Mariusz Kardzis, Janusz Siebert, Maria Wujtewicz, Jan Rogowski
ST monitoring vs cardiac enzymes for the perioperative detection of myocardial ischaemia
Chair and Department of Anaesthesiology and Intensive Therapy,
Head: prof. J. Suchorzewska, Institute of Cardiology;
Head: prof. M. Narkiewicz, Medical Academy of Gdańsk
Summary
The relationship between the creatinine kinase cardiac isoenzyme concentration and total creatinine kinase concentration (CKMB/CK) has been recognized as an useful method of cardiac ischemia assessment. This analysis can be performed in certain time intervals and should be reviewed retrospectively in relation to the ST analysis.
The aim of the study was to assess the realtionship between ST two-leads analysis and CKMB/CK index in fifty patients, scheduled for the coronary bypass surgery. We have chosen for analysis the deepest ST depression, and noted its duration time. Blood for CKMB and CK concentration was taken at 6, 12 and 36 hours after surgery. In nineteen patients the ST depression was noted, usually during first six hours after surgery. Its maximum depth was 4.7 mm and maximum duration time 126 minutes (mean 97 minutes). The CKMB/CK index larger than 1:10 was found in ten patients. There was no correlation between ECG and biochemical data. The only positive correlation (r=0.67) was found between the ST depression exceeding 1 mm and 12 hours-delayed CMKB/ CK index larger than 1:10.

Stabilisation of the lowered ST segment together with an increased CKMB/CK ratio facilitates the differential diagnosis between transient ischaemia and myocardial infarction. In patients with proven coronary artery stenosis, the ineffective attempts of pharmacological treatment provide an indication for bypass surgery. Good results of this therapy caused widening of indications for surgery in coronary heart disease. Nowadays also the patients with increased operative risk are included: elderly persons, patients with widespread atheromatic vascular changes or lowered ejection fraction values. Myocardial ischaemia is a frequent complication in the perioperative period. Its diagnosis involves enzymatic activity testing, among which the ratio of MB-isoenzyme of creatinine kinase (CKMB) to the total creatinine kinase (CK) activity in serum is routinely used. As enzymatic tests become positive with a certain latency to the myocardial ischaemic episode, methods of "on-line" monitoring are being searched for. One of these methods is a continuous analysis of the ST segment deviation in ECG tracing. The lowering of ST by 1mm (i.e. 0.1 mV), parallel or downward oblique to the baseline, lasting more than 0.08 s in subsequent cardiac evolutions, is suggestive of myocardial ischaemia.
The aim of the present study was to assess the usefulness of ST segment monitoring and its correlation with CKMB/CK activity in the diagnosis of myocardial ischaemia in patients after coronary artery bypass graft.
PATIENTS AND METHODS
After obtaining permission from the local Ethical Committee the study was carried out in 50 patients (31 men, 19 women), aged from 41 to 72 years (mean 57), scheuled for coronary bypass surgery. Patients in whom the preoperative ECG tracings demonstrated conduction disorders were not included in the study. Surgery was performed in extracorporeal circulation, moderate hypothermia (28-30°C) and haemodilution (haematocrit 23-24%). Myocardial protection was achieved by cold cardioplegy and superficial cooling of the heart by instillation of 0.9% NaCl solution at 4°C directly to the pericardial sac. The duration of extracorporeal circulation depended on the type of surgery and ranged from 53 to 260 minutes (mean 150 min) (Tab. I). After the operation the patients were transferred to the Intensive Therapy Unit. They were artificially ventilated until the return of spontaneous breathing and full consciousness. The mean time of postoperative artificial ventilation was 16 hours. ECG monitoring, with ST segment analysis, was maintained during the first 3 postoperative days. Samples of blood for CKMB and CK activity analysis were drawn at 6, 12 and 36 hours after surgery. Values of CKMB activity were accepted as normal if they did not exceed 1/10 of the total CK activity. The results were analysed in order to determine:
maximum value of deviation of ST segment and its duration,
maximum values and duration of increased CKMB/CK activities ratio,
possible relationship between ST segment deviation and increased CKMB/CK ratio,
correlation of the results with clinical condition of the patient.
