© Borgis - New Medicine 2/2008, s. 40-44
*Dariusz Gutek
Software to Support a Medical Practitioner in an Endoscopic Laboratory
Lublin University of Technology
Summary
The article presents a concept of applying supporting software for a physician who does endoscopic examination. The proposed system archives examination results together with the picture and video materials and also stores a handy database of descriptions and diagnoses. The discussed software focuses on changes of a polyp character. When the examination is done it is possible to consult a rule expert system that makes a separate application.
Introduction
The application of expert systems in Polish hospitals is rather inconspicuous. A few systems that support medical practice have already been implemented, among them: an expert system to support a diagnosis of benign prostate hypertrophy (1), and the medical expert system BayEx-DYSRAFIE (2). Some information technology projects concerning endoscopic testing such as a system for computer-supported endoscopic tests (3) or systems for computer visualization of the tests (4) have also been elaborated. However, none of the mentioned systems operates real-time in any specific endoscopic laboratory. The projects were either abandoned or completed a long time ago (1999 for (1) and 2001 for (3)) or remained at an experimental stage. Some of the research works were performed using packages that proved not to be optimal such as the Java language platform application for graphical operations, which did not make an effective solution because of excessive memory use by the Java virtual machine itself as well as because of a specific code performance from the level of a precompiled format (3).
The system proposed by the present author is not as platform-wise portable like Java language applications but is easier to program, use, correct and implement. Graphic stations of the system operate within the MS Windows environment, the server is based on one of the Linux distributions (or the MS Windows 2003 Server), access platform – PHP language and MySQL databases, owing to which access to test results via WWW of the hospital LAN and then WAN has been automatically implemented. Architecture of the existing LAN (example implementation in an endoscopic lab of Public Clinical Hospital No. 1 in Lublin) that connects graphic stations with a multimedia server (1Gb/s (5)) has also been altered.
Such a system is easy to implement and integrate
with the existing hospital equipment from where information in the graphical file form can be obtained or when it is only used as access stations to the results. The proposed system stores not only single pictures of various kinds but also videos recorded during USG or endoscopic testing, which makes it possible to comparatively quickly verify the condition of a patient and efficiently compare current results to previous ones. The quality of such verification and comparison based on recorded visual material is much higher than for previously practiced analyses of text documents. It also reduces overall costs of multiple testing performed for the same patient who happened to be diagnosed and treated in several medical units and by various doctors. It is worth mentioning that such a procedure is also more comfortable for the patient, who sometimes can be saved too numerous medical interventions. This is possible owing to a database where results and records of previous examinations are stored together with descriptions attached by the medical staff. Only authorized persons are granted access to the database and the patient records include information of the performed medical testing with the option to see not only its results but also its course if it was performed by other physicians in some other medical establishments (hospital departments). Such information can be very helpful in the course of further treatment or when evaluating the treatment effects.
Objective of the project
The presented research work has aimed at elaborating a computer application to support a medical practitioner who performs endoscopic testing. The application aside with archiving of the test results supports loading descriptions and generating reports that include image and text material. Based on the entered data the implemented expert system would suggest possible interpretations for the observed pathological changes.
Materials and methods
Rapid technological development and the great amounts of information that a medical practitioner can get about the condition of a patient makes support for decision-making in medicine more and more essential. When data and results concerning the condition of a patient come from various sources their analysis can be difficult. In such a situation a computer system for decision-making support can be very helpful. Such systems can analyze archival data and select the most important information out of them in a comparatively short time. They indicate deviations from correct values and suggest a diagnosis or possible procedures to be applied. They also can quickly compare actual test results to archived data and determine improvement or worsening of a patient´s condition.
It should be remembered that the decision-making process is very complex, especially when it concerns treatment, application of medicines or other clinical decisions.
There are many techniques that can be used in elaborating a system for supporting clinical decisions, including: clinical algorithms, expert systems based on rule knowledge, fuzzy systems, systems based on a theory of approximate sets, systems based on conditional probability, and others (6).
Presently, it is clinical algorithms that are the most often applied systems in hospitals and clinics. They define a list of consecutive actions that should be performed during medical procedures. They constitute one of the simplest tools to support medical staff in their work.
The discussed project has aimed at elaborating such a system whose databases would contain data obtained from procedures performed according to assumed algorithms. Such procedures ensure pretty good repeatability of results obtained for the patients and make it possible to compare actual results to the archival ones.
An expert system should be characterized by the following properties:
– all information pieces concerning the area of interest are recorded in a formalized and ordered way and form a structure called a knowledge base,
– processing of the knowledge base data is performed by an adequately developed part of the program called an inference machine,
– the system is equipped with a mechanism that makes it possible to communicate with the user – a user interface.
