© Borgis - New Medicine 2/2009, s. 31-34
*Aneta Dąbek1, Janusz Domaniecki1, Marek Wielochowski2, Jan Gajewski1
A pilot study to evaluate treatment efficacy in patients with primary Raynaud´s phenomenon
1University of Physical Education in Warsaw, Chair of Rehabilitation
Head of the Chair of Rehabilitation: prof. dr habilitatus of medicine Janusz Domaniecki
2Higher School of Pedagogy, Polish Teachers´ Union in Warsaw
Summary
Aim.The aim of the study was to evaluate the objective and subjective efficacy of the following treatments for patients with primary Raynaud´s phenomenon: drug (medication) therapy, physical therapy (infrared sauna) and relaxation (Schultz autogenic training).
Material and method. The study involved 29 outpatients with a diagnosis of primary Raynaud´s phenomenon treated at Warsaw Medical University´s Department of Dermatology. The patients were randomised into four groups receiving drug therapy (controls), relaxation therapy, physical therapy and multimodal (comprehensive) therapy. Treatment was administered for 14 weeks in all groups. All patients were evaluated three times: before starting treatment (baseline) (1), and after 7 (2) and 14 (3) weeks of treatment. The following quantitative data were obtained:
– incidence of manifestations of primary Raynaud´s phenomenon (questionnaire)
– subjective evaluation of pain and sweating (VAS scale)
– subjective impression of treatment efficacy (VAS scale)
– evaluation of microcirculation by capillaroscopy before and after treatment (two evaluations).
Results. The highest subjective and objective treatment efficacy was reported in the multimodal therapy group and the lowest in the drug therapy group. The relaxation therapy group demonstrated a significant decrease in the incidence of ischaemic attacks without significant differences with respect to the other parameters (pain, sweating) between the first and third assessments.
Conclusions. The study ought to be continued with a larger group of patients involved.
Introduction
Effective treatment of Raynaud´s disease and Raynaud´s syndrome is becoming increasingly important as the number of patients seeking specialist help with their Raynaud´s symptoms at dermatology departments is growing every year.
Raynaud´s phenomenon may currently affect up to 20% of the general population [1], though sources cite various prevalence figures, from 4.6% to 30% [2, 3, 4].
Earlier definitions of Raynaud´s phenomenon defined it as circulatory disturbances in the distal parts of the body, mainly the hands and feet. Contemporary researchers [5, 6, 7] believe Raynaud´s phenomenon to represent a systemic illness with a potential to produce pathological vasospasm at any site, including the heart, kidneys, lung, oesophagus, CNS, or retina (fig. 1).
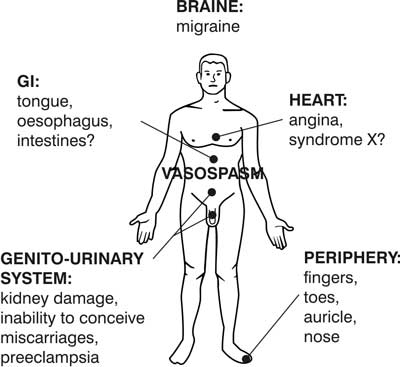
Fig. 1. Generalised vasopastic tendency in patients with Raynaud´s phenomenon [Lauch & Belch].
The vasospastic attacks last 15-45 minutes [8]. An ischaemic attack in the hands manifests as intense pallor of the fingers and the patient complains of impaired sensation ("numb fingers”). After the ischaemic phase, the fingers become red and swollen, and the patient feels a severe throbbing pain.
The causes of primary Raynaud´s phenomenon are believed to be exaggerated emotional responses (stress) or cold. Accordingly, causal treatment of this condition should consist in reducing anxiety and limiting cold exposure. Drug therapy is the only method commonly used in the treatment of primary Raynaud´s phenomenon in Poland. Pharmacotherapy often fails to bring about the desired effect and is costly, while also being cumbersome for the patients, who have to take their medications 3-4 times a day and often experience headaches, flushed skin, low blood pressure and gastroesophageal reflux [8, 9]. Untreated Raynaud´s syndrome may lead to fungal infections of the nails, paronychia, or keratoconus. Some authors [2, 10, 11] claim that primary Raynaud´s may, after several (up to 20) years, transform into secondary Raynaud´s syndrome.
Aim
The aim of the study was to assess the subjective sense of efficacy of drug therapy (medication), physical therapy (IR sauna) and relaxation therapy (Schultz autogenic training) in the treatment of primary Raynaud´s phenomenon.