Table I. The duration of coronary bypass surgery
| Duration of surgery (min.) | Duration of perfusion (min.) | Number of
bypasses |
| 165-645 | 53-260 | 1-6 |
Table II. The value and duration of ST segment depression in the postoperative period
| Time intervals (ECG monitoring) | Maximum ST depression (mm) | Duration of maximum ST depression (min.) | Mean duration of ST depression (min.) |
| 0-6 hours | 4.7 | 120 | 97 |
| 6-12 hours | 2.6 | 16 | 27 |
| 12-36 hours | 3.4 | 72 | 67 |
Results
1. ST segment analysis during continuous ECG monitoring.
The ST segment and enzymatic blood tests were evaluated 6, 12 and 36 hours after the operation. With time, the number of patients presenting symptoms of myocardial ischaemia gradually diminished (Fig. 1). The maximum depression of the ST segment was noted 6 hours after surgery (4,7 mm) but its duration was equally long in the immediate postoperative period and between 6th and 12th postoperative hours (range: 0-360, mean 97 minutes). From this time onwards, ST depression was similar in value, but lasted less time (range: 0-84, mean: 27 minutes) (Fig. 2).
2. Enzymatic activity
At repeated enzymatic assays (6, 12 and 36 hours after surgery) the number of patients with elevated CKMB/CK activity ratio gradually diminished (Tab. II). The increased ratio was most frequently observed in the immediate postoperative period, until the 6th postoperative hour.
No correlation was found between the ST segment deviation (value and duration) and CKMB/CK activity ratio (correlation factor r = 0.34) in corresponding time intervals (Fig. 3).
A positive correlation (r = 0.67) was documented between the duration of ST depression and CKMB/CK value 24 hours after surgery (Fig. 4). Neither clinical signs nor symptoms of myocardial infarction were present in any patient, which was confirmed by later diagnostic tests.
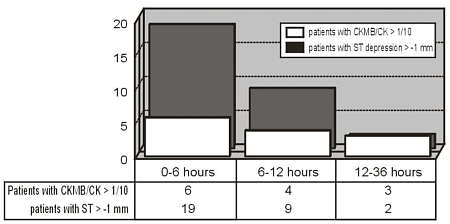
Fig. 1. Duration of ST depression> 1 mm and rate of CKMB/CK incidence> 1/10.
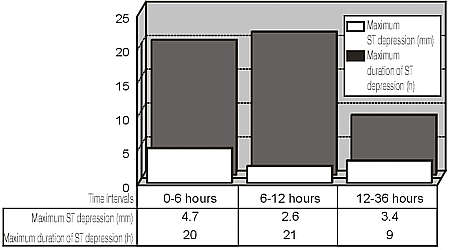
Fig. 2. The duration and value of ST segment depression.
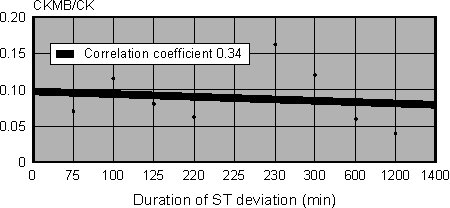
Fig. 3. Correlation between ST depression during the first 12 postoperative hours and CKMB/CK ratio 12 hours after surgery.

Fig. 4. Correlation between ST depression during the first 12 postoperative hours and CKMB/CK ratio 36 hours after surgery.
