© Borgis - New Medicine 3/2010, s. 94-98
*Erzsébet Pálfi, Zoltánné Horváth, Márta Veresné Bálint, Istvánné Németh, Mária Barna
Dietary management of food allergy – different channels of education of patients in hungary
Semmelweis University Faculty of Health Science
Dean: Dr. Judit Meszaros, Phd
Department of Dietetics and Nutrition Science, Budapest, Hungary
Head of Department: Prof. Dr. István Szabolcs
Head: Dr. Mária Barna
Summary
Introduction. The prevalence of food allergy is approximately 1-2% in adults and 5-8% in children less than 3 years of age. The allergen avoidance diet is the key treatment of food allergy and it is feasible only with information about food allergen content. In Hungary there are different techniques of conveying information for sensitive consumers.
Aim. The authors aimed to find the most practicable ways of conveying information in food allergy management.
Material and Method. We measured the Hungarian situation with a computer background multi-criteria interview method that took 1.5 ± 0.50 hours. The interview contained 20 pre-defined options that showed the complex situation of food allergy management in Hungary and some viewpoints of their evaluation. We compared the opinions based on criteria developing a comprehensive opinion spectrum. The 30 interviewees were involved from patient organisations, the health care and scientific sector, food companies, the food commerce and public catering area, consumer protection, the media, and the food safety and policy sector.
Results. Allergen information as patients' information on the food labelling is not sufficient and they do not replace dietitian counselling and further patient management by a dietitian. Education of patients was a priority in food allergy management. The Databank is a parallel way for consumers suffering from food allergy to obtain information about "free from” products that supplements the food labelling legislation.
Conclusions. Both the health system and food safety include channels of allergen information from product to patient.
INTRODUCTION
The incidence of self-reported food allergies is between 3 and 35% (1). Diagnosed food allergies affect approximately 1-2% of adults and 5-8% of children in Europe. Egg and milk allergies are the most common in childhood. Allergies to fruits and vegetables are more common in adulthood and peanut allergy is common among children as well as adults. Furthermore, the prevalence of food allergy changes with age (2). There has been a recent increase in the prevalence of atopic reactions (3). Food allergy is an adverse immune reaction to food proteins and its key treatment is the allergen avoidance diet that is based on the correct diagnosis (4, 5). A safe and adequate allergen-free diet is difficult, because the information on allergen content might be unclear (6). Patients suffering from milk allergy might not recognize that casein is an ingredient of cow's milk (7). Additionally, the allergen cross-contamination in industries is unlabelled in much commercial food, e.g. unpackaged or catering food (8). The avoidance diet has an effect on the quality of life of food allergic patients and their family (9). The effects of food allergy are not only limited to individuals suffering allergy. Food allergy management is part of food safety and food legislation. The European Union regulates allergen labelling in the Directive of 2000/13/EC (2003/89/EC modification), which makes labelling major allergens compulsory (10, 11). The current labelling regulations are not sufficient for patients suffering from food allergy, so we have to provide the information about "free from” products in other ways.
AIM
The aim of this research was to find the best intervention strategies in the management of food allergy. The authors compared the viewpoints of key stakeholders, in this manner developing a comprehensive and multidisciplinary opinion spectrum.
MATERIAL AND METHOD
A computer-based personal interview method was used for the investigation to provide a comparative analysis of the differing perspectives of stakeholders (12). Thirty interviewees were involved in the current research from the following areas: Hungarian patients' organizations, scientific and health care area, the market sector (food industries, commerce, catering), the consumer protection sector, policy makers and the publicity sector. The interview took 1.5 ± 0.50 hours. The interview subjects showed the complex situation of food allergy management in Hungary and they are selected from the following issues: food regulations, food safety and consumer protection, "free from” food trade, public catering, education of patients and staff of health system, protocol of food allergy diagnosis and treatment. In this paper some of the judgements about food allergen information channels are highlighted.
The computer-based, multi-criteria interview contains 20 pre-defined options and some viewpoints (criteria) of their evaluation. The criteria were the feasibility of interventions, the cost-benefit ratio and the group of food allergic patients concerned. The interviewees ranked the options with a score system (score from 1 to 10), so they developed a score interval. The stakeholders made written commentaries that completed the score system (12). Data were analysed by using variance analysis to determine the changes for all comparisons; a P value of 0.05 was considered significant.
RESULTS
The importance of three criteria was considered identical in each single perspective. All three criteria are important to develop a complex opinion spectrum (fig. 1). The allergen avoidance diet is the treatment of food allergy that will only be achieved with the relevant allergen information. Figure 2 shows the comparison of options of information channels. There are no significant differences between options about food allergen information, education of patients and the Databank (p=0.05), so the options are ranked according to the order of importance (fig. 2). Figure 3 gives an overview about the necessity of options in the issue of allergen information on the grounds of rank of opinion scores and written commentaries of stakeholders (fig. 3).
