*Przemysław Ciesielski1, 2, Agnieszka Kucharczyk2, Małgorzata Kołodziejczak2, Paweł Dutkiewicz1, Sylwia Mossakowska1
Retrospective comparative evaluation of anal fissure treatment methods: superficial posterior internal sphincterotomy and lateral internal sphincterotomy in our own patient population
1Department of General Surgery, County Hospital in Wołomin
Head of Department: Krzysztof Górnicki, MD, PhD
2Warsaw Proctology Centre, Saint Elizabeth’s Hospital, Mokotów Medical Centre, Warsaw
Head of Department: Małgorzata Kołodziejczak, PhD, Associate Professor
Summary
Introduction. Among the numerous methods of anal fissure treatment two have been established for many years: superficial posterior sphincterotomy and left lateral severing of the internal anal sphincter. The results of the treatment of patients with both methods described in the literature are comparable and reports of the duration of healing, perioperative pain and complications in the form of gas and stool incontinence do not differ in a significant way.
Aim. The aim of the paper was to conduct retrospective comparative evaluation of anal fissure treatment methods: superficial posterior internal sphincterotomy and lateral internal sphincterotomy in the authors’ own patient population.
Material and methods. All patients who underwent surgery for chronic anal fissure in 2012-2015 at the Department of Surgery of the Hospital in Wołomin, Poland, were included in the analysis. 97 patients in total underwent surgery (42 men, 55 women). In 14 patients lateral internal sphincterotomy was performed and in the remaining 83 patients superficial posterior sphincterotomy with fissurectomy was performed.
Results. The rate of relapse and incontinence was higher in the group of patients who underwent fissurectomy with superficial posterior sphincterotomy (7 vs 1%); the rate of incontinence was also higher (5 vs 1%). The intensity of pain (averaged) before the operation was comparable (VAS: 7 points).
Conclusions. 1. In the studied group better treatment results were achieved by using lateral internal sphincterotomy. 2. Due to the retrospective nature of the paper as well as lack of baseline and postoperative assessment of sphincter function parameters using anorectal manometry, the results of the study should be treated as preliminary data which require confirmation in a prospective study with sphincterometry assessment before the surgery.

Introduction
At present, over 13 different surgical and non-surgical methods of anal fissure treatment have been reported in medical literature. Some of them, such as anal dilation, are widely considered to be antiquated approaches. Some of the other methods undergo continuous evolution in the search for a method that would combine the highest efficacy with the lowest risk of complications and shortest duration of healing. In terms of these characteristics fissurectomy with superficial posterior sphincterotomy and lateral internal sphincterotomy are definitely the most commonly used methods. The surgical technique used in these methods is relatively simple. The duration of the anal canal healing process, peri- and postoperative complaints as well as treatment efficacy measured as a relapse and complication rate are comparable. The reason for the good results may be the selection of a specific type of procedure for individual patients based on additional indications accompanying the primary diagnosis of anal fissure.
Indications for surgery
The basic indications for both procedures include chronic anal fissure with increased sphincter tone and the lack of efficacy of conservative treatment. However, there are certain characteristics which the surgeon should take into account when selecting a given method.
The main indications for a lateral internal sphincterotomy, apart from the ones mentioned above, include: anterior fissure with increased tone, low, flat margins of the fissure, no concomitant anal fistula.
The indications for fissurectomy with superficial posterior sphincterotomy mainly include posterior fissure with thickened margins as well as circumstances in which histopathological examination is required, i.e. if the suspected cause of the fissure is a non-mechanical one (e.g. Crohn’s disease, squamous cell carcinoma or Bowen’s disease). The coexistence of anal fistula, hypertrophied papilla/polyp in the anal canal or coexistence of haemorrhoids are reasons to choose superficial posterior sphincterotomy with simultaneous excision of other pathological changes (fig. 1a, b).


Fig. 1a, b. Chronic posterior fissure with a hypertrophied papilla and a marginal fold suitable for treatment with posterior sphincterotomy (a) and chronic posterior anal fissure (b)
The selection of the type of operation is also determined by the surgeon’s experience in a given method and the conviction that the method they have learnt brings good results.
Contraindications
Relative contraindications for anal fissure surgery using the methods described are fissures with a normal or decreased sphincter tone.
An absolute contraindication is the lack of patient’s consent to the operation.