DISCUSSION
Monitoring of possible myocardial ischaemia in patients after cardiac surgery should provide the continuous "on-line" information, be simple and possibly noninvasive, and should not interfere with postoperative nursing and physiotherapy.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Ansley D. M., O'Connor J. P., Merrick P. M.: On line ST - segment analysis for detection of myocardial ischaemia during and after coronary revascularization. Canadian Journal of Anesthesia 1996, 43, 995-1000
2. Jain U: Electrocardiographic determination of perioperative myocardial ischemia and stunning. Journal of Cardiac Surgery 1994, 9, Suppl. 3, 314-416
3. Mahmarian J. J., Steingart R. M., Forman S.: Relation between ambulatory electrocardiographic monitoring and myocardial perfusion imaging to detect coronary artery disease and myocardial ischemia: an ACIP ancillary study. The Asymptomatic Cardiac Ischemia Pilot (ACIP) Investigators. Journal of the American College of Cardiology 1997, 15, 764-769
4. Hogue C. W. Jr., Herbst T. J., Pond C.: Perioperative myocardial ischemia. Its relation to anatomic pattern of coronary artery stenosis. Anesthesiology 1993, 79, 514-524
5. Friedman D. L., Kesterson R., Puelo P., Wu A. H., Perryman M. B.: Recombinant creatine kinase proteins and proposed standards for creatine kinase isoenzyme and subform assays. Clinical Chemistry 1993, 39, 1598-1601
6. Schwartz J. G., Prichoda T. J., Stuckej J. H., Gage C. L., Darnell M. L.: Creatine kinase MB in cases of skelatal muscle trauma. Clinical Chemistry 1998, 34, 898-901
7. Wu A. H., Wang X. M., Gornet T.G., Ordonez-Lianos J.: Creatine kinase MB isoforms in patient with skelatal muscle injury: ramification for early detection of acute myocardial infarction. Clinical Chemistry 1992, 38, 2396-2400
8. Wu A. H., Feng Y. J., Contois J. H., Pervaiz S.: Comparison of myoglobin, creatine kinase MB znd cardiac troponin I for diagnosis of myocardia infarction. Annual Clinical Laboratory Science 1996, 26, 291-300
9. Kutsal A., Saydam G. S., Yucel D., Balk M.: Changes in the serum levels of CKMB, LDH, LDH1, SGOT, and myoglobin due to cardiac surgery. Journal of Cardiovascular Surgery Torino 1991, 32, 516-522
10. Grychowska J.: Wartość monitorowania enzymatycznego w okresie okołoperacyjnym u chorych po bezpośredniej rewaskularyzacji mięśnia sercowego. Praca doktorska. AM Łódź rok 1994
11. Jawien J., Naskalski J., Dziatkowiak A., Szczelik A.: Diagnostyka zawału okołooperacyjnego serca w zabiegach pomostowania aortalno-wieńcowego. Kardiologia Polska 1993, 39, 478-485
12. Kirklin J. K.: The postperfusion syndrome: Inflammation and the damaging effects of cardiopulmonary by-pass; in: Cardiopulmonary by-pass: Current concepts and controversies (Ed. Tinker J. H.). W. B. Saunders Company, Philadelphia 1989
13. Mc Daniel H. G., Reves J. G., Kouchoukos N. T., Smith L. R., Rogers W. L., Samuelson P. N., Lell W. A.: Detection of myocardial injury after coronary bypass grafting using a hypotermic, cardioplegic technique. Annals of Thoracic Surgery 1982, 33, 139-145
14. De Puey E. G., Aessopos A., Monroe L. R., Hall R. J., Thompson W. L., Sonnemaker R. E., Burdine J.: Clinical utility of a two site immunoradiometric assay for creatine kinase MB in the detection of preoperative myocardial infarction. Journal of Nuclear Medicine 1983, 24, 703-714
15. Miller D. D.: Evaluation of the patient with stable angina following coronary artery by-pass surgery. Cardiovascular Clinical 1991, 21, 137-167
16. Rotman B., Eber B., Dusleang J., Rigler B., Klein W.: Coronary revascularisation: influence on ventricular arrhythmia. Clinical Cardiology 1990, 13, 11-13
17. Pervaiz S., Anderson F. P., Lohmann T. P., Lawson C. J., Feng Y. J., Waskiewicz D., Contois J. H.: Comparative analysis for detection of myocardial ischemia during and after coronary revascularization. Canadian Journal of Anaesthesia 1996, 43, 995-1000
18. Cunningham A. J.: Myocardial ischemia - association with perioperative cardiac morbidity. Yale Journal Biology and Medicine 1993, 66, 339-348
