© Borgis - New Medicine 3/2008, s. 60-63
*Lechosław P. Chmielik, Magdalena Frąckiewicz, Mieczysław Chmielik
TUMOURS OF THE BONY FACE IN CHILDREN TREATED IN THE PAEDIATRIC ENT CLINIC IN WARSAW
Department of Paediatric Otorhinolaryngology, Medical University of Warsaw, Poland
Head of Department: Prof. Mieczysław Chmielik, MD, PhD
Summary
Introduction: Tumours of the bony face in children are rare. Among the most commonly found are inflammatory tumours and development anomalies. Histopathologically, the most frequent are neuromas, fibromas, osteomas and lipomas. Inflammatory tumours include abscesses and inflammatory infiltrations. Malignant tumours in this area in children are rare and mainly among them sarcoma or melanoma can be found. Developmental tumours include cysts and fistulas.
Aim: To analyse tumours of the bony face treated in the Paediatric ENT Clinic in Warsaw.
Material and method: There were thirty-six cases of bony face tumours treated in the Paediatric ENT Clinic in Warsaw between 2005 and 2008.
Results: One case (2.77%) was recognized as malignant, and one (2.77%) as locally malignant. Twenty-five cases (69.44%) were found to be developmental tumours. There were also three cases (8.33%) of abscesses and six cases (16.66%) of benign tumours.
Conclusions: The most frequently found tumours of the bony face in children are developmental tumours. All tumours must be subjected to a histopathological examination. In the case of malignant tumour it has to be established whether the tumour is primary or metastatic. In the analysed group even very rare tumours such as epithelioma and ganglioma were found.
INTRODUCTION
Bony face tumours are not noted as a common pathology among children (1, 2), whereas in adults they are a more frequent pathology (3). Among the most frequent tumours in the area of the bony face, developmental tumours and inflammatory tumours are included. Histopathologically the most frequent are angiomas, neuromas, gangliomas, fibromas, osteomas, lipomas, adenomas, Rathke´s pouch tumours, teratomas and also chordomas. As inflammatory tumours abscesses and inflammatory infiltrations can be numbered. Malignant tumours of this area are rare and we can list lymphomas, leukaemias, sarcomas, melanomas and metastatic tumours (neuroblastoma); in rare cases carcinomas can be found.
Among developmental tumours cysts, recesses and fistulas can be listed (1, 2, 4, 5, 6, 7). However, in adults the most frequent tumour affecting this area is carcinoma planoepitheliale medium and highly differential, constituting 80% of all tumours of the bony face. Among the tumours of the bony face we can also include adenocarcinoma, adenocystic carcinoma, mucoepidermal carcinoma, osteocarcinoma, chondrosarcoma, lymphoma, and plasmocytoma. In adults metastatic tumours of the bony face are tumours originating from the kidneys, testis, mammary gland, bronchi and lungs (3).
AIM
The aim of this research was to analyse the cases of bony face tumours treated in the Paediatric ENT Clinic in Warsaw.
MATERIAL AND METHOD
36 cases of bony face tumours, patients aged 12 months to 17 years, treated in the Paediatric ENT Clinic in Warsaw between 2005 and 2008, were analyzed.
RESULTS
Among the patients one case of Malherbe´s tumour; one case of ganglioma; one of neurofibroma; one ossifying fibromas; one fibroma; one granular cell tumour (Abrikossoff tumour); one juvenile angiofibroma; one angioma; three bony face abscesses; ten cysts of the nasal dorsum; one neuroblastoma; nine preauricular fistulas; one retroauricular fistula; and four outgrowths were recognized.
In one case it was a malignant tumour – neuroblastoma – a metastatic lesion found in a 10-month-old girl who was admitted to the Clinic as a complication of acute sinusitis. In the CT of the sinuses destruction of the alveolar process of the maxilla and retrobulbar lesions were noted. In ultrasonography of the abdomen a tumour was noted. In histopathological examination of bone marrow and of material from the alveolar process of the maxilla a neuroblastoma was revealed. A patient was transferred to the Clinic of Oncology in Institute-Statue Centre of Children´s Health, where she received six courses of cytostatic treatment. Remission of lesions in the bones and bone marrow was obtained; primary tumour and suprarenal glands were removed. Chemotherapy is being continued.
A 16.5-year-old boy was admitted to the Paediatric ENT Clinic in Warsaw. For 3 months the patient had been suffering from difficulties in breathing through the nose and recurrent nasal bleeding for 6 weeks. On admission in physical examination blockage of the right nasal cavity and impaired patency of the nose were noted. In endoscopic examination of the nasal cavities a solid, greyish lesion on the right side was found. In radiological examinations (CT, NMR) an abnormal, tissular change that amplified after intravenous contrast was revealed. It was located in the right nasal cavity, pharynx, subtemporal fossa and right maxillary sinus (photo 1).
