© Borgis - New Medicine 3/1999, s. 12-15
Mieczysław Chmielik, Stanisław Betlejewski
Management of deviation of the nasal septum in children
Department of Paediatric Otolrhinolaryngology, Warsaw Medical School, Poland
Head: Prof. Mieczyslaw Chmielik, M.D.
Department of Otolaryngology, University of Medical Sciences, Bydgoszcz, Poland
Head: Prof. Stanislaw Betlejewski, A.M.
Summary
In this study we investigated the optimal treatment of nasal fractures and nasal deformations in children. An algorithm for the menagament of nasal fractures by children is publicated.
Disorders affecting nasal patency, especially in children, can seriously impair the development of hearing, speech intelligence, and physical development. Therefore, the ability to foresee the possible audiological consequences caused by deformations of the nose, and the evaluation of the possibilities of surgical correction, is very important.
Childhood, the most important period of life, consists of several stages, and the possibilities of nasal injury vary from stage to stage. During delivery, the child is exposed to injuries of the nose because the birth canal has bony walls, and its diameter is usually smaller than that of the head; nasal trauma always occurs during the birth process. The majority of these traumas do not require repositioning, as in the new-born there are mechanisms which can repair deformations spontaneously. This phenomenon, recorded over a long period, is presented in detail by P.Spiewak in this doctoral thesis.
Delivery by Caesarean section can also cause nasal injury, especially if the child is removed rapidly.
Deformations of the nasal endoskeleton in the new-born require surgical intervention if they fail to reposition spontaneously within the first seven days of life. These deformations may cause breathing difficulties in the infant or small child, particularly during feeding and sleep. This apparent coryza may cause the family doctor to prescribe anti-inflammatory, antibacterial, anti-allergic, or anti-oedematous treatment. This is, of course, ineffective. Examination of the nasal cavities in infants is outside the competency of most family doctors, and therefore every infant with persistent coryza should be examined by a laryngologist.
In cases of perinatal fracture of the nasal septum, repositioning of the deformation is necessary. Stiff plastic catheters are introduced into both nasal cavities, and the repositioning is achieved by bringing the catheters close together. To keep the elements in a fixed position, the nose should be packed for 5 to 7 days. Tamponing of the cavities in an infant requires constant observation, and the child should therefore be hospitalised. After removal of the tampons, nasal breathing usually returns to normal.
Nasal traumas do not usually occur in infants, who are normally at home. This type of trauma appears when the child begins to walk. They are very frequent, but the force causing them is usually small. The skeleton of the child´s nose consists mainly of elastic chondral elements, and injuries rarely have a permanent effect. As the child grows, the range of its penetration increases, and the probability of nasal injuries involving larger forces also increases. The child may, for example, be struck by a swing, kicked by a horse, or suffer a traffic accident. In such cases, the physician should, first of all, evaluate the patient´s general condition. It should be remembered that nasal trauma is a cranial trauma, and that dangerous intracranial complications requiring immediate intervention may occur. If this happens, the child should be admitted to a medical centre to ensure proper care.
In the child, the periosteum is relatively strong, and this is why bone fractures without rupture of the periosteum occur. These are called greenstick fractures. Dislocation does not occur very often.
These fractures do not require repositioning, but can sometimes cause a subperichondral or subperiosteal haematoma. Fractures without dislocation in childhood can result in external deformations of the nose - e.g: humps or thickenings. This is why it is very important for parents to be informed of this possible complication immediately after the trauma. In patients with a lateral wall haematoma, the retained blood may suppurate. This is particularly dangerous in haematomas of the septum, because the untreated septal abscess leads to permanent cosmetic deformations and impairment of nasal breathing.
Therefore, in cases of distension of the nasal septum where there is retention of blood or pus, evacuation of the skeletal elements is essential. This is done by a wide semi-transverse incision. Losses in the column or dorsum of the nose should be reconstructed simultaneously by a preserved cartilage implant.
Haematoma or abscess of the nasal septum always requires systemic antibiotic therapy, and compact nasal packing with an antibiotic.
Fractures with dislocation due to nasal trauma in children must be repositioned within 7 days. This is necessary because metabolic mechanisms, including the healing of wounds, occur much more rapidly in the child than in the adult. Within 7 days from the trauma adhesion appears, usually being elastic in this period. A repositioning performed at this stage may seem effective, but within a short time the adhesion can pull the repositioned fragments of bone to the earlier bad position. Thus, the period of up to three weeks after the trauma which some handbooks recommend as being suitable for repositioning seems to be too long for patients at a developmental age.
