcerated small bowel loop in the fascia defect located in the right lower abdomen. The patient was prepared to undergo a surgical procedure. Minilaparotomy was performed by accessing through an incision over the painful bulging (fig. 2).
Fig. 2. Incarcerated Richter’s hernia in the peritoneal drainage catheter tunnel (an intraoperative image)
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. da Silva Barbosa RB, Pereira Pinto JC, Duarte L et al.: Small Bowel Obstruction Due to Incarcerated Obturator Hernia: Successfull Surgical Management with Modified Mesh-Plug Hernioplasty. Am J Case Rep 2021; 22: e931398.
2. Sahsamanis G, Samaras S, Gkouzis K, Dimitrakopoulos G: Strangulated Richter’s incisional hernia presenting as an abdominal mass with necrosis of the overlapping skin. A case report and review of the literature. Clin Case Rep 2017; 5(3): 253-256.
3. Regelsberger-Alvarez CM, Pfeifer C: Richter Hernia. StatPearls. Treasure Island (FL): StatPearls Publishing; 2022 Jan.
4. Katragadda K, de Stefano LM, Khan MF: A case of Richter Hernia: a rare entity. ACS Case Reviews in Surgery 2019; 2(3): 5-7.
5. Zhao Ch-Z, Liu L-B: Richter’s hernia in a 5-mm trocar site. J Minim Invasive Gynecol 2020; 27(4): 794-795.
6. Pereira N, Chung ER, Irani M et al.: Incarcerated Omental Hernia at a 5-mm Trocar Site after Laparoscopy. J Minim Invasive Gynecol 2021; 28(3): 384-385.
7. Hayes C, Schmidt C, Neduchelyn Y, Ivanovski I: Obturator hernia of Richter type: a diagnostic dilemma. BMJ Case Rep 2020; 13: e238252.
8. Cinalli M, Selvaggi F, Casolino V et al.: Strangulated Richter’s hernia with caecum necrosis. Case report. Ann Ital Chir 2021; 92: S2239253X21036380.
9. Agegnehu B, Limenh S: Richter’s Type Recurrent Indirect Inguinal Hernia, an Extremely Rare Occurrence: A Case Report. Emergency Medicine 2022; 14: 323-326.
10. Skandalakis PN, Odyseas Z, Skandalakis JE, Mirilas P: Richter hernia: surgical anatomy and technique of repair. Amg Surg 2006; 72(2): 180-184.