Photo 1. MRI of juvenile angiofibroma.
Preliminary diagnosis of juvenile angiofibroma was made and the patient was qualified for surgical treatment.
The patient and his parents were informed that during the surgical procedure blood loss might exceed the amount of circulating blood and there might be an eventual need for blood transfusion. The patient and parents gave their consent to the operation but did not give consent for blood transfusion.
Leading doctors filed with the court a motion for granting permission to use blood substitutes in case of an immediate threat to life resulting from bleeding that could not be stopped. The court decided „(...) to grant the permission to use blood and blood platelets concentration during a surgical procedure of tumourectomy in the nasal area”.
The patient demanded individual preparation before the operation, which among other things included administering before the surgical procedure erythropoietin (40 000 units), performing arteriography of the external carotid arteries and right internal carotid artery with embolization of the artery supplying the lesion (right maxillary artery) (photos 2 and 3) and, after consultation with the anaesthesiologist, applying blood-sparing techniques.
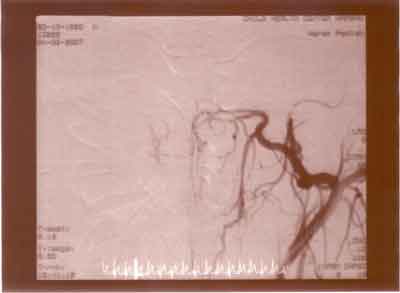
Photo 2. Arteriography of the tumour.

Photo 3. Arteriography after embolization of the tumour.
Course of surgical procedure
1393 millilitres of blood were taken up from the patient without disconnecting this amount from the patient´s blood circulation; the uptake was compensated with HES.
Right-sided maxillotomy was performed, and the lesion was removed in whole from the nasopharynx, right maxillary sinus and pterygopalatine fossa. The result of intra-operative morphology was: Hb-10.7 g%, Ht-30.2% and RBC-3.7 x 106/mm3. Posterior packing and dressing into the postoperative cavity was performed. After bleeding stopped the whole amount of blood taken up before the operation was re-transfused. The material was sent to the Department of Paediatric Anatomopathology of Warsaw Medical University.
In 3.5-month follow-up the patient came to the Clinic with impaired nasal patency on the right side and recurrence of nasal bleeding. In NMR a lesion in the sphenoid sinus was found; it was suspected to be a recurrence. Re-operation was performed; no tumour was noted in the area shown in NMR, but surgeons found pathologically changed, bleeding bone, which was removed.
In twenty-one cases developmental tumours were noted. In a 5-month-old girl admitted to the Paediatric ENT Clinic in Warsaw with a lesion of the dorsum of the nose in NMR a tumour in the area of the nasal dorsum without communication with the central nervous system was revealed. The child was qualified for surgical treatment, which was performed. An arch-like cut was used on the skin of the lateral wall of the nose. Intra-operatively a hard, skin-connected tumour was found, which was removed. In histopathological examination congenital ganglioma was confirmed. Among the extremely rare tumours of the area of the nasal dorsum gangliomas are included (nervous tissue split off). In the postoperative period small necrosis in the area of the skin flap formed but healed.
In our material also a dermoid cyst of the nasal dorsum in a 9-year-old boy was found. Intra-operatively an atypical course between nasal bones and skin ending in the area of the frontal bone was noted. And no as usually cysts of the nasal dorsum come beneath the nasal bones and end in the area of the anterior cranial fossa. Histopathologically it turned out to be a dermoid cyst.
In three cases abscesses were recognized. Treatment included incision and drainage of their cavity and systemic antibiotics.
We also present a case of an 8-year-old boy who was sent to the Paediatric ENT Clinic in Warsaw with a tumour of the cheek. In angio-CT and NMR a tumour in the pterygopalatine fossa penetrating to the orbit and infiltrating the structures of the cheek was revealed. A specimen from the tumour and enlarged lymph node from the submandibular area were taken and sent for histopathological examination. Neurofibroma was confirmed. The patient was qualified for surgical treatment. The operation was performed in Fich C modification on 16.03.2006 with facial nerve preservation. Semi-coronal incision of the head skin was performed, then muscles were cut and the edge of the orbit and jugular bone were revealed, and the bone was removed. In the subtemporal fossa and in the temporal area the mass of the tumour was revealed. The tumour was removed from the subtemporal fossa and tissue of the cheek. The material was sent to the Department of Paediatric Anatomopathology of Warsaw Medical University. After the surgical procedure disturbance of the forehead movements on the left side occurred. Apart from that the postoperative period proceeded without complications. Rehabilitation and orthodontic control were recommended. CT from 29.01.2007 showed no recurrence. In NMR no lesions in the orbit were revealed. In the nasopharynx a tissular mass located in an area much smaller than in the previous examination on the level of occlusion near the buccal muscle and masseter muscle, relating to scar lesions, was revealed. An NMR control in 3 to 6 months was recommended.
