© Borgis - New Medicine 2/2014, s. 55-56
*Konrad Wroński1, 2
Porcelain gallbladder – case report
1Department of Oncology, Faculty of Medicine, University of Warmia and Mazury, Olsztyn, Poland
Head of Department: prof. Sergiusz Nawrocki, MD, PhD
2Department of Surgical Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department: Andrzej Lachowski, MD
Summary
Porcelain gallbladder is rare manifestation of chronic cholecystitis. Calcification of the gallbladder wall is present between 0.06%-0.8% of cholecystectomy specimens. The pathogenesis is still unknown but it is believed that it caused by irritation the gallbladder by stones which lead to chronic inflammation associated with calcium deposit. Calcification of the gallbladder wall is associated with risk of gallbladder cancer.
The author of this article presented a case of a woman who was admitted to the hospital because of suspicion tumor of gallbladder. The patient underwent open cholecystectomy during which porcelain gallbladder was removed. The author performed a literature review on porcelain gallbladder.
INTRODUCTION
Porcelain gallbladder is rare manifestation of chronic cholecystitis. Calcification of the gallbladder wall is present between 0,06-0,8% of cholecystectomy specimens (1, 2). The pathogenesis is still unknown but it is believed that it caused by irritation the gallbladder by stones which lead to chronic inflammation associated with calcium deposit. Calcification is five times more common in female than in men population (3). Mean age of diagnosed porcelain gallbladder is 54 years (range 38-70 years) (3). Calcification of the gallbladder wall is associated with risk of gallbladder cancer. The carcinogenesis in calcified gallbladder probably follows the metaplasia – dysplasia – carcinoma sequence.
CASE REPORT
A 62-year-old white lady referred to the department due to a suspicion tumor of gallbladder diagnosed in ultrasound examination. The patient has reported pain in the right hypochondrium region. She had no any other symptoms, drug abuse and there was no history of weight loss and loss of appetite. She had two surgeries – first due to uterine myomas and total hysterectomy due to cervical cancer. There was history of carcinoma in patient family – mother suffered from anal canal cancer.
On physical examination, in the right hypochondrium patient reported pain. There were no peritoneal symptoms. Blood tests were normal. There was no histopathological examination of the fine-needle aspiration biopsy before planned surgery.
An ultrasound examination showed thickened gallbladder wall with a diameter of 9 mm with a focus on the nature of the tumor in the wall with a diameter of about 8 mm. Computer tomographic scan (CT scan) revealed calcified gallbladder wall with dense intraductal calcification.
The patient was taken to the operating room for an open cholecystectomy. During the surgical exploration claimed calcification of the gallbladder wall. Porcelain gallbladder was removed (fig. 1-3). The material was sent for routine histopathological examination. The time of surgery was about 45 minutes.
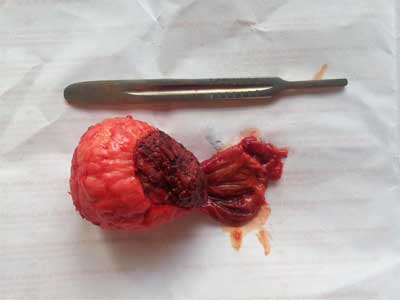
Fig. 1. Porcelain gallbladder after cholecystectomy.

Fig. 2. Calcification of the gallbladder wall – view from the fundus.
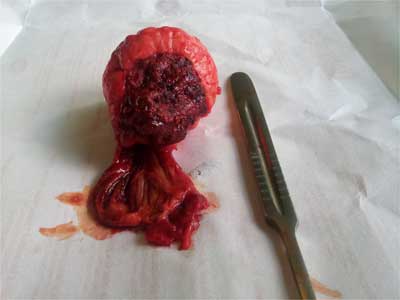
Fig. 3. Porcelain gallbladder – view from the neck.
Histopathology examination showed a porcelain gallbladder without neoplasm component. Patient after surgery felt good and did not complain of pain. The postoperative period was uncomplicated and the patient left the ward in the 5th day after surgery.
