© Borgis - Nowa Stomatologia 3/2005, s. 115-117
Joanna Politowska1, Adam Okoń2, Elżbieta Jodkowska2
Multidisciplinary treatment of a case of dentine dysplasia. A case report
Multidyscyplinarne leczenie przypadku rozpoznanej dysplazji zębiny
Zakład Stomatologii Zachowawczej IS AM w Warszawie
Kierownik Zakładu: dr hab. n. med. Elżbieta Jodkowska 1Koło Naukowe przy w Zakładzie Stomatologii Zachowawczej IS AM w Warszawie 2Zakład Stomatologii Zachowawczej IS AM w Warszawie

INTRODUCTION
A patient who presents with dentin dysplasia is always included in the high risk group of losing teeth when young. When such cases are diagnosed they require additional care from the dentist: the patient should be constantly monitored and offered consultations with doctors of many specialties such as maxillofacial surgeons, periodontists, orthodontists and prosthetists. It is true that almost every patient comes in contact specialities they represent in his life: for example, with conservative dentistry when he is edentate, with orthodontics as a youngster, and usually with prosthetics and periodontics in the later period of his life. There are also other situations like dental trauma or a complicated extraction requiring the assistance of a dental surgeon. The question is: must patients with dentine dysplasia be monitored from the earliest years of their lives?
Dentine dysplasia is a disorder of the structure of the hard tissue of the tooth affecting mostly dentine. It is hereditary condition. It is a heritable autosomally. It affects one patient in the population of one hundred thousand. The aetiology of this disease is yet unknown. The migration of the epithelium cells of Hertwig´s sheath to the tooth germ and inducing odontoblasts to differentiate and apposition dentine can be the cause. Lesions are seen in deciduous dentition, but can also be present in permanent dentition (1, 2, 3, 4, 5, 6). Such lesions affect the crown of the tooth, its roots or both. Attributes of dentine dysplasia include: (1) proper shape and size of the crown, poor mineralization of teeth, susceptibility to attrition and sometimes increased mobility. Radiographically, this disease is manifested by: lack of root canals, the presence of dentinoma, presence of periradicular pathology and thinning of the cementum of the root. Dentine dysplasia mostly is divided into two types (1, 2, 3, 6).
Type I – concerns changes in both deciduous teeth and permanent teeth that clinically have proper shape, color and hardness. Radiographically, milk teeth demonstrate total obliteration of pulp chambers and canals, permanent ones are characterized by crescent-like shape of obliterated chambers and the presence of periapical pathology in generally caries-free teeth (5, 7, 8, 9). According to Carroll et al. type I dentine dysplasia is divided according to the progression of dysplastic changes as seen on radiographic examination. The following subtypes were proposed: 1a, 1b, 1c, 1d (4, 5). DD1a – total pulpal obliteration and no root development; DD1b – with crescent-shaped remnants of the pulp chamber and minimal root development; DD1c with two crescent-shaped radiolucent lines and significant but incomplete root development; DD1d with radiographically visible pulp chambers, oval pulp stones and bulging roots
Type II – lesions in primary dentition and permanent dentition differ. Milk teeth have brownish or blue-brown discoloration, and are susceptible to attrition. Radiographically, obliteration of the pulp chamber of milk teeth is present. Permanent teeth have the right color and root length and obliterated pulp chamber in the shape of thistle with dentinoma in it.
In fibrous dysplasia lesions are present only in primary dentition, teeth have the right color and shape. Radiographically, there are radiolucent and radiopaque areas visible in the pulp chamber and in the canals. Histologically, the condition is far from perfect but neither the shortening of the roots nor the obliteration of the chambers in the shape of the crescent can be observed (4).
All the above mentioned characteristics of the dysplastic dentition lead to tooth loss when the patient is in his 30s, 40s. Clinically, tooth decay is manifested as foci of carious lesions penetrating the obliterated chamber. Additionally there is tooth mobility of degree I or II, especially of incisors due to short roots which hold the teeth in the alveolar bone, as well as periradicular pathology even without clinical signs of caries. The treatment of patients with diagnosed dentin dysplasia requires multidisciplinary approach.
