Jolanta Jadczyszyn, Karolina Raczkowska-Łabuda, *Lidia Zawadzka-Głos
Congenital cholesteatoma of the middle ear in children: a hidden pathology
Perlak wrodzony ucha środkowego u dzieci ? utajona zmiana chorobowa
Department of Paediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Lidia Zawadzka-Głos, MD, PhD
Streszczenie
Wstęp. Perlak wrodzony jest rzadko występującą zmianą ucha środkowego u dzieci. Aby zakwalifikować zmianę chorobową jako perlaka wrodzonego muszą być spełnione odpowiednie kryteria kliniczne.
Cel pracy. Przedstawienie pacjentów z perlakiem wrodzonym hospitalizowanych w Klinice Otolaryngologii Dziecięcej WUM w latach 2018-2019, u których zmiana została wykryta przypadkowo w badaniu pediatrycznym i laryngologicznym, przebiegała skrycie za niezmienioną błoną bębenkową, nie dając żadnych objawów klinicznych.
Materiał i metody. U pacjentów przeprowadzono dokładny wywiad laryngologiczny, badanie mikrootoskopowe i badanie słuchu. W wykonanym przedoperacyjnym badaniu tomografii komputerowej kości skroniowej dokonano analizy rozległości zmian w obrębie ucha środkowego. U wszystkich pacjentów wykonano jednoetapowy zabieg operacyjny z usunięciem zmian z ucha środkowego, a następnie oceniono wynik słuchowy i rezultaty po przeprowadzonej operacji.
Wyniki. U dwóch pacjentów śródoperacyjnie stwierdzono masy perlaka w przednio-górnej części jamy bębenkowej i okolicy trąbki Eustachiusza, u jednego pacjenta perlak wypełniał całe mezotympanum. U pacjentów nie stwierdzono zmian zapalnych w obrębie komórek i jamy wyrostka sutkowego. W dotychczasowej obserwacji nie stwierdzono wznowy perlaka.
Wnioski. 1. Perlaki wrodzone u dzieci są najczęściej wykrywane przypadkowo i zlokalizowane w przednio-górnym kwadrancie jamy bębenkowej. 2. Perlak wrodzony jest zmianą wolno rosnącą i rozwija się za niezmienioną błoną bębenkową. 3. Rozpoznanie opiera się o badanie mikrootoskopii. 4. Jedyną metodą leczenia jest operacyjne usunięcie zmiany.
Summary
Introduction. Congenital cholesteatoma is a rare middle ear pathology in children. An abnormality can be classified as congenital cholesteatoma if it meets certain clinical criteria.
Aim. To present patients with congenital cholesteatoma hospitalised at the Department of Paediatric Otolaryngology of the Medical University of Warsaw in 2018-2019 in whom the abnormality was detected incidentally during paediatric and ENT examination. The disease was hidden behind an intact tympanic membrane with no clinical symptoms.
Material and methods. A thorough ENT history was taken and microotoscopy and a hearing test were conducted. Preoperative computed tomography of the temporal bone was performed to assess the extent of the pathology in the middle ear. A single-stage surgical procedure was performed in all the patients to remove the pathological growths from the middle ear. Subsequently the patients’ hearing and surgical outcomes were evaluated.
Results. During surgery, in two patients cholesteatoma masses were found in the anterosuperior part of the tympanic cavity and in the Eustachian tube area; in one patient, the growth filled the whole mesotympanum. No inflammatory lesions were found in the mastoid cells and antrum. No cholesteatoma recurrence has been found found in follow-up to date.
Conclusions. 1. Congenital cholesteatoma in children is most often detected accidentally and localized in the antero-upper quadrant of the tympanic cavity. 2. Congenital cholesteatoma is a slow-growing lesion and develops behind the unchanged eardrum.3. Diagnosis is based on microotoscopy. 4. The only method of treatment is surgical removal of the lesion.
Introduction
A cholesteatoma, also known as pearly tumour, is a tissue mass composed of matrix, i.e. deposits of keratinised epithelium, keratin, cholesterol crystals and a capsule built of keratinising stratified squamous epithelium. The mass develops at an abnormal anatomical location in the middle ear. Otitis media with cholesteatoma in children can involve acquired cholesteatoma or, much less frequently, congenital cholesteatoma. Congenital cholesteatoma accounts for approximately 2-28% of all cholesteatomas in children (1-3). Congenital cholesteatoma was first described by House in 1953 (4). In 1965, Derlacki and Clemis proposed clinical criteria for this pathology (5). These initial diagnostic criteria were modified by Levenson et al. (6) who regarded a one-time history of otitis media as not excluding congenital cholesteatoma (tab. 1).