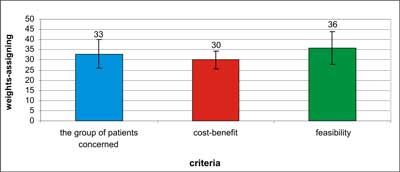
Fig. 1. The importance of criteria (feasibility, cost-benefit ratio and the group of patients concerned) based on the opinion of different stakeholders (n=30; p=0.05).
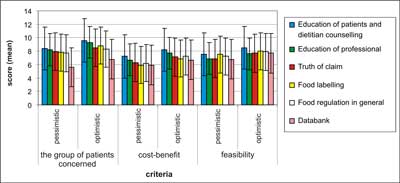
Fig. 2. Comparison of options of education techniques (p=0.05). The stakeholders developed a pessimistic (negative) and an optimistic (positive) score (score of 1-10) based on each viewpoint.
Fig. 3. Rank means given by different stakeholder groups' range for options of allergen information. A score interval from pessimistic (score 1) to optimistic (score 10) opinion was developed. Stakeholder groups: A – patient organisations; B – health care and scientific sector; C – market sector; D – consumer protection; E – policy makers; F – publicity.
Education of patients was a priority in food allergy management in this gradation by stakeholders of the consumer organisation, policy makers, the scientific-health care sector and the market sector. The mean pessimistic and optimistic score (negative score-positive score ± SD) of the patient education option was 7.3-8.8 ± 2.49 in the market sector, 8.6-9.1 ± 2.67 in the policy maker group, 7.9-8.7 ± 2.16 in the scientific and health care sector and 9.6 ± 0.52 in the consumer organisation. In the view of patient organisations, the education of patients was just sixth (mean score was 6.5-8.2 ± 2.64) and the publicity sector placed it in second position (7.6-8.5 ± 2.43). Education of professionals was the second most relevant option in policy makers (8.2-8.6 ± 2.92) and the scientific-health care sector (7.7-8.7 ± 2.24); it was third in patient organisations (9.0 ± 1.59). However, the consumer protection organisation found the education of professionals option the least relevant point of all (6.0 ± 1.78). In the opinion of patients, the necessity of understanding scored 9.5 ± 0.79. Although allergen information as patients' information on the labelling is not sufficient and does not replace dietitian counselling and patient management by a dietitian, full and reliable labelling is very important. Adequate allergen labelling as an intervention point was also preferred by the publicity sector (8.5-9.5 ± 1.54), policy makers (7.6-7.8 ± 2.68), the consumer protection specialists (9.3-9.3 ± 1.03) and the patient organisations' representatives (8.2-9.2 ± 1.77). The third channel is the Hungarian Food Allergy and Food Intolerance Databank. The stakeholders of the scientific/health care and policy maker sectors gave the food allergy databank scores of 5.9-7.0 ± 2.83 and 6.6-7.7 ± 2.96 respectively. Table 1 shows the rank of options based on the opinion of stakeholders from different areas (tab. 1).
Table 1. Rank of necessity of options in food allergy management.
| Rank | Mean ? SD | Options |
| 1. | 8.26 ? 2.38 | Education of patients |
| 2. | 7.75 ? 2.61 | Education of professionals |
| 3. | 7.49 ? 2.76 | Food labelling |
| 4. | 7.43 ? 2.70 | Role of commercial sector |
| 5. | 7.4 ? 2.83 | Truth of food claim |
| 6. | 7.38 ? 2.74 | Food law in general |
| 7. | 7.36 ? 3.26 | Therapy protocol use |
| 8. | 6.8 ? 3.48 | Prevention |
| 9. | 6.71 ? 3.20 | Dietitian counselling |
| 10. | 6.59 ? 2.94 | Food Allergy Databank |
| 11. | 6.3 ? 3.49 | Food allergy diagnosis |
| 12. | 6.24 ? 3.08 | Research |
| 13. | 6 ? 3.12 | Assortment of product |
| 14. | 5.8 ? 3.51 | Therapy of food allergy |
| 15. | 5.58 ? 3.44 | Subsidy of family affected by food allergy |
| 16. | 5.54 ? 3.12 | Control of labelling |
| 17. | 5.2 ? 3.39 | Social impact of food allergy |
| 18. | 5 ? 3.72 | Subsidy of health system |
| 19. | 4.49 ? 3.15 | Cost of diet |
| 20. | 4.2 ? 3.10 | Subsidy of industries and commerce |
DISCUSSION
Overall, the options formed a picture about which information channels may be effective for food allergy treatment and management. The allergen information affects the quality of life of food allergic patients (13). In our research we found both education of patients and relevant, reliable allergen labelling to be the primarily workable treatment strategies. The safe avoidance diet is feasible only with sure knowledge of allergen content and understanding of food labelling. In addition, the communication between patients, physician and dietitian plays the most important role in the treatment of food allergy. Food allergic patients are very conscious consumers who take into consideration most seriously legible labelling information. In spite of relevant labelling consumers cannot understand the information (14), and their knowledge is uncertain, so the education of consumers is necessary. Our results showed that the patients suffering food allergy and their health care professionals both demanded readable, understandable and easy-to-use allergen labelling. Cornelisse-Vermaat et al. reported similar results (15).
