© Borgis - New Medicine 3/2014, s. 86-88
*Konrad Wroński1, 2, Maciej Żechowicz1, 3, Tadeusz Żechowicz3
Preparation of the patient with colorectal carcinoma receiving Omega-3 fatty acids to surgery – case report and review of literature
1Department of Oncology, Faculty of Medicine, University of Warmia and Mazury, Olsztyn, Poland
Head of Department: prof Sergiusz Nawrocki, MD, PhD
2Department of Surgical Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department: Andrzej Lachowski, MD
3Department of Internal Diseases, Gastroenterology, Cardiology and Infectiology Faculty of Medicine, University of Warmia and Mazury in Olsztyn, Poland
Head of Department: prof. Piotr Zaborowski, MD, PhD
Summary
Fish oil rich in omega-3 polyunsaturated fatty acid comes from cold water fish such as tuna, herring, salmon and anchovies. Omega-3 fatty acids plays important role on human health. Their beneficial effects were discovered in cardiovascular diseases, hepatic lipid metabolism, inflammatory diseases, glucose homeostasis and insulin sensitivity. Fish oil rich in omega-3 fatty acids inhibit thrombosis and it is possible that the patients taking fish oil tablets have higher risk for bleeding during surgery (1-4).
The authors of this article presented a case of a men who was admitted to the hospital because of colorectal carcinoma. In the interview, the patient was taking fish oil tablets. In this article, we describe the behavior of the receiving sick fish oil tablets, and reviewed the literature relating to this issue.
INTRODUCTION
Fish oil rich in omega-3 polyunsaturated fatty acid comes from cold water fish such as tuna, herring, salmon and anchovies. Omega-3 fatty acids plays important role on human health. Their beneficial effects were discovered in cardiovascular diseases, hepatic lipid metabolism, inflammatory diseases, glucose homeostasis and insulin sensitivity (1-3). Fish oil rich in omega-3 fatty acids inhibit thrombosis. Because of an antithrombotic effect it is possible that fish oil could potentially increase the risk for bleeding during surgery (1-4).
CASE REPORT
A 65-year-old white man, Caucasian race, referred to the Department of Surgical Oncology Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre in Olsztyn due to diagnosed colorectal carcinoma. In colonoscopy and computed tomography tumor was located in thehepatic flexion. Microscopically, the tumor was adenocarcinoma. The patient has reported no pain in the abdominal area. He had no any other symptoms and there was no history of weight loss and loss of appetite. There was no history of colorectal carcinoma in his family.
In medical history: the patient suffered from hypertension and ischemic heart disease. Therefore was prescribed inter alia the oral administration of fish oil tablets by his cardiologist (fig. 1).
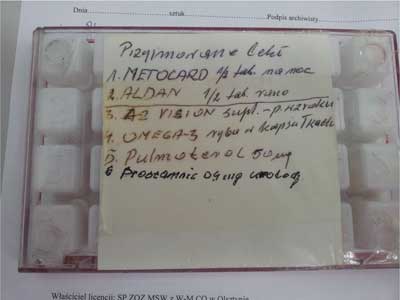
Fig. 1. List of drugs taken by the patient – in fourth position are fish oil tablets.
On physical examination the abdomen was soft, painless, without symptoms of peritoneal. The hemoglobin level was 126 g/l, the red blood cell count was 4.15 x 1012/l and other routine hematological examinations and biochemical tests were within normal limits.
In the absence of symptoms of gastrointestinal obstruction and admission by the patient of fish oil tablets was decided to delay the surgery for 7 days. The patient did not require urgent surgical intervention. The patient was informed about the risks related to certain bleeding in the perioperative period and ordered to set aside the fish oil pills.
After seven days, the patient was re-admitted to the Department of Surgical Oncology purpose for elective surgery. Considering the neoplasm was located in the hepatic flexion, an open right hemicolectomy was performed. During a surgical procedure, there was no bleeding. Patient after surgery felt good and did not complain of pain. The postoperative period was uncomplicated and the patient left the ward in the 7th day after surgery. The patient is now under the care of oncological outpatient at our hospital. After eleven months of surgery performed, there was no recurrence or metastasis.