Tab. 1. Clinical criteria for the diagnosis of congenital cholesteatoma
| | Clinical criteria for congenital cholesteatoma |
| 1 | A whitish abnormality in the tympanic cavity visible through the tympanic membrane |
| 2 | Normal appearance of the pars flaccida and pars tensa of the tympanic membrane |
| 3 | No ear discharge, no tympanic perforation, no ear trauma |
| 4 | Negative history of ear surgery |
| 5 | A history of uncomplicated acute otitis media does not warrant the exclusion of congenital cholesteatoma |
Potsic distinguished between 4 stages of congenital middle ear cholesteatoma (7):
I: cholesteatoma confined to the anterosuperior quadrant of the tympanic membrane,
II: cholesteatoma of the mesotympanum and a few quadrants of the tympanic membrane without ossicular involvement,
III: cholesteatoma of the mesotympanum and a few quadrants of the tympanic membrane with ossicular involvement but with no mastoid involvement,
IV: mastoid involvement.
Aim
The aim of the study is to characterize and present a rare disease in children that runs secretly behind a properly preserved eardrum, initially gives no clinical symptoms and is most often detected accidentally in a paediatric and ENT examination.
Material and methods
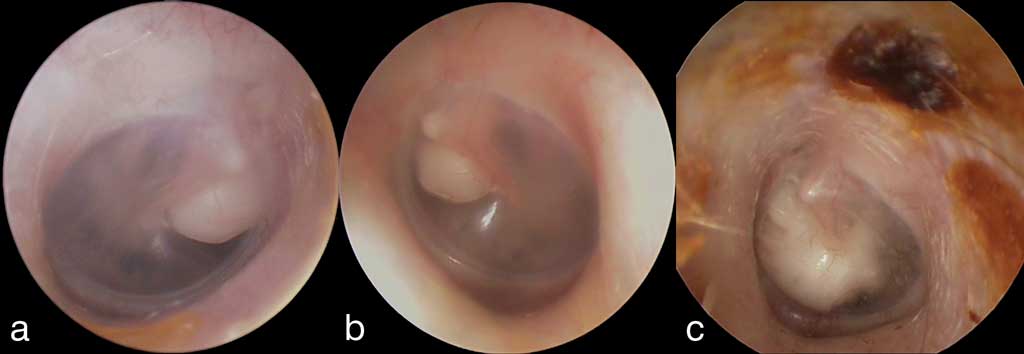
In 2018-2019, three boys with congenital cholesteatoma of the middle ear were hospitalised at the Department of Otolaryngology of the Medical University of Warsaw. Two patients (1 and 2) were referred to the hospital by a paediatrician with suspected foreign body in the ear, while another patient (3) was referred by an ENT physician with suspected congenital cholesteatoma. On admission a thorough ENT history was taken: the patients had not had any episodes of otitis media or middle ear trauma and had not had any ear surgery. The patients did not report any ear pain, tinnitus, a sense of fullness in the ear, dizziness or headaches. The patients’ history was negative for chronic diseases. No family history of cholesteatoma was found either. Otoscopy revealed a normal, wide and inflammation-free external auditory canal in all patients; no foreign body was found there. However, a whitish, spherical mass was found in the tympanic cavity behind an intact tympanic membrane (both pars flaccida and pars tensa were normal). The first, 4-year-old boy, developed a cholesteatoma in the anterosuperior part of the tympanic cavity of the right ear near the tympanic end of the Eustachian tube (fig. 1a). The second, 5-year-old boy, developed a cholesteatoma in the tympanic cavity of the left ear also near the tympanic end of the Eustachian tube (fig. 1b). In the third, 7-year-old patient, the abnormality filled the whole mesotympanum and part of the epitympanic recess (fig. 1c, tab. 2).