Material and Methods
The study involved 29 outpatients attending the Warsaw Medical University Department of Dermatology at Koszykowa St. in Warsaw who had been diagnosed with primary Raynaud´s phenomenon on the basis of history and capillaroscopic evidence. The patients were randomised into four groups receiving drug therapy (controls), relaxation therapy, physical therapy and multimodal (comprehensive) therapy. Treatment was administered for 14 weeks in all groups. All patients were evaluated three times: before starting treatment (baseline) (1), and after 7 (2) and 14 (3) weeks of treatment. The following quantitative data were obtained:
– incidence of manifestations of primary Raynaud´s phenomenon (questionnaire)
– subjective evaluation of pain and sweating (VAS scale)
– subjective impression of treatment efficacy (VAS scale)
– evaluation of microcirculation (capillaroscopy) before and after treatment (two evaluations).
Drug therapy group (controls)
The patients in this group took Vessel Due – one of many kinds of medicines
available on the market for the treatment of Raynaud´s disease – according to their attending doctor´s orders.
Relaxation therapy group
These patients were subjected to Schultz autogenic training in addition to the drug therapy.
Schultz autogenic training is a relaxation technique based primarily on suggestion and imagination. Many specialists believe that this technique exerts the most potent effect on blood vessels. This effect is especially due to one of its elements, namely, the induction of a sense of warmth in the limbs [12].
The patients in this group received CDs with a recording of a training session and were instructed to relax for 20 minutes every day. The patients learned to relax using a Blue Watcher feedback device (fig. 3), which was also used to monitor their progress.

Fig. 2. The hands and feet of a 30-year-old female patient with Raynaud´s disease following an ischaemic attack [own materials].

Fig. 3. Patient during biofeedback session with Blue Watcher [own materials].
Physical therapy group
The patients in this group used the infrared sauna.
An IR sauna looks like a conventional sauna and produces similar effects but uses a different source of heat, namely infrared radiators, instead of an electric furnace. The radiators emit biologically active infrared energy. Unlike Finnish saunas, where heat is carried by the air, in IR cabins only 20% of the energy warms the air and 80% penetrates deep into the skin (0.5-3 mm), where it transforms into heat [13]. Infrared sauna sessions are completely safe, as proved by Japanese and Chinese researchers who used the sauna in patients with risk factors for myocardial infarction [14], chronic pain [15], depressive symptoms [16] or heart failure [17]. Infrared sauna sessions administered to the patients with Raynaud´s phenomenon were supposed to lower anxiety and dilate cutaneous blood vessels. This effect is consistent with Dastre-Morat´s law, which states that high temperature "reduces peripheral circulatory resistance, mainly via dilation and reduced tension of peripheral vessels and the opening of arteriovenous connections” [18].
The patients with Raynaud´s disease attended an IR sauna three times a week for 14 weeks. Each session lasted 30 minutes. The sauna was pre-warmed before the session to a temperature of 65°C. Following a sauna session, the patients took a shower, got dressed, and rested in a lying or sitting position for a minimum of 15 minutes. We recommended increasing their daily intake of fluids by at least 1 litre.
Multimodal (comprehensive) therapy group
The patients took drugs and were subjected to relaxation therapy and IR sauna sessions.
Results
ANOVA revealed statistically significant differences (p=0.1426) in the patients´ subjective assessment of treatment efficacy between the groups (Fig. 5).

Fig. 4. Infrared (IR) sauna: outside and inside view [own materials].
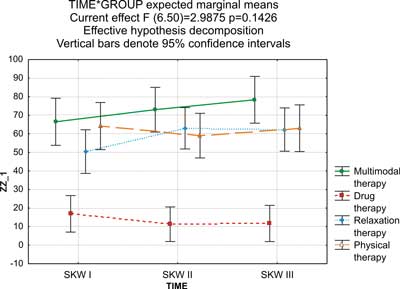
Fig. 5. Subjective assessment of the efficacy of treatment of primary Raynaud´s phenomenon in the four treatment groups (drug therapy, relaxation therapy, physical therapy, and multimodal therapy) by duration of treatment (SKW I – baseline, SKW II – after 7 weeks of treatment, SKW III – after 14 weeks of treatment).
Additionally the Kruskal-Wallis test demonstrated statistically significant differences (p=0.0299) in objective assessment of treatment efficacy by capillaroscopy between the groups.
Table 1 presents the results of capillaroscopic evaluation of small vessels of the nail folds on completion of treatment as compared to baseline.
Table 1. Capillaroscopic evaluation after 14 weeks of treatment by treatment group.
| Variable | Controls | Relaxation | Physical therapy | Multimodal therapy |
| Deterioration | 4 | - | - | - |
| No change | 4 | 4 | 5 | 3 |
| Improvement | 1 | 3 | 1 | 3 |
There were statistically significant differences (p=0.0496) in the incidence of Raynaud´s phenomenon between individual treatment groups (tab. 2).
