© Borgis - New Medicine 2/2001, s. 4-5
Mieczysław Chmielik, Anna Gabryszewska
The influence of diseases of the nose on the functioning of the Eustachian tube and middle ear
Department of Paediatric Otorhinolaryngology, The Medical University of Warsaw
Head of Department: Prof. Mieczysław Chmielik, MD.
Summary
The functions of the Eustachian tube and the middle ear are associated with nasal patency. All disorders, both acquired and congenital, which decrease nasal patency, have an impact on the function of the middle ear. The most common reasons for nasal obstruction in children include inflammatory and allergic diseases of the respiratory tract, adenoidal hypertrophy and septum deviation. Therapeutic management in children differs from that in adults.
The nasal cavity with the paranasal sinus system forms, with the tympanic cavity, the Eustachian tube and the pneumatic cells of the mastoid process, an anatomical and functional totality. Thus, disorders of the upper respiratory tract (u.r.t.) influence the functioning of the hearing organs including the Eustachian tube and tympanic cavity. The most frequent reason for child referral to a physican is acute viral infection of the upper respiratory tract. This is normally due to congenital immunological factors in childhood and harmful environmental factors. Infections of the u.r.t. may appear as a primary disease or as a complication of congenital defects, of trauma, of neoplasms, or of general disease. In the case of acute, commonly viral, infections of the u.r.t. we treat according to a standard scheme which includes antinflammatory and antibacterial treatment.
If the symptoms don´t disappear after 3-7 days, it becomes necessary to perform additional examinations to assess local and general conditions affecting the pathology, the type of pathogen, and other factors.
If the infection is prolonged for more than 3 weeks, or recurs frequently it is neccessary to perform particular clinical diagnostic tests: microbiological examination, microscopy, laboratory investigation and others.
Diagnostic examination beyond basic tests should include:
1. The immunologic condition of the patient: assessment of the level of immunoglobulin and subpopulation of lymphocytes evaluated by monoclonal antibodies.
2. Radiolgical examinaton, especially computed tomography of the facial skeleton at sagittal sections. On the scan one should see congenital or acquired defects of the lateral wall of the nasal cavity. These anomalies can lead to prolonged sinusitis.
3. Assess the patency of the nose. This is a difficult issue because the air flow through the nose is a subjective sensation. The flow resistance should be measured by rhinomanometry, which is a valuable but not always sufficient way to assess the function of the nose. Similarly, we can use acoustic rhinomanomery which is an objective way. The most accurate method rhinoresistometry, has been proposed by rhinologic Centre in Greisfald which assesses the relation between the laminar and turbulent flow in various parts of the nasal cavity.
4. Ciliary clearance – we can recognize rare but severe disorders such as immobile cilia syndrome.
5. Cytology from the mucus of the nose is a valuable method when it is carried out by an experienced centre. The results of this examination can provide useful information about the aetiology.
6. Examination of the nasal cavity and the radiological examination can give information about the anatomical strucures and source of drainage of secretions.
In the case of confirmed obstructive changes of the u.r.t. it will be necessary to treat pharmacologically or surgically to remove the obstruction. If allergic reactions are recognised, the child should be referred to an allergologist.
Septal deviations can develop due to trauma or congenital defects, and consequentty leads to prolongend sinusitis hypertrophy of the adenoidal tissues. This is the most common reason for obstruction of the nose, and requires surgical treatment (picture 1).
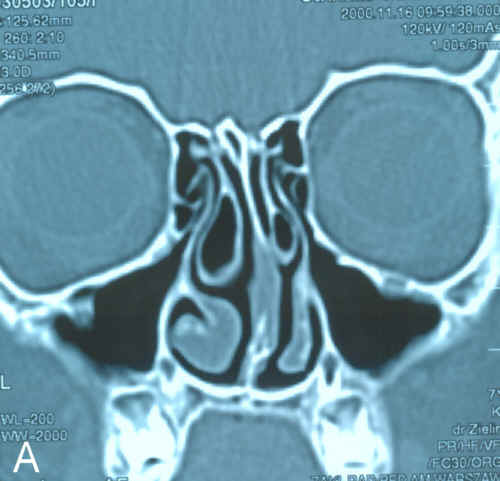

Picture 1. Computed tomography of paranasal sinuses revealing a difference in structure in the lateral wall of the nose which can impact on the patency of ostio – meatal complex and thus allow prolonged infection. A – concha bullosa; B – Haller´s cells.
At this point we must mention therapeutic limitiens in patients at developmental age as compared to adults.
Antibiotics should only be administered in cases where we are sure that we are dealing with bacterial aetiology of infection.
Administration of mucosal decongestant drugs should be reduced to a minimum, and it is best if applied by the laryngologist using a cotton – tipped applicator only in the region of the natural ostia of the sinuses and the pharyngeal ostium of the Eustachian tube.
Surgical treatment should be performed in centres which have proper equipment for this type of operation, and highly – qualified staff.
The operations should be performed as economically and conservatively as possible. It is important to note that the age of the child is not a contraindication to the performance of any operation improving defects of the septum or lateral wall of the nose.
Operations which improve nasal patency and viability of the Eustachian tube include:
1. Operations with regard to lymphoepithelial tissue
– adenotomy,
– adentonsillotomy.
2. Operations with regard to the nose and the nasal septum:
– septoplasty,
– rhinoplasty.
3. Operations concerning the lateral wall of the nose:
– microdebrider usage,
– argon plasma coagulation,
– laser usage.
After succesful treatment of acute or prolonged disorders of the upper respiratory tract, we expect to see an improvement in the functioning of the Eustachian tube. If there is not a sufficient improvement and otitis media with effusion is seen, we must begin to use a plan of management, which may include perflation of the Eustachian tube, tympanocentesis, and the use of ventilation tubes.
Piśmiennictwo
1.Fujita A., Honjo I., Kurata K., Gan I., Takahashi H.: Refractory otitis media with effusion from viewpoints of eustachian tube dysfunction and nasal sinusitis. Am. J. Otolaryngol. 1993 May – Jun;14(3):187-90. 2.Knight L.C., Eccles R., Morris S.: Seasonal allergic rhinitis and its effects on eustachian tube function and middle ear pressure. Clin. Otolaryngol. 1992 Aug;17(4):308-12. 3.Thompson A.C., Crowther J.A.:Effect of nasal packing on Eustachian tube function. J. Laryngol. Otol. 1991 Jul; 105(7):539-540. 4.Low W.K., Willatt D.J.: The relationship between middle ear pressure and deviated nasal septum. Clin. Otolaryngol. 1993 Aug;18(4):308-10. 5. Sismanis A.: Otitis media: the pathogenesis approach. Assessment and treatment of associated upper respiratory tract pathology. Otolaryngol. Clin. North. Am. 1991 Aug; 24(4):947-55. 6.Fireman P.: Otitis media and eustachian tube dysfunction: connection to allergic rhinitis. Allergy. Clin. Immunol. 1997 Feb;99(2):S787-97. 7.Buchman C.A., Doyle W.J., Swarts J.D., Bluestone C.D.: Effects of nasal obstruction on Eustachian tube function and middle ear pressure. Acta. Otolaryngol. 1999; 119(3):351-5. 8.Van Cauwenberge P., Derycke A.: The relationship between nasal and middle ear pathology. Acta. Otorhinolaryngol. Belg. 1983; 37(6):830-41. 9.Stackpole S.A., Edelstein D.R.: The anatomic relevance of the Haller cell in sinusitis. Am. J. Rhinol. 1997 May – Jun;11(3):219-23.