Fig. 1a-c. Microotoscopy upon admission to hospital. Congenital cholesteatoma visible behind a normal tympanic membrane, a) right ear (patient 1), b) left ear (patient 2), c) left ear (patient 3)
Tab. 2. Characteristics of patients with congenital cholesteatoma of the middle ear
| No. | Sex | Age (years) | Congenital cholesteatoma of the middle ear |
| 1 | Boy | 4 | Right |
| 2 | Boy | 5 | Left |
| 3 | Boy | 7 | Left |
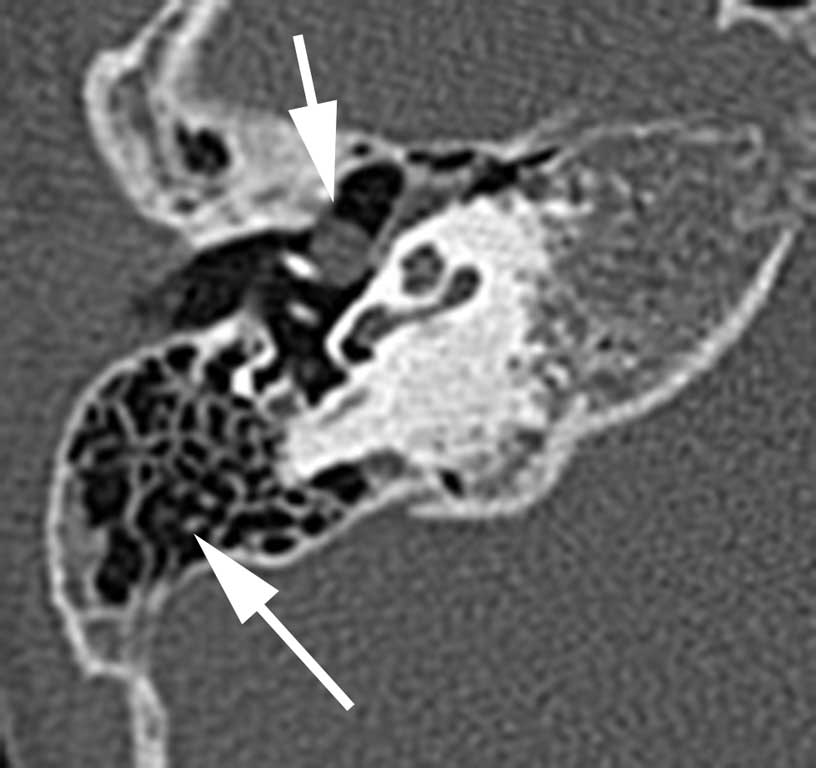
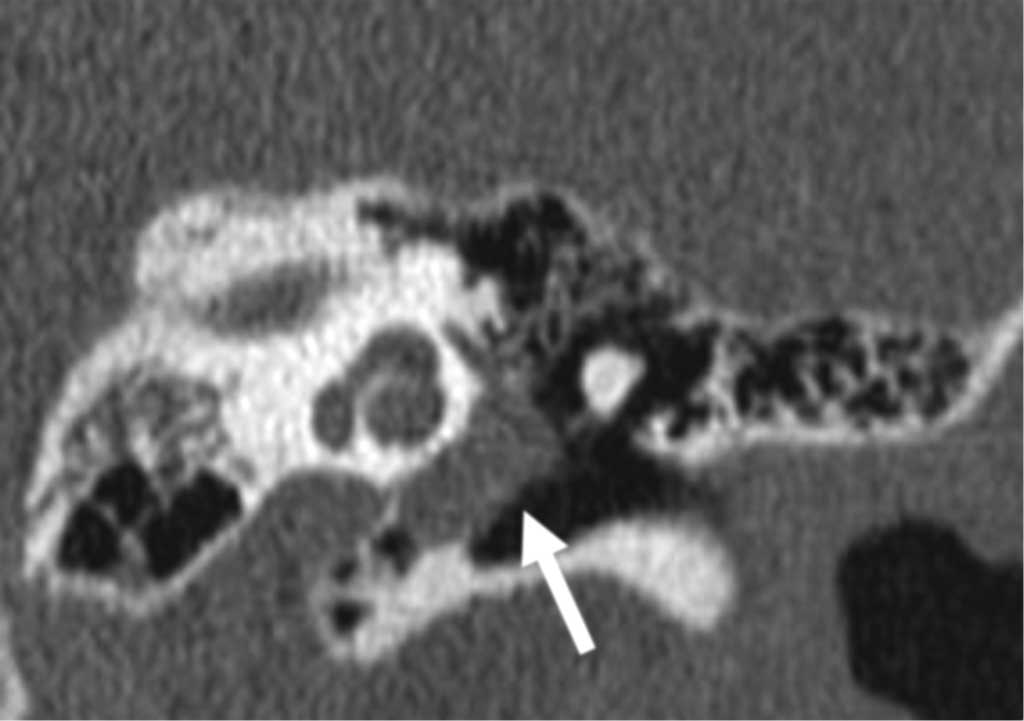
Laboratory test results were normal and inflammatory markers were negative. Whisper and tuning fork hearing tests were performed. Impedance audiometry and pure tone audiometry were also conducted. Before the planned surgery, computed tomography of the temporal bone was also performed in order to assess the pathology in the middle ear. In the first patient, a round soft tissue mass with a diameter of 3.5 mm was present in the medial part of the right tympanic cavity anterior from the manubrium of malleus; the tympanic cavity was inflammation-free and mastoid cells were normally pneumatised (fig. 2a, b).