Superficial posterior internal sphincterotomy
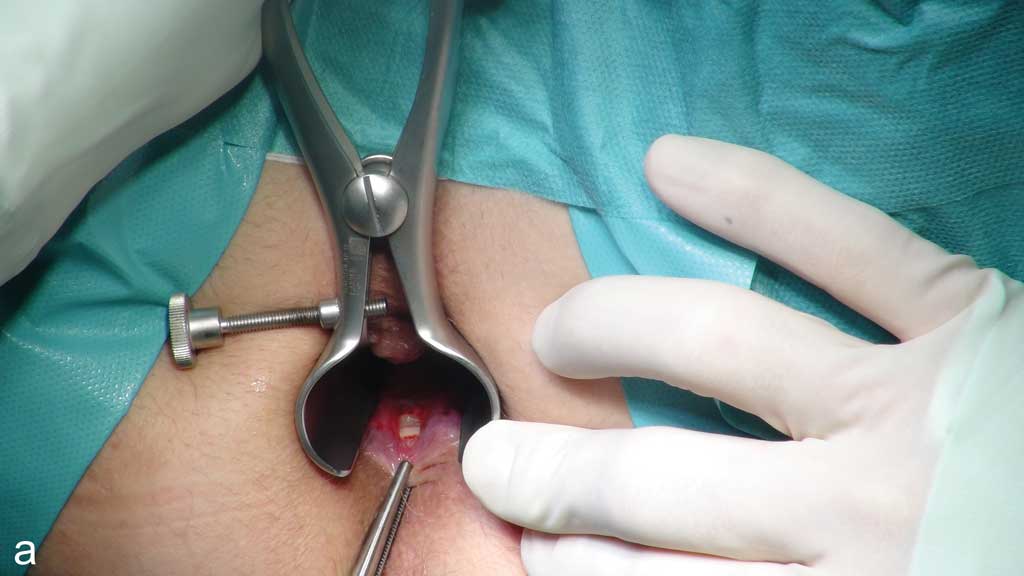
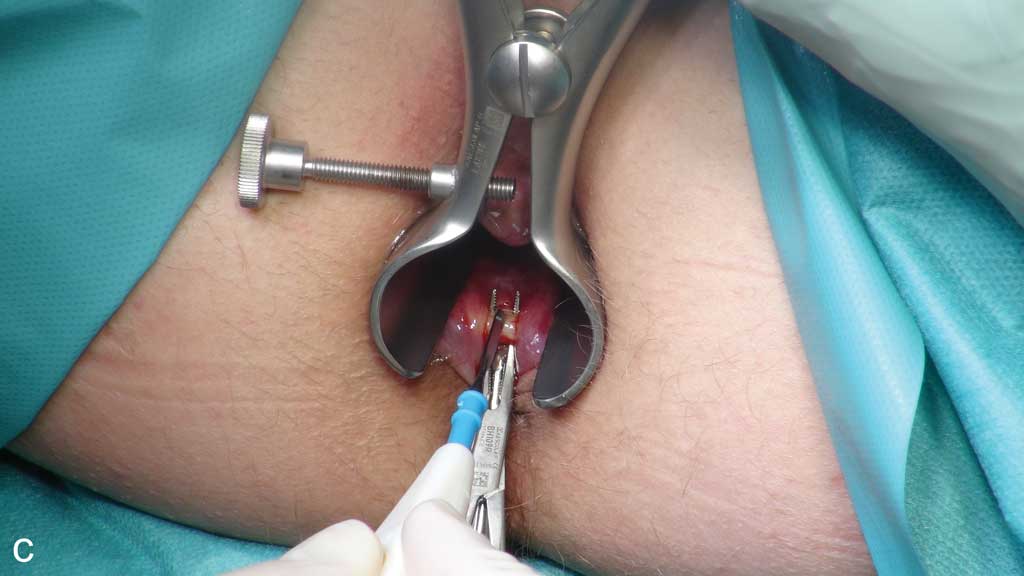
Fissurectomy with superficial posterior sphincterotomy is performed with the patient lying in a lithotomy position. The fissure should be cut around with an elliptical incision and dissected from the sphincter muscles. Subsequently the fissure is excised together with additional elements typically accompanying a chronic fissure – a hypertrophied marginal fold and polypous sentinel papilla of the pectinate line. The next stage involves gentle severing of part of internal sphincter fibres in the line of the fissure with muscle fibres left in the bottom of the fissure. The wound is not sutured after the operation. At the end of the operation it is important to ensure that the surgical wound is smooth and does not contain any structures that would compromise draining, which is indispensable for normal healing (fig. 2a-c).



Fig. 2a-c. Internal sphincter fibres visible at the bottom of the fissure (a), elevated internal sphincter on a dissector (b), severing of internal sphincter muscle fibres (c)
Advantages of the method
This method allows for the excision of all lesions and their histopathological verification, which is indispensable for chronic lesions, primarily with a view to excluding neoplastic diseases as well as inflammatory conditions of the colon. Additional incision of the anoderm in the anal area associated with a lateral sphincterotomy is avoided. It is also worth noting that sphincterotomy conducted at the posterior end is in a sense secured by the puborectalis muscle, which is an important part of the continence mechanism.