Easy access to the information and compiled knowledge of many experts are the main advantages of using the expert system (fig. 1). In the discussed case it is necessary to supplement the system with calculation models that can quickly provide quantitative information about the tested phenomena. Another valuable property of the expert system is the possibility of perpetual updating of the knowledge base and a reduction of expertise opinion costs (6).
Fig. 1. Schematic diagram of the expert system.
Rules of the expert system for the interpretation of the obtained knowledge
When elaborating an expert system that cooperates with knowledge databases it should be remembered that a description of the input data should be unambiguous (e.g. by a colour specification), invariable (e.g. by mathematical functions describing shape or regularity of a coat), or concern a determined quantity such as the diameter of a polyp or its volume (fig. 2) (7).

Fig. 2. Example screen of the new software that determines measurable characteristics of pathological changes based on a pattern.
In order to make the discussion of the elaborated expert system very clear, one of the possible anomalies that can occur in the human digestive system, that is polyps, has been selected for descriptive purposes.
Based on the performed observations the following data about polyps have been selected to be stored in the database: location of the polyp (description or a selection field listing digestive system parts), height (mm), diameter (mm), volume (mm3), stalk length (mm), colour (selection field or colour pattern), bleeding or not (selection field), regularity of shapes (selection field), preliminary cancer classification (name if the polyp resembles some known cancerous form), ingrowth depth (mm – update field to be filled e.g. by actual USG test results), ulcerous condition (selection field/check box), blood supply (selection field), comments (description field).
An analysis of changes and pathologies that form a basis for the discussed system elaboration yields example rules for an example system to be based on, such as the following ones:
Rule 21: If a polyp is of porous structure it may be a cancerous change.
Rule 22: If a polyp diameter exceeds some determined quantity (considered to be big) it qualifies for polypectomy (removal) – the rule is valid for its volume as well.
Rule 23: If a polyp is well blood-supplied it should be removed in small portions.
Rule 24: If a polyp is distinctly pedunculated (distinct stalk) it should be removed.
Rule 25: If a polyp is of insignificant dimensions and smooth surface its location should be marked in the database and it should be subject to further observation.
The formulated rules have to be complemented by functions elaborated on the basis of endoscopic lab research, literature and expert knowledge. Such functions based on fuzzy logic can determine whether a diameter or volume of a polyp can be considered to be big (fig. 3) or what curvature describes porosity of a structure.
Fig. 3. Example membership function distribution in a fuzzy system illustrated by polyp geometry.
Obviously, general condition and age of a patient should always be taken into account, as e.g. an intervention in the digestive tract of a 75-old patient may be a futile effort.
PC-Shell [8] has been selected as a tool to elaborate the expert system. It is a shell of a hybrid architecture, which means that it combines various methods of problem solving and knowledge representation. What makes the PC Shell system very interesting is a built-in and fully integrated neural network simulator. Another interesting feature of the system is its table structure, which makes it possible to divide a big knowledge base into smaller topic-oriented modules – so called knowledge sources.
An example of the new expert system operation
Knowledge base description language of the PC Shell system is meant for a formal description of expert knowledge in a specific area. Languages of that type are used mostly by knowledge engineers. Their basic task is to obtain specific knowledge from a specialist using techniques elaborated based on theory and practice of the expert system domain and to encode it by means of some formal language.
Knowledge base sources of the presented system are within the table architecture. The PC-Shell system makes it possible to use in one application an unspecified amount of various knowledge bases as knowledge sources.
For the sake of full comprehensibility, knowledge sources have been classified in the following way:
– anamnesis,
– post-examination observation.
The anamnesis source expects responses to the following questions:
1. Does an increased susceptibility to bleeding occur, especially in small injuries?
2. Does copious bleeding occur, e.g. after tooth extraction?
3. Do extensive ecchymoses form even in small injuries?
4. Have similar symptoms occurred with any other family members?
5. Have allergy symptoms to any foods or medicines ever occurred?
6. Are any medicines that influence blood coagulability, like aspirin or dicumarol, taken?
7. What is the age of the patient?
Responses to the above given questions are analyzed and then the knowledge base rules determine whether health condition, medicines taken and the patient´s reaction to the disruption of tissue continuity permit polypectomy.
Together with knowledge sources, facets have been defined. A facet is a set of declarations that refer to selected attributes. A block of facets comprises a list of all attributes used in the knowledge base including the ones contained in knowledge sources. Not all attributes have to be described by facets but all of them have to be declared in the facet block. The PC-Shell system along with text declarations also admits pictures, sounds and videos as attributes.
Facet picture makes it possible to relate attributes with pictures e.g. in the form of bitmaps.
picture filename
picture { file_1,..., file_n}
For example:
susceptibility to bleeding:
query „Does increased susceptibility to bleeding occur, especially in small injuries?”
val oneof {„yes”, „no”}
picture „blood.jpg”;
The picture is automatically presented when a query concerning the attribute related to the picture occurs and in the case when a solution to the query concerning an attribute related to the picture appears. The system makes it possible to assign a picture directly to an attribute or each of the quantities is assigned a separate picture.