Summing up, in the Paediatric ENT Clinic in Warsaw between 2005 and 2008 there were treated: one case (2.77%) of malignant tumour, one case (2.77%) of locally malignant tumour, twenty-five cases of developmental tumours (69.44%), three cases of abscesses (8.33%), and six cases of benign tumours (16.66%).
DISCUSSION
A child as a patient has different specificity both in the course of disease and treatment (1, 4, 6). Histopathologically various are bony face tumours occurring in adults, among which tumours deriving from epithelium (carcinomas) dominate. However, among malignant neoplasms in children tumours deriving from lymphatic tissue dominate. In children tumours demonstrate more dynamics of growth than in adults. In otolaryngologists´ opinion in the case of bony face tumours both in children and in adults to make a final diagnosis taking material for histopathological examination is necessary. When treating malignant tumours of the bony face in adults first the maximum should be surgically removed (except e.g. lymphomas) and then complementary chemotherapy or radiotherapy should be planned (3). In the case of malignant tumours in children to achieve the optimal method of treatment good cooperation between the oncologist and surgeon is needed. It is vital to introduce immediately correct cytostatic therapy, owing to which significant reduction or even total remission of the tumour is possible. This was shown in the presented case of neuroblastoma (4, 7), where remission of metastatic tumours and significant decrease of the primary focus were gained. It enables a significant reduction of the extent of surgical treatment. This method of treating malignant bony face tumours in children seems to be the most optimal one (4, 8). Both in children and in adults it is important whether the tumour of the bony face is a primary or metastatic tumour.
Some authors advise conservative treatment of developmental tumours of the bony face, whereas others because of a potential risk of neoplastic process in old age recommend surgical treatment (9). In the cases we presented we prefer surgical treatment, owing to which on the one hand we achieve the removal of abnormal tissue and on the other hand it was possible to make the final diagnosis, as in cases of ganglioma in the area of the nose (10). No disputable indication for surgical treatment of developmental tumours is a reoccurring inflammatory state (after the acute phase is controlled). The treatment of choice for abscesses is surgical drainage and general antibiotics.
CONCLUSIONS
1. The most frequently found tumours of the bony face in children are developmental tumours.
2. All tumours must be subjected to a histopathological examination.
3. In case of malignant tumour it has to be established if the tumour is primary or metastatic.
4. In the analysed group even very rare tumours such as epithelioma and ganglioma were found.
5. Neoplasms in children have different specific character in comparison to those in adults, which is reflected in different therapeutic process and prognosis.
Piśmiennictwo
1. Chmielik M.: Otolaryngologia Dziecięca. W-wa PZWL, 2001; 89-92. 2. Chmielik M.: Otolaryngologia Dziecięca. W-wa PZWL 2001; 219-230. 3. Osuch - Wójcikiewicz E.: Otorynolaryngologia praktyczna pod red. Janczewski G. Via Medica 2005; 353-357. 4. Perek D.: Otolaryngologia Dziecięca pod red. Gryczyńska D. a-medica pres 2007; 492-511. 5. Hassman-Poznańska E.: Otolaryngologia Dziecięca pod red. Gryczyńska D. a-medica pres 2007; 423-436. 6. Hassman-Poznańska E.: Otolaryngologia Dziecięca pod red. Gryczyńska D. a-medica pres 2007; 456-467. 7. Brodeur GM.: Clinical and biological aspects of neuroblastoma. In Vogelstein B, Kinzler KW. (eds) The genetical basis of human cancer. New York: McGraw-Hill, 1998. 8. Pietniczka M, Kukwa A, Krajewski R, et al.: The possibilities of surgical treatment of tumours of the head and neck in children. New Medicine vol. IV no 2/2001; 28-30. 9. Chmielik LP, Krajewski R.: Neurofibroma of the pterygo-palatine fossa in children. New Medicine vol. XI no 4/2007; 88-89. 10. Chmielik LP, Boratyński W.: Ganglioma of the base of the nose in children. New Medicine vol. XI no 4/2007, 96-97.
