© Borgis - New Medicine 4/2004, s. 109-111
Artur Lorens, Anna Piotrowska, Arkadiusz Wąsowski, Adam Walkowiak, Henryk Skarżyński
Objective method of paediatric cochlear implant system fitting
International Center of Hearing and Speech, the Institute of Physiology and Pathology of Hearing, Warsaw, Poland
Head: Prof. Henryk Skarżyński MD, PhD
Summary
One hundred and two children with implant devices worn over different periods of time were considered for fitting based on eSRT measurements. The first step of the procedure was tympanometry performed by means of an electroacoustic immittance instrument (Madsen Middle Ear Analyser Zodiac 901). Children with abnormal tympanograms were excluded from the study. Subsequently, a change in acoustic admittance resulting from an electrically-evoked stapedius reflex was measured in the non-implanted ear. The same instrument was used after setting it to the "reflex decay” mode. At that stage, eleven children were excluded from the study due to abnormal tympanograms. Nine children reported loudness discomfort before reaching eSRT. Sufficient cooperation was not obtained in fifteen children. Two out of 67 children who had successfully completed eSRT measurements, did not except the new map. Having assessed these results, the authors propose and discuss a procedure for fitting young children based on eSRT measurments.
The paediatric fitting procedure based on eSRT measurements is easy to perform, reliable, and it is worth introducing to clinical practice.
INTRODUCTION
At present, hearing loss is treated with prosthetic devices – either hearing aids or cochlear implants. Hearing aids are chiefly used in mild to severe hearing loss. In profound hearing loss and deafness, the current treatment is based on placement of cochlear implants (9). The cochlear implant system is an electronic hearing prosthetic device, whose action relies on electronic stimulation of the acoustic nerve (7). It consists of an external and an internal part. The internal part is surgically placed in the mastoid portion of the temporal bone and contains a receiver and an electric stimulator in the same housing, with an electrode array. The electrode array extending from the implant housing is inserted into the cochlea (1). The external part is a speech processor which transforms sounds into electric stimuli, according to the algorithm called a sound coding strategy (Fig 1). Fitting of a cochlear implant system, also referred to as „programming” or „mapping”, creates a set of instructions defining the specific parameters of electric impulses used to stimulate the electrodes of the implanted array.
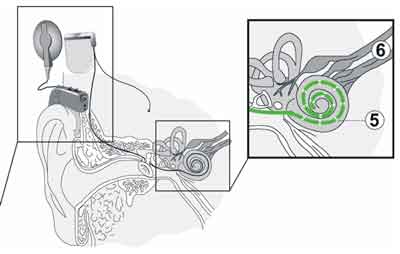
Fig. 1. A schematic representation of the cochlear implant system.
The most important parameters are stimulus amplitudes referring to hearing sensation threshold THRěA and comfort hearing level MCLěA for each stimulating electrode.
The results that implanted children can achieve in the post-operative rehabilitation period depend to a great extent on appropriate fitting of the implant system. Thus, the paediatric fitting methods have been developed and implemented at the Institute of Physiology and Pathology of Hearing, Warsaw (5).
Considerable improvement in the cochlear implant technology has resulted in relaxation of selection criteria (6). An increasing number of very young children are now being evaluated for cochlear implant candidacy. With expanding criteria, the fitting of paediatric cochlear implant patients based on implemented methods has become more difficult and time consuming, as very young prelingually deaf children have no auditory experience and limited communication skills. Therefore, there is a need to introduce objective methods to the process of speech processor fitting.
Objective (electrophysiological) measures do not require active participation from the patient and can provide useful information regarding the THRěA and MCLěA levels. Thus, objective fitting procedures can be useful for fitting very young children (4).
The aim of the study was to propose a paediatric fitting procedure based on electrically-evoked stapedius reflex thresholds (eSRT) measurements.
ELECTRICALLY-EVOKED STAPEDIUS REFLEX THRESHOLDS (ESRT)
The use of electrically evoked stapedius reflex thresholds (eSRT) in cochlear-implanted patients was mooted by Jerger et al. (2). They considered the morphology, latency and amplitude growth of the reflex. The use of electrically-evoked stapedius reflex thresholds has been suggested as a useful means for creating a cochlear implant speech processor programme (8). Results of a previous study demon-strated a high correlation between CI programmes created using behavioural procedures and eSRT recordings to determine MCL levels in experienced implant users in paediatric population (3). Parental reports suggested that the programme created with eSRT measurements is as good as or better than the behaviourally-measured programme. Thus, the eSRT measurement may be considered as a simple, reliable and useful tool to add to the speech processor programming procedure (3, 4).
MATERIAL
In order to develop an objective fitting procedure, the eSRT measurements were performed in a group of 102 implanted children, aged between 1.5 and 7.4 years (mean age 4.2 years) implanted at the Institute of Physiology and Pathology over the last three years. All the children were users of the MEDEL Combi 40+ cochlear implant system. The results were assessed and consequently, the fitting procedure was proposed.