Repositioning of the nose in children should always be done under general anaesthesia. For safe anaesthesia, basic laboratory investigation is essential. Thus, the repositioning cannot be done in the period immediately after the accident, when it will be too early for oedema to appear. Post-traumatic oedema usually disappears within 4 to 6 days after the trauma, leaving only one day for the repositioning. For this reason, basic laboratory tests should be ordered immediately after the accident, and an appointment with the anaesthetist should be made for the sixth day after the fracture.
Nasal repositioning in post-infancy is analogous to the procedure in the adult patient. The invaginated elements are lifted, and the externally dislocated skeletal fragments are simultaneously pushed into the correct position. After fixing bones and cartilage in the right position, the nose should be filled with an inexpansible material, such as gauze. The nasal packing should remain in place for 7 to 10 days. Materials such as polyurethane sponge or merocel should not be used. These materials are useful in cases of an isolated fracture of the nasal septum, where the bony skeleton of the lateral walls and dorsum of the nose are preserved.
There are not usually any serious contraindications for ambulatory treatment in post-infant children after this procedure. It will be obvious that the nasal repositioning and removal of the tamponade must be done by a laryngologist. Unsatisfactory results after a properly conducted reposition procedure may indicate a fracture in the deeper cranio-facial structures. Computer tomography of the affected region is then essential, and in the case of a lesion of the deep skeletal craniofacial structure, the patient should be under the care of a maxillofacial surgeon. If tomography shows no pathology within the mandibulo-facial complex, the nose repositioning procedure should be repeated.
When a child with a fractured nose comes to the doctor between 7 days and 3 or 4 weeks after the trauma, repositioning of the fractured elements should be attempted. The parents should always be told that the procedure is likely to be ineffective after the above period. If the parents give their consent, the procedure is carried out as previously described. If it is unsuccessful, and the deformation has made a considerable reduction in nasal patency, rhinoplasty should be performed after six months. Patients with a fixed deformation of the septum or lateral walls of the nose, impairing breathing, should also undergo such an operation.
Unfortunately, no Polish laryngology manual to date gives precise instructions for operating procedures on the nasal chondroskeleton or the bony skeleton in children. This is why we consider the publication of methods which can be safely used in children of developmental age to be of considerable importance.
It is the authors´ hope that this report will contribute to the above objective. Most Polish manuals state that resection of the nasal septum should not be carried out on children. However, this is not to be taken as saying that the operation should be postponed until an age of 16 to 18 years.
The patient at a developmental age with the patency of the upper air passages impaired by skeletal deformation should undergo a conservative operation, as recommended by prominent rhinosurgical centres in Poland and elsewhere. This type of operation spares the skeletal elements, previously located in the nose, and places the cartilaginous and bony elements in their proper positions. These criteria are fulfilled by a procedure known as Cottle´s method, established for over 50 years, and regularly improved. There are three essential elements to be considered:
1. Surgical access is obtained by a hemitransfixion incision within the skin of the vestibule of the nose - there is no incision in the mucous membrane;
2. Operating manoeuvres should be performed symmetrically - asymmetrical healing and cicatrization may lead to the dislocation of properly fixed skeletal elements;
3. Cartilaginous elements of the nasal septum must not be removed, as this may inhibit the development of the nose.
Surgical procedures which are in accordance with Cottle´s instructions have been widely described in Polish publications. Because of this, and limited space, only an outline of the operative procedures will be presented here.
The operation begins with a hemitransfixion incision, the perichondrium then being detached from the cartilage symmetrically. The anterior nasal spine is then detached, and dorsally we detach the periosteum form the bone of the nasal septum, obtaining a bilateral symmetrical inferior nasal tunnel.
At this point, where the cartilage joins with the bone and the periosteum joins the perichondrium, the elements are fused in a particular way. The next stage of the operation, the connection of the inferior and superior tunnel, must be performed as a ”sharp operation”. After the liberation of the skeletal elements of the septum, deformation can be estimated.
In the area of the lamina and the nasal crest the cartilage is cut and positioned in the sagittal plane. In cases of bony skeletal deformations, limited resection is possible. The fragments of the perichondrium or the periosteum must be deprived of skeletal support. It is necessary to obtain effective support for the column and the dorsum of the nose during the operation. If the objectives of the operation are achieved, it is completed by closing the semitransverse incision, followed by nasal packing, and by fixation of the nasal skeleton with an external plaster dressing containing a metal plate or thermohardened plastic.