Table 2. Incidence of ischaemic attacks in patients with Raynaud´s disease on completion of therapy (measurement 3).
| Variable | Controls | Relaxation | Physical therapy | Multimodal therapy |
| Incidence of attacks (0-7) per week | 5.7 + 1.8 | 3.5 + 2.8 | 2.85 + 1.9 | 3.33 + 1.6 |
Discussion
To begin with, it is not easy to assess the efficacy of treatment of primary Raynaud´s phenomenon because some patients have progressive disease. In these patients, a finding of no deterioration should be interpreted as therapeutic success. The situation is additionally compounded by the fact that Raynaud´s loops do not always show on capillaroscopic assessment [3, 6, 19]. Many researchers differ in their views on such a cardinal issue as the distinction between primary and secondary Raynaud´s. Following Allen & Brown, who specified criteria to define Raynaud´s disease that accounted for the difficulties in differentiating between Raynaud´s disease and Raynaud´s syndrome [19], I assumed that my patients should fulfil the following criteria: at least two-year history of Raynaud´s phenomenon; no pathologies interpretable as underlying causes of Raynaud´s phenomenon; and microcirculatory disturbances in the hands revealed by capillaroscopy.
Randomisation into treatment groups is another problem related to treatment efficacy assessment. Kulmatycki et al. [20] demonstrated that personality traits have an effect on the ability to relax. Highly extrovert people, unlike introverts, do not have difficulty learning to relax. Randomisation may adversely affect therapeutic success rates. A person who finds it difficult to relax might tolerate the sauna. The methodology of this study precluded targeted placement of a patient in a particular group. Ethics, in turn, rules out the possibility of no care being provided to the control group, which was the reason behind the use of drug therapy in the control group and drug therapy plus another modality (infrared sauna or relaxation therapy) in the other groups.
While clinicians specialising in the treatment of Raynaud´s phenomenon concur that the underlying cause is anxiety [1, 2, 11], there is no scientific evidence to confirm this theory. This issue is of central importance with regard to the efficacy of treatment of primary Raynaud´s phenomenon. It is known that the best kind of treatment is causal. In the case of patients with primary Raynaud´s phenomenon, drug therapy is a symptomatic treatment and often fails to produce the desired results [21]. Relaxation training, and particularly Schultz autogenic training, has an advantage over drug therapy in that there are no side effects. Relaxation therapy is also not associated with repeated costs. Foreign papers are often concerned with causal treatment for patients with primary Raynaud´s phenomenon. The authors often explore the utility of biofeedback. As early as 1980, researchers from Harvard University [22] compared the efficacy of treatment in patients with primary Raynaud´s phenomenon subjected to three different types of relaxation training: autogenic training, progressive relaxation and biofeedback-based relaxation training. While no significant differences in efficacy were revealed between the different types of relaxation training, the study employed a surprisingly innovative approach to the treatment of Raynaud´s phenomenon. In 2001, Middaugh et al. [23] conducted a study aiming to teach biofeedback regulation of temperature and muscle tone to patients with Raynaud´s phenomenon using a biofeedback device. The study showed that patients with Raynaud´s phenomenon, unlike the control group, found it difficult to learn the biofeedback regulation skill. Only 34.6% of the patients with Raynaud´s disease learnt to regulate their body temperature and 55.4% of the Raynaud´s sufferers learnt to relax their muscles.
Infrared sauna is another unconventional method employed in the treatment of patients with primary Raynaud´s phenomenon. The IR sauna exerts an effect not only on peripheral blood flow but also on anxiety, which is the underlying cause of this condition. The present study confirmed that the most effective treatment, both in the subjective opinion of the patients and according to an objective (capillaroscopic) evaluation, is multimodal (comprehensive) therapy. Psychosomatic disorders, of which Raynaud´s disease doubtless is one, require a holistic approach to the patient´s health problems.
Conclusions
1) The highest subjective (VAS scale) and objective (capillaroscopy) efficacy of treatment for primary Raynaud´s phenomenon was found in the multimodal therapy group. However, the high efficacy rating was noted in the absence of a considerable reduction in pain or sweating in this group.
2) The lowest subjective and objective treatment efficacy was seen in the control (drug therapy) group. This was presumably related to the many adverse effects of calcium channel blockers and the fact that patients did not take their medicines regularly.
3) The incidence of Raynaud´s attacks fell most markedly in the relaxation therapy group.
4) These results need to be confirmed in a study on a larger sample.