CASE REPORT
A 21-year old female was referred by her family dentist to the Maxillo-Facial Surgery clinic in Warsaw with suspected cysts in the region of teeth 14, 15, 16. Medical history revealed that the patient had no health complaints.
Clinical examination revealed the following findings:
– Extra-orally: symmetrical face, no visible abnormalities of the maxilla and mandible. Exits of trigeminal nerve not tender. Submandibular and submental lymph nodes not enlarged.
Intra-orally: the mucous membrane of the vestibule, the buccae, the floor of the mouth, the tongue, the palate with no pathology.
An OPG of the patient was taken (Fig. 1). Carious lesions of teeth 15, 37 were noted, tooth 26 was missing (the patient reported that it had been extracted due to lack of conservative treatment). Tooth 28 fully erupted while teeth 18, 38, 48 not visible in the mouth. Second degree mobility of central and lateral incisors of the mandible was noted. The patient was also consulted orthodontically.
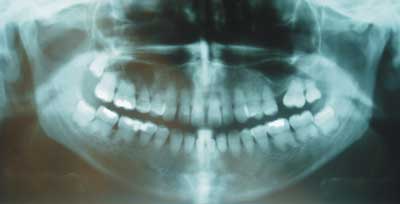
Figure 1. The OPG.
Basing on the interview, the clinical and radiographic examination as well as consultations with orthodontists the following was concluded.
The OPG (taken in November, 2004) displayed:
– periapical lesions of teeth 15, 16,
– deep caries penetrating the remnant of the pulp chamber in tooth 15,
– almost complete obliteration of pulp chambers in all teeth,
– lack of outlines of root canals in all teeth,
– shortening and deformity of all roots,
– reduction of periodontium in all teeth,
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
24 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
59 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
119 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 28 zł
Piśmiennictwo
1. Witkop C.J. Jr.: Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: problems in classification. J. Oral Pathol., 1989, 17, 6, 547-553. 2.Carroll M.K., Duncan W.K.: Dentin dysplasia type I. Radiologic and genetic perspectives in a six-generation family. : Oral Surg Oral Med Oral Pathol. 1994 Sep; 78(3) :375-81. 3.Winter G.B.: Anomalies of tooth formation and eruption. (w:) Pediatric Dentistry (red.) WelburyR.R. OxFord University Press, 1999, 271-273. 4. Carroll M.K.O., et al.: Dentin dysplasia: reviev of literature and a proposed subclassification based on radiographic findings. Oral. Surg. Oral. Med. Oral. Pathol., 1991, 72, 1,119-125. 5.Kaczmarek U., Fita K.: Dysplazja zębiny. Magazyn Stomat., 2004, XIV, 5, 57-61. 6.Shields E.D., et al.: A proposed classification for heritable human dentine defects with a description of new entity. Arch Oral Biol., 1983, 18, 6, 5543-553. 7.Hulisz-Seconska M., et al.: Dysplazja zębiny typ I. Opis przypadku. Czas. Stomat. 1999, LII, 1. 8.Kaczmarczyk-Stachowska A., i wsp.: Rzadki przypadek dysplazji zębiny typu I. Czas. Stomat. 2002, LV, 3. 9.Politowska J., Okoń A.: Dysplazja zębiny. Opis przypadku. Stomat. Współcz., 2005, 1: 30-32. 10.Coke J.M., et al.: Dentinal dysplasia, Type I. Report of a case with endodontic therapy. Oral. Surg. Oral. Med. Oral. Pathol., 1979 Sep; 48(3): 262-8. 11.Seow W.K., Shusterman S.: Spectrum of dentin dysplasia in a family: case report and literature review. Pediatr. Dent., 1994 Nov-Dec; 16(6) :437-42. 12.Kalk W.W., et al.: Dentin dysplasia type I: five cases within one family. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod., 1998 Aug; 86(2) :175-8. 13.Petrone J.A, Noble E.R.: Dentin dysplasia type I: a clinical report. J. Am. Dent. Assoc., 1981 Dec; 103(6) :891-3.