Fig. 2a. A soft tissue mass in the tympanic cavity of the right middle ear located medially from the ossicles (thick arrow). Normally pneumatised mastoid cells (fine arrow), patient 1

Fig. 2b. Congenital cholesteatoma of the right middle ear (thick arrow): coronal view, patient 1
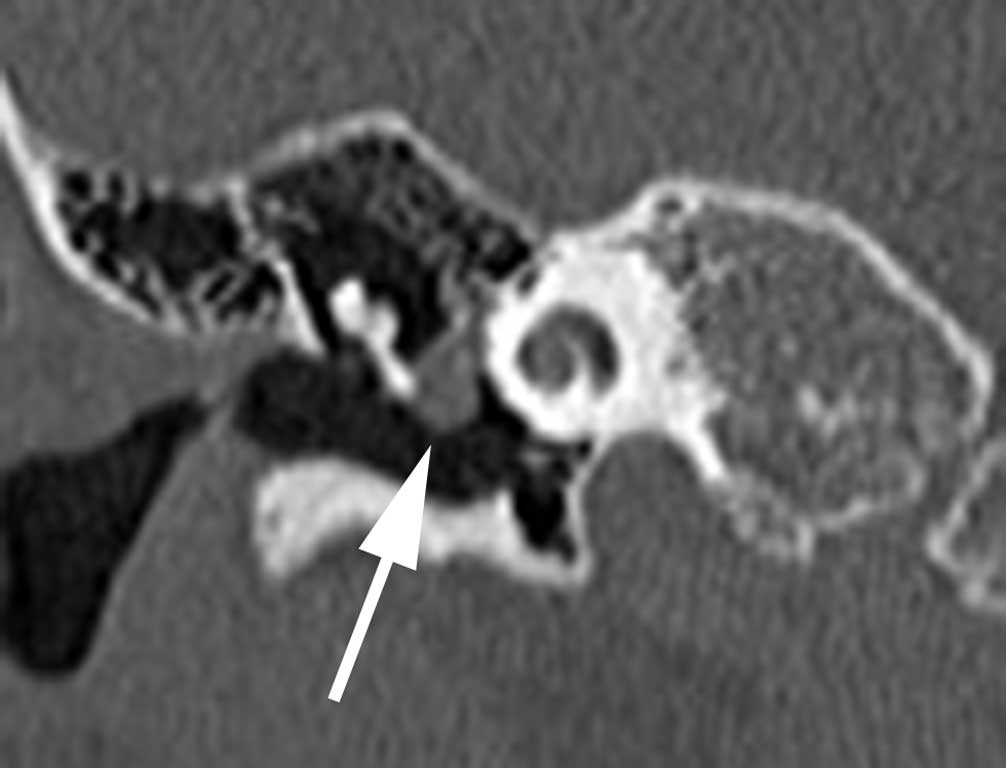
In the second patient, a well-defined, round mass 4 mm in diameter was found directly at the manubrium of malleus in the left tympanic cavity, the epitympanic recess was clear and the ossicular chain was normal (fig. 3a, b).