METHOD
The first stage of the procedure consisted of a visual otoscopic examination of the external auditory meatus and tympanic membrane, as well as tympanometric examination (using a Madsen Zodiac 901Middle Ear Analyser) to exclude the influence of external or middle ear conditions. Children with external ear anomalies or abnormal tympanograms were excluded from the procedure. At the second stage, a change in acoustic admittance, resulting from the electrically-evoked stapedius reflex, was measured in the non-implanted ear. The same instrument (Madsen Zodiac 901Middle Ear Analyser) was used after setting it to the "reflex decay” mode. The speech processor was connected to the computer via the MED-EL DIB diagnostic interface box, and controlled using the MED-EL fitting software v4.02. The measure mode was selected and a 500ms duration burst of biphasic pulses was delivered to the selected 6 electrodes. The MCL level was increased until a clear downward deflection of the pre-stimulus baseline was noted (Fig. 2). Subsequently, the MCL level was decreased until no deflection was observed.

Fig. 2. A diagram showing a) absent reflex b) absent reflex, reflex and suprathreshold reflex using the ascending approach and c) suprathreshold reflex, reflex and absent reflex using the descending approach.
This level was considered as eSRT. The third stage involved setting the MCL levels at the level at which the eSRT threshold was identified on 6 measured electrodes, interpolating the MCL levels on the other electrodes, and setting the THR level at the 10% of the MCL level.
RESULTS
The results obtained are shown in fig. 3. Eleven children were excluded from the procedure due to abnormal tympanograms. Nine children reported loudness discomfort before reaching eSRT. Fifteen children did not cooperate sufficiently. Two out of sixty seven children who had successfully completed eSRT measurements, did not except the new map.
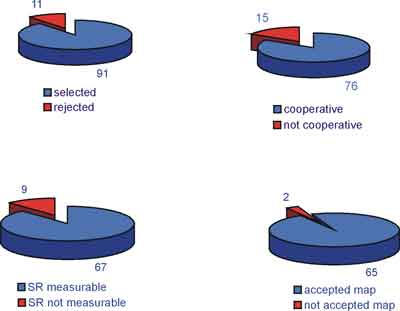
Fig. 3. Children who completed different stages of the procedure.
CONCLUSIONS
The results obtained showed that it was possible to fit the cochlear implant system according to the proposed fitting procedure based on eSRT measurements in more than 50% of the children investigated. The proposed procedure is a simple, reliable and useful tool to complement the speech processor programming in children. It provides useful data in fitting the MCL levels, without overstimulating the child, thus, avoiding any trauma, whilst providing the child with adequate stimulation required for the development of auditory and listening skills. The tool is useful in reducing the time required for a suitable, stable programme for that young patient population who are often difficult to measure. The proposed procedure is a worthwhile supplementary objective method to facilitate appropriate cochlear implant fitting in children.
Piśmiennictwo
1. Helms J., Muller J., et al.: Evaluation of performance with the COMBI40 cochlear implant in adults: a multicentre clinical study. ORL J. Otorhinolaryngol. Relat. Spec. 1997; 59(1):23-35. 2.Jerger J., Fifer R., Jenkins H., Mecklenburg D.: Stapedius reflex to electrical stimulation in a patient with a cochlear implant, Ann. Otol. Rhinol. Laryngol. 1986; 95:151-157. 3.Lorens A., Walkowiak A., Piotrowska A., et al.: ESRT and MCL correlations in experienced paediatric cochlear implant users. Cochlear Implants International 2004; 5(1):28-37. 4. Lorens A., Skarżyński H., Piotrowska A. et al.: Objective methods of post-operative tests in cochlear implant patients. International Congress Series, Elsevier 2003; 1240C:379-383. 5.Lorens A., Zliwa L., Walkowiak A.: Principle of speech processor fitting in the programme of rehabilitation of children after cochlear implantation, New Medicine 1999; 3:33-35. 6.Lorens A., Geremek A., Walkowiak A., Skarżyński H.: Residual acoustic hearing in the ear before and after cochlear implantation. Proceedings of 4th European Congress of Oto-Rhino-Laryngology Head and Neck Surgery, Klaus Jahnke, Markus Fischer; Monduzzi Editore, Italy 2000; I,135-138. 7.Niparko J.K.: Cochlear Implants. Principles & Practices, Lippincott Williams & Wilkins, 2000.8. Stephan K., Welzl-Muller K.: Post-operative stapedius reflex tests with simultaneous loudness scaling in patients supplied with cochlear implants. Audiology 2000; 39(1):13-18. 9.Skarżyński H., Janczewski G., Niemczyk K., Geremek A.: Cochlear implants: state of knowledge, prospects, indications for implantation Otolaryngol Pol. 1993; 47(5):444-51.