If the operation reveals considerable obstruction of the air passages due to deformation of the lateral walls of the nose, an osteotomy should be carried out in order to mobilise and stabilise the entire skeleton of the bony nasal pyramid. These procedures should only be carried out in highly-specialised rhinosurgical centres, as they require considerable surgical experience. It should be stressed that all procedures aimed at improving the patency of the upper air passages should be performed by a laryngologist, not a plastic surgeon, because only a laryngologist can evaluate all the skeletal elements of the nasal cavities with precision, and choose the best operating procedure.
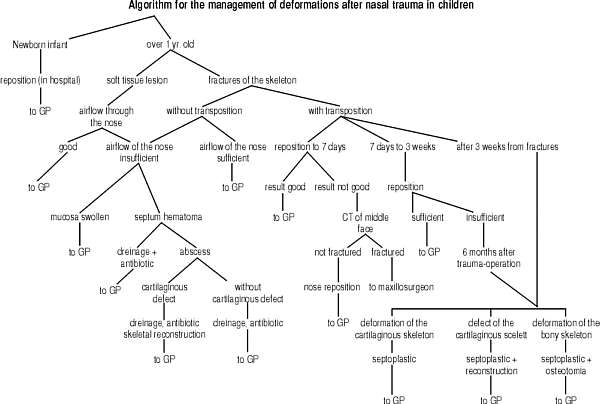
Table 1. Algorithm for the management of deformations after nasal trauma in children
If the operation reveals losses in the bony skeleton or the chondroskeleton of the nose, the operation must include reconstruction of these losses. To achieve this, knowledge of the location, dimension, and aetiology of the losses is essential. The most frequent post-traumatic deformation is a chondral loss in the I, II, or III regions of the nasal septum. This is due to a lack of skeletal support within the column and the dorsum of the nose. Usually, it is caused by a massive injury, or an abscess of the nasal septum. When there is no chondral or bony support in this region, which plays a major role in breathing, a reconstruction with the patient´s or conserved cartilage should be made. The long-term results of a reconstruction using artificial materials are not satisfactory. The application of these materials in the reconstruction of the nose does not seem justified. The partial loss of septum cartilage sometimes only requires the replacement of cartilage fragments with some growth potential - e.g: where there is a loss of full value cartilage in the first region, and consequently lack of support for the nasal dorsum. Where we find sufficiently resistant cartilage in the dorsoventral part of the fourth region, we can install the full value fragments in the first region, or vice-versa. This fragment will give effective support for the nasal apex. The fragment from the first region, injured and deprived of mechanical endurance, is put in the fourth region to ensure support for the mucoperichondral flap placed there.
In many cases, however, the ”boxer´s nose” is deprived of any chondral support for the septum. An effective reconstruction is achieved by installing properly-modelled fragments of costal cartilage into the dorsum and the column of the nose. The implant has the shape of the letter L, or consists of two distinct fragments transplanted to the dorsum and the column. These two fragments are sewn together after introducing them to the nose. Such a reconstruction ensures the right tension for the lateral nasal walls, improving breathing and leaving a good appearance.
It is important to emphasise that impairment of the upper air passages in children can slow development, and may result in a number of diseases of other organs. The influence of prolonged infection of the upper air passages on the condition of the Eustachian tube and the middle ear is particularly important. In many cases, ineffective treatment of serous otitis media follows post-traumatic deformations of the nose. Therefore, we must again emphasise the importance of performing a reconstruction operation at the correct time. This is particularly important in Poland, as this is one of the few countries where the parents of a child with a deviated septum can be advised to have a laryngologist perform the operation at an age of 14-16 years. This recommendation is, as we have mentioned above, completely unjustified nowadays.
To summarise - it is extremely important for patients with post-traumatic nasal deformations to be taken to the general practitioner in good time, going on to the laryngologist, and even to a rhinosurgical centre should this be necessary. The efficient flow of patients between the respective levels of medical care ensures therapeutic success on the one hand, and on the other the lowest possible cost of treatment.
Piśmiennictwo
1. Chmielik M. et al.: Functional and cosmetic long term results after reconstructive operations of the nose in children using preserved homologous cartilage graft. Otolaryng. Pol., 1998, suppl. 27:49-53. 2. Chmielik M., Witkowska A.: Rhinosurgery in children. Otolaryng. Pol., 1993, 47:138-143. 3. Huizing E.: Septum surgery in children, invications. Surgical technique and long-term results. Rhinology 1979, 17:91-93.