Disadvantages
The disadvantages and at the same time complications of the method primarily include keyhole deformation of the anal canal, which occurs in some patients and may be the cause of loss of anal tightness and the associated soiling of underwear and compromised gas and liquid stool continence.
Lateral internal sphincterotomy
Lateral internal sphincterotomy (LIS) is a technically simple method. The patient is put in a lithotomy position. The anoderm is incised on the left side of the anus approximately 1 cm from the anal margin at a length of approximately 15-20 mm. The incision may be radial or curved. Subsequently the internal sphincter should be dissected in the intersphincteric groove up to the level where the upper pole of the fissure projects onto the left side of the anal canal, which in practice usually involves 1/3 or 1/2 of the distal part of the internal sphincter (fig. 3). Once it is visualised the sphincter is severed at its full thickness up to a predetermined place. The surgery is finished by applying pressure on the operated site for 3 minutes for full haemostasis. Layered closure of the wound with absorbable sutures is conditional.

Fig. 3. Lateral internal sphincterotomy
Advantages of the method
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Liang J, Church JM: Lateral internal sphincterotomy for surgically recurrent chronic anal fissure. Am J Surg 2015 Oct; 210(4): 715-719. doi:10.1016/j.amjsurg.2015.05.005. Epub 2015 Jun 27. 2. Aytac E, Erem HH, Remzi FH, Gorgun E: A novel data collection and monitoring system for health status measures in patients undergoing lateral internal sphincterotomy: The Knowledge Program (TKP). Asian J Surg 2015 Jul; 38(3): 134-138. doi:10.1016/j.asjsur.2015.01.001. Epub 2015 Mar 14. 3. Iswariah H, Stephens J, Rieger N et al.: Randomized prospective controlled trial of lateral internal sphincterotomy versus injection of botulinum toxin for the treatment of idiopathic fissure in ano. ANZ J Surg 2005 Jul; 75(7): 553-555. 4. Shao WJ, Li GC, Zhang ZK: Systematic review and meta-analysis of randomized controlled trials comparing botulinum toxin injection with lateral internal sphincterotomy for chronic anal fissure. Int J Colorectal Dis 2009 Sep; 24(9): 995-1000. doi:10.1007/s00384-009-0683-5. Epub 2009 Mar 6. 5. Youssef T, Youssef M, Thabet W et al.: Randomized clinical trial of transcutaneous electrical posterior tibial nerve stimulation versus lateral internal sphincterotomy for treatment of chronic anal fissure. Int J Surg 2015 Oct; 22: 143-148. doi:10.1016/j.ijsu.2015.08.033. Epub 2015 Aug 24. 6. C M G, Babu P, Rao KS: A Comparative Study of Lateral Sphincterotomy and 2% Diltiazem Gel Local Application in the Treatment of Chronic Fissure in ANO. J Clin Diagn Res 2014 Oct; 8(10): NC01-2. doi:10.7860/JCDR/2014/10480.4925. Epub 2014 Oct 20. 7. Menteş BB, Tezcaner T, Yilmaz U et al.: Results of lateral internal sphincterotomy for chronic anal fissure with particular reference to quality of life. Dis Colon Rectum 2006 Jul; 49(7): 1045-1051. 8. Elsebae MM: A study of fecal incontinence in patients with chronic anal fissure: prospective, randomized, controlled trial of the extent of internal anal sphincter division during lateral sphincterotomy. World J Surg 2007 Oct; 31(10): 2052-2057. 9. Kucharczyk A: Kliniczna i obrazowa ocena powierzchownej otwartej sfinkterotomii w leczeniu przewlekłej szczeliny odbytu. Rozprawa na stopień naukowy doktora nauk medycznych. WUM, Warszawa 2013. 10. Taha SA, Merdan I, Kadhim HM: Open midline internal sphincterotomy (with fissurectomy) in the treatment of chronic anal fissure. Bas J Surg 2007; 13. 11. Nahas SC, Sobrado Júnior CW, Araujo SE et al.: Chronic anal fissure: result of the surgical treatment of 220 patients. Rev Hosp Clin Fac Med Sao Paulo 1997 Sep-Oct; 52: 246-249. 12. Queidat DA: Comparative study in anal fissure treatment. J Med Liban 1999 May-June; 47: 164-168. 13. Jonas M, Scholefield JH: Anal fissure Surgical Treatment Evidence-Based and Problem-Oriented. Zuckschwerdt, Munich 2001. 14.