Facet video makes it possible to relate attributes with animations (videos), e.g. avi or mpg files.
video filename
video {file_1,..., file_n}
For example:
polyp_size:
query „Can the polyp be considered to be small and smooth-surfaced?”
val oneof {„is small and smooth-surfaced”, „no”}
video „2.avi”;
Animation can be assigned to an attribute in the same way as it is in the case of a picture. Types of animations used depend on controllers installed in the system and responsible for the file presentation.
The elaborated system perfectly realizes the discussed features and when asking a question illustrates it with a picture (fig. 4) or with a video sequence (fig. 5).
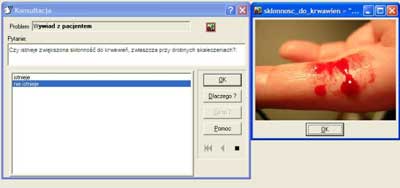
Fig. 4. Query illustrated by a picture.

Fig. 5. Query illustrated by video material.
Based on the entered information the system infers that polypectomy can be performed for the patient in question (fig. 6) or that the surgery is not recommended, or the user is informed (fig. 7) that on the basis of available data the system cannot unambiguously decide on the question.
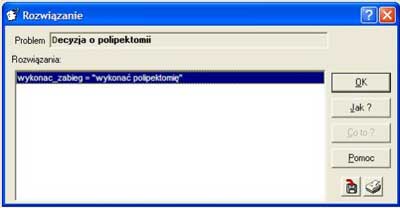
Fig. 6. Message of the system – the surgery can be performed.

Fig. 7. Message of the system – available data are not sufficient to make a decision on the question.
The presented example shows that having adequately prepared data and a configured expert system shell it is possible to elaborate an application that can be used to support less experienced medical staff in their practice or to evaluate decisions that have been made. The selected tool makes it possible to directly combine text query of the system with graphical examples in the picture or video forms, which makes the work easier and considerably enhances quality of the given responses.
Conclusions
Applications that store graphical and video data are finding wider and wider use in various areas of life. All noted world companies dealing with information technologies develop software that makes it possible to select, process and store medical information in the form of images. Implementation of the proposed solutions in hospitals depends on the attitude of medical staff to the problem of archiving medical image data. The rate of storing and exchange of information from devices that return measurement results in graphical or video forms is also of considerable importance. An exchange of such information could reduce redundancy in performance of medical tests for the same patient by various hospital units. The proposed expert system aside with supporting diagnostic processes in the observed cases could also support comparative diagnosis of similar disease cases recorded and classified in a hospital database.
The proposed system is easy to implement and integrate with the existing hospital equipment from where information in the graphical file form can be obtained or when it is only used as access stations to the results. The application stores not only single pictures of various kinds but also videos recorded during USG or endoscopic testing, which makes it possible to relatively quickly verify the condition of a patient and efficiently compare current results to previous ones. The quality of such verification and comparison based on recorded visual material is much higher than for previously practiced analyses of text documents. It also reduces overall costs of multiple testing performed for the same patient.
Piśmiennictwo
1. Makal J, Nazarkiewicz A, Oniśko A, et al.: System ekspertowy do wspomagania diagnozy łagodnego przerostu prostaty, PAR, Warszawa 7-8/2004; s. 193-196. 2. Valenta MA, Zygmunt A: Medyczny system ekspertowy BayEx-DYSRAFIE, Telemedycyna 2001, II krajowa konferencja naukowa, Łódź 2001; s. 67-72. 3. Krawczyk H, Knopa R, Mazurkiewicz A: Komputerowe wspomaganie badań endoskopowych [w:] Biocybernetyka i Inżynieria Biomedyczna 2000, Tom 7, Systemy komputerowe i teleinformatyczne w służbie zdrowia, EXIT, Warszawa 2002; s. 82-97. 4. Bartz D, Skalej M: VIVENDI - A Virtual Ventricle Endoscopy System for Virtual Medicine. In Data Visualization (Proc. of Symposium on Visualization), s. 155. 166, 324, 1999. 5. Gutek D: The computer system of medical picturing, Materiały IX International PHD Workshop, Wisła 2007. 6. Michnikowski M: Systemy wspomagania decyzji, w: Informatyka medyczna, (Red. R. Rudowski), PWN, Warszawa 2003; s. 93-117. 7. Gutek D: Measurements of the size of losses and polyp diameters on basis of endoscope images, 4th International conference of PHD students, University of Miskolc, Hungary 2003. 8. PC-Shell wersja 4. 1. 0. 0. Plik pomocy programu, AITECH, http://aitech.pl/, 2004.