Fig. 3a. Cholesteatoma “pearl” in the left middle ear (thick arrow). Epitympanic recess with no inflammatory lesions, patient 2

Fig. 3b. Cholesteatoma “pearl” (marked with a thick arrow) in the left tympanic cavity. Bilaterally intact ossicular chain, patient 2
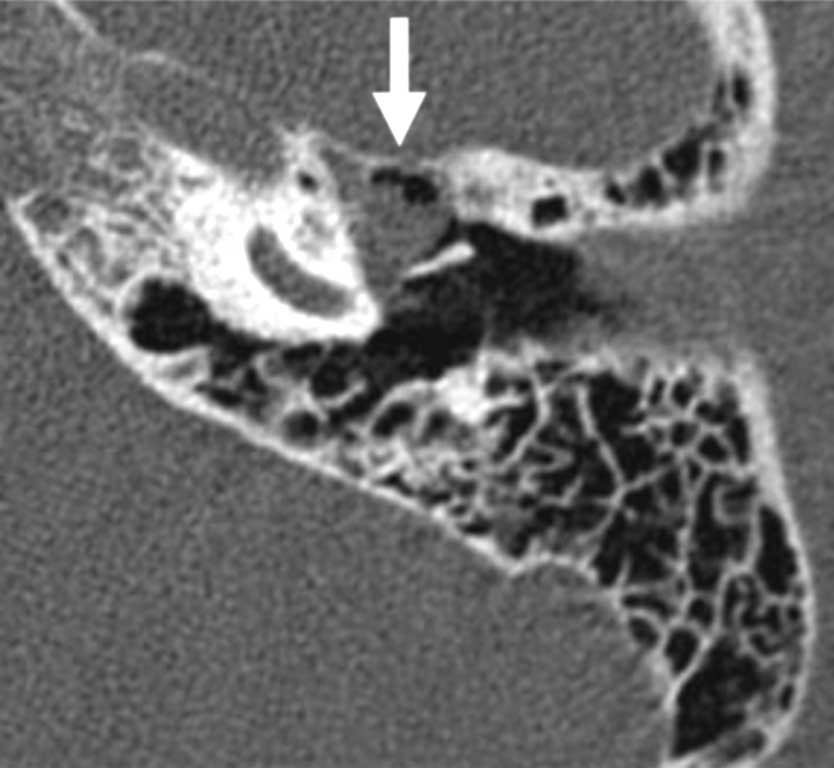
In the third patient, a soft tissue mass was revealed in the left tympanic cavity, which was 7.5 x 8 mm in diameter; the abnormality was present in the mesotympanum and was directed towards the hypotympanum and epitympanic recess; the mass was adjacent to the ossicles but did not cause them to become disconnected (fig. 4a, b). All diagnostic imaging procedures revealed normally pneumatised middle ear cells and mastoid antrum without lesions typical for chronic otitis media. The patients were assessed and scheduled for surgery.

Fig. 4a. Congenital cholesteatoma covering the medial part of the tympanic cavity, the tympanic end of the Eustachian tube and the epitympanic recess, patient 3

Fig. 4b. Congenital cholesteatoma covering the mesotympanum and developing towards the hypotympanum, patient 3
Results
In the hospitalised patients congenital cholesteatoma limited to the tympanic cavity of the middle ear was diagnosed. The mean age of the patients was 5 years and the mean hospitalisation time was 6 days. Microotoscopy revealed a normal, intact, translucent tympanic membrane which had no perforation, signs of thickening or inflammatory lesions of the myringosclerosis type. All congenital cholesteatomas adhered tightly to the tympanic membrane. Normal sound reception was observed on whisper and tuning fork hearing tests in a quiet room with no external noise. Impedance audiometry produced type A tympanometric curves (fig. 5a, b).

Fig. 5a. Impedance audiometry, preoperative assessment, patient 2

Fig. 5b. Impedance audiometry, preoperative assessment, patient 3
The stapedius reflex was present symmetrically in both ears. Pure tone audiometry showed a normal hearing threshold for air and bone conduction in both ears (fig. 6).

Fig. 6. Pure tone audiometry: preoperative hearing test
Computed tomography revealed the presence of abnormalities in tympanic cavities with an intact tympanic membrane. The cholesteatoma was a well-defined tissue mass located medially from the ossicles; it did not cause them to erode. An additional computed tomography scan was performed to make a thorough anatomical analysis of the temporal bone, evaluate the extent of pathology and select the right surgical technique. A single-stage surgical procedure was performed in all the patients during which the masses were removed from the middle ear. In two patients the cholesteatoma “pearls” were removed through an intra-aural approach. These cholesteatomas were well-separated from the surrounding area, had a capsule and adhered to the manubrium of the malleus without causing bone erosion (fig. 7).

Fig. 7. Cholesteatoma “pearl” removed intraoperatively, patient 2
The location of the cholesteatoma “pearls” was confirmed intraoperatively. In the patient in whom the cholesteatoma filled the mesotympanum and partially filled the epitympanic recess and the hypotympanum, left closed tympanoplasty with posterior epitympanotomy was performed. The cholesteatoma did not cover the posterior part of the tympanic cavity and did not reach the antrum; it did adhere to the ossicles, but did not cause them to erode. The ossicular chain was inspected intraoperatively: it had a normal mobility and no adhesions or inflammatory lesions were found in the middle ear. Tympanoplasty was performed during the same surgical session. Histopathological examination confirmed the diagnosis of cholesteatoma. Postoperative hearing results remained good and a tympanic transplant healed well (fig. 8); at present, a year-long follow-up has not revealed any cholesteatoma recurrence.