DISCUSSION
The polyunsaturated omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid from fish and fish oils are widely prescribed in the secondary prevention for cardiovascular diseases. According to many clinical studies they are responsible for a beneficial influence on blood pressure, lipids, vascular and cardiac function mainly through their anti-inflammatory, anti-oxidative and anti-thrombotic actions (1). Their association with coronary heart disease mortality and in particular with sudden cardiac arrest risk reduction has been convincingly documented. For example in GISSI-Prevenzione study, long-term administration of omega-3 PUFA (1 gram daily) significantly decreased the risk of overall (-20%), cardiovascular (-30%), and sudden death (-45%) (2). The omega fatty acids became also of interest in oncology patients, based on the fact that some studies indicate a positive association between the dietary intake of saturated fat and/or animal fat and for example colon cancer risk and an inverse relationship between the intake of fish and fish oil rich in n-3 PUFAs and colon cancer development (3, 4). Nonetheless some patients with CHD with a regular intake of omega fatty acids are diagnosed with colon cancer or another oncological disease that require a radical treatment in form of a surgery. Omega-3 fatty acids do not associate with any adverse effects as stated in recent studies and observations and even it is widely suggested that doses up to 4 g daily concomitant with anticoagulant or antiplatelet drugs do not increase the risk of major bleeding (5, 6). On the other hand the dietary omega-3 PUFAs provoke a hypocoagulant, vitamin K-independent effect in humans, the degree of which may depend on fibrinogen level and requires further investigations (7). In vivo studies have shown that eicosapentaenoic acid (an n-3FA derivative) competes with arachidonic acid as a substrate for cyclooxygenase (COX) and thus, their mechanism of action is thought to result from an antiplatelet effect leading to inhibition of vascular thrombus formation (8). Although multiple studies have proven an increase in bleeding times and a significant decrease in platelet aggregation when taking regularly n-3FA supplements (9, 10, 11). None of the studies concerning vascular, cardiac and abdominal surgery has shown a significant increase in perioperative bleeding events (11, 12, 13). However there is still little evidence in the oncological surgery literature to guide decision-making regarding the cessation of n-3FA supplements around the time of planned surgery, mainly due to the metabolic, hormonal and therefore coagulation changes in oncological diseases (14, 15).
Although little information about influence omega-3 fatty acids for bleeding during operation, the authors of this article believe that in the case of information that the patient regularly takes pills with fish oil, it should be for the safety of the patient discontinued the tablet and planned surgery performed for seven days.
CONCLUSIONS
1. Fish oil rich in omega-3 fatty acids inhibit thrombosis.
2. The patients who take regularly fish oil tablets can have potentially increase the risk for bleeding during surgery.
3. In the case of information that the patient regularly takes pills with fish oil, it should be for the safety of the patient discontinued the tablet and planned surgery performed for seven days.
Piśmiennictwo
1. Simopoulos AP: Omega-3 fatty acids and cardiovascular disease: the epidemiology evidence. Environ Health Prev Med 2002; 6(4): 203-208. 2. Marchiolo R: Omega-3 polyunsaturated fatty acids and cardiovascular diseases. Minerva Cardioangiol 2003; 51(5): 561-576. 3. Reddy BS: Types and amount of dietary fat and colon cancer risk: Prevention by omega-3 fatty acid-rich diets. Environ Health Prev Med 2002; 7(3): 95-102. 4. Caygill CP, Hill MJ: Fish, n-3 fatty acids and human colorectal and breast cancer mortality. Eur J Cancer Prev 1995; 4: 329-333. 5. Harris WS: Expert opinion: omega-3 fatty acids and bleeding – cause for concern? Am J Cardiol 2007; 99(6A): 44C-46C. 6. Watson PD, Joy PS, Nkonde C et al.: Comparison of bleeding complications with omega-3 fatty acids + aspirin + clopidogrel versus aspirin + clopidogrel in patients with cardiovascular disease. Am J Cardiol 2009; 104(8): 1052-1054. 7. Vanschoonbeek K, Feijge MA, Paquay M et al.: Variable hypocoagulant effect of fish oil intake in humans: modulation of fibrinogen level and thrombin generation. Arterioscler Thromb Vasc Biol 2004; 24(9): 1734-1740. 8. Harker LA, Kelly AB, Hanson SR et al.: Interruption of vascular thrombus formation and vascular lesion formation by dietary n-3 fatty acids in fish oil in nonhuman primates. Circulation 1993; 87(3): 1017-1029. 9. Knapp HR: Dietary fatty acids in human thrombosis and hemostasis. Am J Clin Nutr 1997; 65: 1687S-1698S. 10. Schacky C, Weber PC: Metabolism and effect on platelet function of the purified eicosapentaenoic and docosahexaenoic acids in humans. J Clin Invest 1985; 76: 2446-2450. 11. Heller AR, Fischer S, Rossel T et al.: Impact of n-3 fatty acid supplemented parenteral nutrition on haemostasis patterns after major abdominal surgery. Br J Nutr 2002; 87(Suppl. 1): S95-S101. 12. Calo L, Bianconi L, Colivicchi F et al.: N-3 fatty acids for the prevention of atrial fibrillation after coronary artery bypass surgery: a randomized, controlled trial. J Am Coll Cardiol 2005; 45: 1723-1728. 13. Thies F, Garry JM, Yaqoob P et al.: Association of n-3 polyunsaturated fatty acids with stability of atherosclerotic plaques: a randomized controlled trial. Lancet 2003; 361: 477-485. 14. Ulybina IuM, Imianitov EN, Vasil’ev DA et al.: Polymorphism of glucose intolerance and insulin resistance susceptibility genes In oncological patients. Mol Biol (Mosk) 2008; 42(6): 947-956. 15. Van Haren RM, Valle EJ, Thorson CM et al.: Long-term coagulation changes after resection of thoracoabdominal malignancies. J Am Coll Surg 2014; 218(4): 846-854.