Work done within the framework of statutory research conducted at the Chair of Rehabilitation, University of Physical Education in Warsaw within project DS. 110, Treatment of Primary Raynaud´s Syndrome, financed by the Minister of Science and Higher Education
Piśmiennictwo
1. Brown MK et al.: The Effects of Stress, Anxiety and Outdoor Temperature on the Frequency and Severity of Raynaud´s Attacks: The Raynaud´s treatment study. Journal of Behavioral Medicine 2001; Vol. 24, No 2. 2. Coffnan JD: Cutaneous changes In Peripheral Vascular Disease. In: Dermatology in General Medicine. Ed.: Fitzpatrick T, Essen A, Wolff K, McGrow-Hill Inc. San Francisco, 1993; 2075-2089. 3. Rychlik-Golema W et al.: Fenomen Raynaud – wcišż aktualny problem kliniczny. Przeglšd Lekarski 2002; 59, 1. 4. Ciecierski M, Migdalski A, Jawień A: Choroba i zespół Raynauda. Przewodnik Lekarza 2000; 6: 64-66. 5. Aron JH et al.: Cerebral oxygen desaturation after cardiopulmonary bypass in a patient with Raynaud´s phenomenon detected by near-infrared cerebral oxymetry. Anesth Analog 2007; 104, 1034-1036. 6. Sicińska J, Rudnicka L: Choroba Raynauda i objaw Raynauda w przebiegu kolagenoz. Pol Arch Med Wewn 2002; 108(4), s. 1011-1022. 7. Kozielski J et al.: Zachowanie się parametrów badań czynno?ciowych układu oddechowego w chorobie Raynauda. Pol Arch Med Wewn 1992; 87(6), s. 341-344. 8. Rychlik-Golema W et al.: Fenomen Raynaud – wcišż aktualny problem kliniczny. Przeglšd Lekarski 59, 1: 2002. 9. Migdalski A, Ciecierski M, Jawień A: Leczenie ambulatoryjne chorych z objawem Raynauda, Nowa Medycyna 2001; 112: 6-8. 10. Jędrasik M et al.: Badanie elektroencefalograficzne u chorych z napadami fenomenu Raynauda, Polski Przeglšd Chirurgiczny 1992; 64, 1: 49-52, 1992. 11. Lauch CS, Belch JJF: Chirurgia naczyniowa: objawy Raynauda – zaburzenie kurczu naczyniowego. Chirurgia Współczesna 1993; 1(3): s. 192-197. 12. Siek S: Autopsychoterapia; Wyd. Psyche. 13. Chojnowski J et al.: (2006), Czy przegrzewanie ogólnoustrojowe w saunie w podczerwieni ma wpływ na dobowy profil glikemii u chorych na cukrzycę? Balneologia Polska 1999; nr 4, 231-234. 14. Imamura M et al.: Repeated thermal therapy improves impaired vascular endothelial function in patients with coronary risk factors. J Am Coll Cardiol 2001; 38: 1083-1088. 15. Masuda A et al.: The effects of repeated thermal therapy for patient with chronic pain. Psychotherapia psychosomatyka 2005; 74(5): 288-294. 16. Masuda et al.: Repeated thermal therapy diminishes appetite loss and subjective complaints in mildly depressed patients. Psychosomatica Medicine, 2005; 67(4): 643-647. 17. Kihara T et al.: Repeated sauna treatment improves vascular endothelial and cardiac function in patients with chronic heart failure. J AM Coll Cardiol 39, 2002; s. 754-759. 18. Mika T, Kasprzak W: Fizykoterapia, Warszawa 2003. 19. Jędrasik M, Zajšc S: Studium naturalnej historii napadów fenomenu Raynauda. Polski Przeglšd Chirurgiczny, 1992; 64(1): s. 43-47. 20. Kulmatycki L, Miedzińska B: Podatno?ć na relaksację a cechy osobowo?ci. Postępy Rehabilitacji 1999; t. XII, z. 3, s.151-159. 21. Wesołowski J et al.: Badanie przepływu krwi w tętnicach palców w fenomenie Raynauda za pomocš Dopplera o wysokiej częstotliwo?ci, Polski Przeglšd Chirurgiczny 1997; 69, 5: 512-517. 22. Keefie FJ, Surwit RS, Pilon RN: Biofeedback, autogenic training and progressive relaxation In the treatment of Raynauds disease; Journal of Applied behavior Analysis, 1980; 13: 3-11. 23. Middaugh JS et al.: The Raynaud´s Treatment Study: Biofeedback Protocols and Acquisition of Temperature Biofeedback Skills. Applied Psychophysiology and Biofeedback, 2001; Vol. 26: No 4.