Fig. 8. Microotoscopy. Status post surgical removal of congenital cholesteatoma with tympanoplasty, patient 1
Discussion
At the Department of Paediatric Otolaryngology of the Medical University of Warsaw, Potsic stage I and II congenital cholesteatoma limited to the tympanic cavity was found in the hospitalised patients. It should be noted that the patients had been referred to the department by a paediatrician with an incorrect diagnosis of foreign body in the ear. Congenital cholesteatoma in children is a hidden disease. There are a few theories accounting for the development of congenital cholesteatoma, which starts to develop already in the embryo and has not underwent involution. Paparella and Rybak explain that this epidermal growth arises from germinal ectoderm from the first and second pair of pharyngeal arches left after foetal development (8). Sade presents a metaplastic theory whereby the mucous membrane of the tympanic cavity undergoes metaplasia to keratinising stratified squamous epithelium (9). Aimi suggests that keratinising stratified squamous epithelium migrates from the external auditory canal skin and grows into the tympanic cavity when the inhibitory function of the tympanic ring fails (10). Piza et al. presents a theory whereby the cells of stratified squamous epithelium are transplanted to the middle ear during amniotic fluid aspiration by the foetus (11). Michaels believes that the epithelium may be formed due to the presence of residual dormant non-keratinising epithelial cells which are distributed in the lateral wall of the Eustachian tube near the tympanic ring and can become keratinised at approximately month 10 of foetal development and disappear at approximately week 33 of gestation (12). However, none of these theories have been proven conclusively and the precise aetiology is still a subject of debate. In the available literature congenital cholesteatomas are usually located in the anterosuperior quadrant of the tympanic membrane (13, 14). Initially, cholesteatomas develop in a slow and limited fashion in the tympanic cavity and as such they do not cause any pain or inflammation in the middle ear and do not cause ossicle erosion and the associated hearing loss, consistent with what was observed in our patients. Cholesteatomas are most often diagnosed incidentally on otoscopic examination as a white pearly mass in the anterosuperior part of the tympanic cavity and near the tympanic end of the Eustachian tube behind an intact tympanic membrane (3, 15). Sometimes congenital cholesteatoma may originate in the posterior part of the mesotympanum from epithelial cells of the area during the development of the temporal bone (16). However, the diagnosis of congenital cholesteatoma is sometimes quite late (3, 17), which is demonstrated by the case of our patients, who were diagnosed as late as at age 5. It needs to be noted that congenital cholesteatoma may be observed for the first time on examination during an acute otitis media episode in children (13). One of the first symptoms of congenital cholesteatoma may be hearing loss associated with otitis media with effusion, when the mass grows anteriorly towards the Eustachian tube causing its obstruction. Subsequently, negative pressure in the tympanic cavity causes the tympanic membrane to be pulled in; as a result, cholesteatoma is visible on otoscopic examination behind an intact tympanic membrane (14, 18). The majority of authors agree that congenital cholesteatoma has a relatively predictable course of slow expansion starting usually from a small “pearl” in the middle ear (13, 14, 19). Cholesteatoma grows down towards the hypotympanum, laterally towards the manubrium of malleus and posteriorly towards the incudostapedial joint, sometimes towards the epitympanic recess causing osteolysis of first the long crus of incus and head of stapes. Once the cholesteatoma grows superiorly towards the epitympanum and anteriorly from the neck and head of malleus where the space is limited, the mass stops growing as a ball and begins to mould to the surrounding spaces penetrating successively the epitympanic recess, retrotympanum and mastoid cells. With time, an expanding cholesteatoma damages the surrounding bone (3, 13, 14). In one of our cases, intraoperative inspection revealed a cholesteatoma growing inferiorly towards the hypotympanum, towards the manubrium of malleus and posteriorly to where it adhered to the incudostapedial joint; however, the mass did not cover the whole joint or the stapedial suprastructure and did not cause the ossicles to erode. However, one needs to bear in mind that the mastoid antrum in small children is built of a few well-pneumatised cells, which is conducive to cholesteatoma spread. However, in older children, mastoid cells are smaller, more sclerotised and less pneumatised, often with a history of inflammation episodes. While congenital cholesteatoma is initially asymptomatic, with time it may lead to hearing loss, tinnitus, otalgia, a sense of fullness in the ear and facial nerve paralysis (5, 8). The clinical presentation of a child with a purulent discharge and tympanic perforation, conduction hearing loss and a cholesteatoma filling the tympanic cavity and mastoid antrum may also be the presentation of the final stage of congenital cholesteatoma development. In our patients, none of the clinical symptoms mentioned