Furthermore, the Food Allergy Databank is a parallel way to access information about "free from” products and it functions side by side with the labelling regulation in Hungary. The Hungarian Food Allergy and Food Intolerance Databank publishes approximately 5000 booklets/year for patients and it has approximately 12 000 website-downloads/month. Patients suffering from food allergy have access to "free from” product lists and booklets during everyday shopping and they found them readable and useable. The stakeholders found that keeping and developing the Databank was important, although these "free from” booklets were time-consuming and expensive to keep up-to-date. At the same time, the allergen information booklets are easy to understand and easy to use for allergic patients.
Additionally, dietitian counselling as a patient education method was ranked as a good intervention point in treatment of food allergies. The key stakeholders suggested that the education of consumers is the most relevant intervention strategy and that allergy expert training is important, because adequate dietician counselling is not efficient without up-to-date knowledge and the allergen avoidance diet.
CONCLUSION
All of the information channels have considerable importance in food allergy management. The safe allergen avoidance diet includes dietetic counselling and the patients' management that is concentrated in the health system. However, the further follow-up and management take place beyond the health system. The information about allergens and "free from” products are part of food safety as well as dietetics and the health system.
Piśmiennictwo
1. Mills ENC et al.: The prevalence, cost and basis of food allergy across Europe. Allergy 2007; 62: 717-722. 2. Yun J, Katelaris CH: Food allergy in adolescents and adults. Int Med J 2009; 39: 475-478. 3. Chehade M: IgE and non-IgE-mediated food allergy: treatment in 2007. Curr Opin Allergy Clin Immunol 2007; 7: 264-268. 4. Johansson SGO et al.: A revised nomenclature for allergy. Allergy 2001; 56: 813-824. 5. Bindslev-Jensen C et al.: Standardization of food challenges in patients with immediate reactions to foods – position paper from the EAACI. Allergy 2004; 59: 690-697. 6. Pieretti MM et al.: Audit of manufactured products: Use of allergen advisory labels and identification of labeling ambiguities. J Allergy Clin Immunol 2009; 124: 337-41. 7. Buhl T et al.: The European labelling law for foodstuffs contains life-threatening exemptions for food-allergic consumers. Int Arch Allergy Immunol 2008; 146: 334-337. 8. Cornelisse-Vermaat JR et al.: The information needs and labelling preferences of food allergic consumers: the views of stakeholders regarding information scenarios. Food Science & Technology 2008; 19: 669-676. 9. de Blok BMJ et al.: A framework for measuring the social impact of food allergy across Europe: a EuroPrevall state of the art paper. Allergy 2007; 62: 733-737. 10. Directive 2000/13/EC of the European Parliament and of the Council of 20 March 2000 on the approximation of the laws of the Member States relating to the labelling, presentation and advertising of foodstuffs for sale to the ultimate consumer. OJ EC L 109. European Union 2000; 29-42. 11. Directive 2003/89/EC of the European Parliament and of the Council of 10 November 2003 amending directive 2000/13/EC as regards indication of the ingredients present in foodstuffs. Official Journal of the European Union 2003; L308/15. 12. Stirling A, Lobstein T, Millstone E: Methodology for obtaining stakeholder assessments of obesity policy options in the PorGrow project. Obesity Reviews 2007; 8(Suppl. 2): 17-27. 13. Miles S et al.: A framework for measuring costs to society of IgE-mediated food allergy. Allergy 2005; 60(8): 996-1003. 14. Mills ENC et al.: Information provision for allergic consumers – where are we going with food allergen labelling? Allergy 2004; 59: 1262-1268. 15. Cornelisse-Vermaat JR et al.: Food-allergic consumers' labelling preferences: a cross-cultural comparison. Eur J Public Health 2007; 18(2): 115-120.