DISCUSSION
Porcelain gallbladder is a relatively rare disease. The term „porcelain gallbladder” is used to describe brittle consistency and white-bluish discoloration of the gallbladder wall. The pathogenesis of this disease is still unknown. It is believed that it caused by irritation the gallbladder by stones which lead to chronic inflammation associated with calcium deposit (2). Other theories postulated that obstruction of cystic duct leading to mucosal precipitation of calcium carbonate salts which in turn causes bile to stagnate within gallbladder (1). Cornell and Clarke (3) think that calcification is a dystrophic process resulting from chronic infection and compromised circulation due to influence cystic duct stones which cause hemorrhage, scaring and hyalinization of gallbladder wall. Such process leads to origin a matrix for deposition of lime salt (3).
There are two histological types calcification of the gallbladder wall. First type consists of a continuous broad band within the muscularis, and second type where numerous calcified microliths are scattered diffusely throughout the mucosa and submucosa localized in glandular spaces and in the Rokitansky-Aschoff sinuses (6, 7).
The risk of malignancy inside a porcelain gallbladder was reported, in first publication from 1960s, on the level 10-61% (6-8). Latest publication have shown lower incidence carcinoma cells inside calcified gallbladder between 5-10% (4, 5). Presently stands out two types of calcification. In case of selective mucosal calcification the incidence of cancer is approximately 7% (5). There is no association between carcinoma and complete intramural calcification (5).
Because of the gallbladder cancer risk, prophylactic cholecystectomy is the treatment of choice for porcelain gallbladder (4, 9). Some articles suggest that patients with calcified gallbladder are not good candidates for laparoscopic treatment due to brittle consistency of the gallbladder wall (10, 11). The other articles describe the successful cholecystectomy performed because of porcelain gallbladder (10-13). Some authors suggest that laparoscopic cholecystectomy is suggested in the completed calcification type of porcelain gallbladder than in the complete intramural calcification type (4, 6, 14).
CONCLUSIONS
1. Porcelain gallbladder is a relatively rare disease.
2. Calcification of the gallbladder wall is associated with risk of gallbladder cancer.
3. Prophylactic cholecystectomy is the treatment of choice for porcelain gallbladder.
Piśmiennictwo
1. Polk HC Jr: Carcinoma and the calcified gallbladder. Gastroenterology 1966; 50: 582-585. 2. Ashur H, Siegal B, Oland Y et al.: Calcified gallbladder (porcelain gallbladder). Arch Surg 1978; 113: 594-596. 3. Cornell CM, Clarke R: Vicarious calcification involving the gallbladder. Ann Surg 1959; 149: 267-272. 4. Kwon AH, Inui H, Matsui I et al.: Laparoscopic cholecystectomy in patients with porcelain gallbladder based on preoperative ultrasound findings. Hepatogastroenterology 2004; 51: 950-953. 5. Stephen AE, Berger DL: Cancer in the porcelain gallbladder: a relationship revisited. Surgery 2001; 129: 699-703. 6. Shimizu M, Miura J, Tanaka T et al.: Porcelain gallbladder relation between its type by ultrasound and incidence of cancer. J Clin Gastroenterol 1989; 11: 471-476. 7. Berk RN, Armbuster TG, Salzstein SL: Carcinoma in the porcelain gallbladder. Radiology 1973; 106: 29-31. 8. Opatrny L: Porcelain gallbladder. Can Med Assoc J 2002; 166: 933. 9. Sheth S, Beford A, Chopra S: Primary gallbladder cancer: recognitation of risk factors and the role of prophylactic cholecystectomy. Am J Gastroenterol 2000; 95: 1402-1410. 10. Puia IC, Vlad L, Iancu C et al.: Laparoscopic cholecystectomy for porcelain gallbladder. Chirurgia (Bucur) 2005; 100(2): 187-189. 11. Welch NT, Fitzgibbons RJ Jr, Hinder RA: Beware of the porcelain gallbladder during laparoscopic cholecystectomy. Surg Laparosc Endosc 1991; 1(3): 202-205. 12. Kim JH, Kim WH, Yoo BM et al.: Should we perform surgical management in all patients with suspected porcelain gallbladder? Hepatogastroenterology 2009; 56(93): 943-945. 13. Khan ZS, Livingstone EH, Huerta S: Reassessing the need for prophylactic surgery in patients with porcelain gallbladder. Arch Surg 2011; 146(10): 1143-1147. 14. Kane RA, Jacobs R, Kats J et al.: Porcelain gallbladder: ultrasound and CT appearance. Radiology 1984; 152: 137-141.