above were observed due to the fact that the cholesteatoma was diagnosed at a relatively early stage of development and the diagnosis was based on microotoscopic examination. Speech is an acoustically valuable stimulus for the ear. A whisper speech test is simple, does not require any specialist medical equipment and can be performed by a general practitioner in an outpatient clinic. However, in the diagnosis of middle ear diseases causing conduction hearing loss, impedance audiometry and acoustic resistance measurement are of particular importance. Type A tympanogram is observed in individuals with normal Eustachian tube function, but it may also be present in conduction hearing loss, stapedial ankylosis or the initial stage of otosclerosis (20). However, a type As tympanogram with low middle ear compliance can also occur in healthy ears or in middle ear inflammation manifesting as cholesteatoma, tympanic cavity effusion, polyps, inflammatory granulation tissue or otosclerosis in children (20). Pure tone audiometry is used to determine air and bone conduction hearing threshold (21). However, in children such a test can only be performed from approximately 4 years of age. Computed tomography of temporal bones was performed before the procedure in order to assess the extent of disease found on otoscopic examination, analyse the anatomy of the middle ear and choose the right surgical technique. Hao et al. also considers a diagnostic imaging procedure to be justified before surgery (17, 22). A common location for congenital cholesteatoma of the middle ear is the anterosuperior part of the tympanic cavity near the Eustachian tube and the anterior part of the tympanic ring, medially from the ossicular chain, just below the tensor tympani muscle (13, 14, 19). A middle ear mass in the middle ear should be differentiated from an organised tympanic cavity effusion, cholesterol granuloma, tympanic glomangioma and neurofibroma originating from the tympanic section of the facial nerve (23). Although the abnormalities mentioned above look similar on diagnostic imaging, congenital cholesteatoma does not enhance upon contrast administration and differential microotoscopy remains a very important examination (24, 25). One should bear in mind the fact that the only method of cholesteatoma treatment in children is surgical removal of the tumour. Topical and systemic antibiotic therapy is ineffective. In congenital cholesteatomas limited to the tympanic cavity intra-aural approach was used, which provided good access to the tympanic cavity and possibility to remove the whole intact cholesteatoma pearl with little risk of residual disease. This access is also recognised by Nelson as appropriate for the early stage of cholesteatoma development and the 0% recurrence rate suggests that stage I cholesteatomas do not require routine second-look surgery (13). When intraoperative inspection revealed that the cholesteatoma started to adhere to the manubrium and neck of malleus, covered the complex topography of supporting ligaments and was spreading to the epitympanic recess, retroauricular access with closed tympanoplasty and posterior epitympanotomy was used. Isaacson confirms that although cholesteatoma is a histologically benign abnormality, it has the ability to spread in the middle ear, causing bone damage. Treatment is exclusively surgical and the success of the operation is largely dependent on the stage of the disease (26). Congenital cholesteatoma is still a diagnostic challenge for primary care doctors and a surgical one for ENT physicians. Incorrect diagnosis is common due to the infrequent occurrence and insidious development of cholesteatoma and the characteristic lack of complaints and lack of otitis media symptoms. Too late a diagnosis leads to the development of complications. It is important that the disease be diagnosed at an early and asymptomatic stage and the patient be referred for a quick diagnostic investigation and surgery so that ossicle erosion and the associated hearing loss can be prevented. Our one-year-long follow-up period is relatively short compared to the one reported by other authors (27). However, to date we have not found any recurrence of congenital cholesteatoma in the tympanic cavity and the patients are still under the care of the hospital outpatient clinic. Early detection of abnormalities in the tympanic cavity of the middle ear is primarily due to the awareness of the possible occurrence of congenital cholesteatoma in children.
Conclusions
1. Early-stage congenital cholesteatoma of the middle ear in children is usually diagnosed incidentally.
2. The most common location is the anterosuperior part of the tympanic cavity.
3. Investigation and diagnosis of congenital cholesteatoma is based on microotoscopy; computed tomo-graphy of the temporal bones is also a useful procedure in the process.
4. The only method of cholesteatoma treatment is surgical removal of the mass.
Piśmiennictwo
1. McDonald TJ, Cody DT, Ryan RE Jr: Congenital cholesteatoma of the ear. Ann Otol Rhinol Laryngol 1984; 93: 637-640.
2. Friedberg J: Congenital cholesteatoma. Laryngoscope 1994;104: 1-24.
3. Potsic WP, Wetmore RF, Marsh RR: Congenital cholesteatoma: fifteen years experience at The Children’s Hospital of Philadelphia. [In:] Sanna M (ed.): Cholesteatoma and Mastoid Surgery. CIC Edizioni Internazionali, Rome 1997: 422-431.
4. House HP: An apparent primary cholesteatoma, case report. Laryngoscope 1953; 63: 712-713.
5. Derlacki EL, Clemis JD: Congenital cholesteatoma of the middle ear and mastoid. Ann Otol Rhinol Laryngol 1965; 74: 706-727.
6. Levenson MJ, Micheals L, Parisier SC: Congenital cholesteatomas of the middle ear in children: origin and management. Otolaryngol Clin North Am 1989; 22: 941-954.
7. Potsic WP, Samadi DS, Marsh RR, Wetmore RF: A Staging System for Congenital Cholesteatoma. Arch Otolaryngol Head Neck Surg 2002; 128(9): 1009-1012.
8. Paparella MM, Rybak L: Congenital Cholesteatoma. Otolaryngol Clin North Am 1978; 11: 113-120.
9. Sade J: The etiology of cholesteatoma: the metaplastic theory. [In:] McCabe B, Sade J, Abrahamson M (eds.): Cholesteatoma: First International Conference. Aesculapius Publishing, Birmingham 1977: 212-232.
10. Aimi K: Role of the tympanic ring in the pathogenesis of congenital cholesteatoma. Laryngoscope 1983; 93: 1140-1146.
11. Piza J, Gonzales M, Northorp CC: Meconium contamination of the neonatal ear. J Pediatr 1989; 115: 910-914.
12. Michaels L: An epidermoid formation in the developing middle ear: possible source of cholesteatoma. J Otolaryngol 1986; 15: 169-174.
13. Nelson M, Roger G, Koltai PJ et al.: Congenital cholesteatoma classification, management and outcome. Arch Otolaryngol Head Neck Surg 2002; 128: 810-814.
14. Koltai PJ, Nelson M, Castellon RJ et al.: The natural history of congenital cholesteatoma. Arch Otolaryngol Head Neck Surg 2002; 128: 804-809.
15. Tos M: A New Pathogenesis of Mesotympanic Congenital Cholesteatoma. Laryngoscope 2000; 110: 1890-1897.
16. Karmarkar S, Bhatia S, Khashaba A et al.: Congenital cholesteatomas of the middle ear: a different experience. Am J Otol 1996; 17(2): 288-292.
17. Hao JS, Chen M, Liu B, Yang Y, Liu W, Zhang J. Clinical treatment of congenital middle ear cholesteatoma in children. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2018 Jul;32(14):1097-1101.
18. House JW, Sheehy JL. Cholesteatoma with intact tympanic membrane: a report of 41 cases. Laryngoscope 1980;90(1);70-76.
19. Park KH, park SN, Chang KH, Jung MK, Yeo SW. Congenital middle ear cholesteatoma in children; restrospective review of 35 cases. J Korean Med Sci 2009;24;126-131.
20. Namysłowski G., Fira R: Audiometria impedancyjna. In Śliwińska-Kowalska M, editors Audiologia Kliniczna. 1. Łódź: Mediton Oficyna Wydawnicza, 2005. 137-148.
21. Pruszewicz A., Świdziński P: Metody psychofizyczne badania narządu słuchu. In Pruszewicz A., Obrębowski A., editors Audiologia Kliniczna zarys. Wydawnictwo Naukowe Uniwersytetu Medycznego im. Karola Marcinkowskiego w Poznaniu,2010. 182-192.
22. Manolis EN, Filippou DK, Tsoumakas C et al.: Radiologic evaluation of the ear anatomy in pediatric cholesteatoma. J Craniofac Surg 2009; 20(3): 807-810.
23. Phelps PD, Wright A: Imaging cholesteatoma. Clin Radiol 1990; 41(3): 156-162.
24. Reddy CE, Goodyear P, Ghosh S, Lesser T: Intratympanic membrane cholesteatoma: a rare incidental finding. Eur Arch Otorhinolaryngol 2006; 263: 1061-1064.
25. Pasanisi E, Bacciu A, Vincenti V, Bacciu S: Congenital cholesteatoma of the tympanic membrane. Int J Pediatr Otorhinolaryngol 2001; 61: 167-171.
26. Isaacson G: Diagnosis of pediatric cholesteatoma. Pediatrics 2007; 120(3): 603-608.
27. McGill TJ, Merchant S, Healy GB, Friedman EM: Congenital cholesteatoma of the middle ear in children: a clinical and histopatological report. Laryngoscope 1991; 101(6): 606-613.