© Borgis - Nowa Stomatologia 4/2012, s. 170-173
Monika Adamczyk, *Agata Gieorgijewska
Diagnozowanie w periodontologii na podstawie aktualnych klasyfikacji
Periodontal diagnosis based on commonly used classifications
Department of Oral Medicine and Periodontal Disease, Medical University of Warsaw
Head of Department: prof. Renata Górska, MD, PhD
Streszczenie
Podstawą prawidłowego postępowania leczniczego jest postawienie właściwego rozpoznania. Duże znaczenie mają powszechnie stosowane klasyfikacje jednostek chorobowych, które dzięki usystematyzowaniu objawów znacznie ułatwiają i przyspieszają prawidłową diagnozę.
Powszechnie uznaną i stosowaną klasyfikacją chorób przyzębia jest Klasyfikacja Amerykańskiej Akademii Periodontologicznej (AAP) z 1999 roku, uwzględniająca jako kluczowy parametr utratę przyczepu łącznotkankowego (CAL) i na jego podstawie oceniająca stopień zaawansowania choroby oraz postać – zlokalizowaną lub uogólnioną.
W 2008 roku Offenbacher i wsp. zaproponowali nowy podział chorób przyzębia opierający się na takich parametrach, jak głębokość kieszonki (PD) oraz krwawienie przy zgłębnikowaniu (BOP), z całkowitym pominięciem CAL, mający na celu przede wszystkim zweryfikowanie obecności lub brak aktywnego stanu zapalnego, którego wykładnikami są właśnie BOP i PD. Czy słusznie? W niniejszej pracy przeanalizowano badania periodontologiczne trzech pacjentów i porównano otrzymane rozpoznania w odniesieniu do obu klasyfikacji.
Ustalenie jednej, słusznej klasyfikacji spośród proponowanych dwóch jest zadaniem trudnym, a nawet niemożliwym, gdyż każda z nich jest niedoskonała i każda interpretuje diagram periodontologiczny względem innych aspektów. W celu pełnej oceny tkanek przyzębia naszych pacjentów, zasadne wydawałoby się zatem stosowanie obu klasyfikacji jednocześnie.

INTRODUCTION
The most fundamental for proper treatment is right diagnosis. Unspecific symptoms occur in many diseases, that is why differential diagnosis plays a highly significant role.
The use of classifications, which methodize disease symptoms, quickens and facilitates proper diagnosis.
Periodontal diagnostics is not easy to perform and it is based on exhaustive examination including not only teeth and periodontium but the whole stomatognathic system. It is also important to perform additional examination, e.g. radiological, microbiological and genetic or blood examination.
“Periodontitis” is not a full diagnosis and does not give any information about the course of treatment. According to G. C. Armitage (1) answering these questions should precede a definitive diagnosis:
– What is the patient’s periodontal status?
– Is it acute?
– Is the disease localized or generalized?
It requires periodontal examination including evaluation of pocket depth, clinical attachment loss, plaque and bleeding index, root furcation status and teeth looseness. Unfortunately, dentists rarely perform such examination and impede or even preclude right diagnosis and proper treatment.
Let’s analyze the two basic periodontal parameters defining the diagnosis.
PD – pocket depth – the distance between the gingiva margin and the pocket bottom (the surface of the attachment)
CAL – clinical attachment loss – the distance between the pocket bottom and the cementoenamel junction (CEJ) (2).
It is possible to observe different situations:
– When the gingiva margin is located over the cementoenamel junction level (CEJ is invisible) – fig. 1
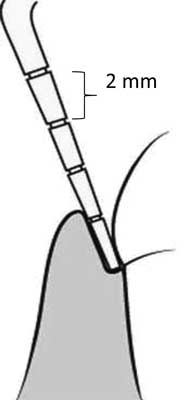
Fig. 1. PD = 0, CAL = 0.
– When the gingiva margin is located on the same level as cementoenamel junction – fig. 2
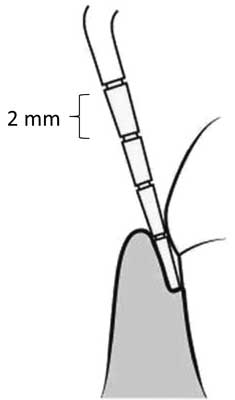
Fig. 2. PD = 2, CAL = 1.
– When the gingiva margin is located under the cementoenamel junction level, there is a gingiva recession (CEJ is visible) – fig. 3
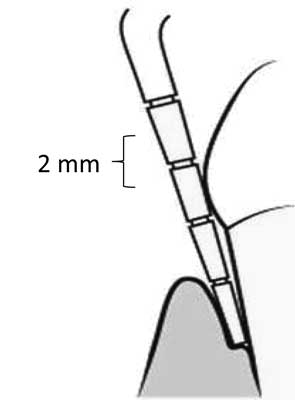
Fig. 3. PD = 2, CAL = 4.
PD evaluation is not a challenge, while the CAL evaluation may be difficult, especially when the cementoenamel junction is not yet visible (PD > CAL). Figure 4 shows such situation and helps to provide proper CAL measurement.
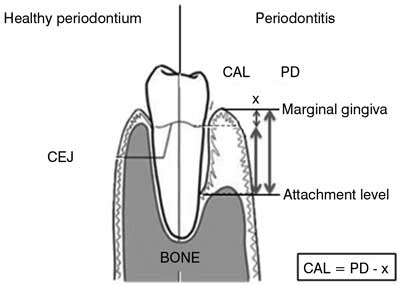
Fig. 4. CAL evaluation, when pocket depth value i higher than attachment loss and the cementoenamel junction is sightless.
PD and CAL are the most important points of reference applied in two commonly used classifications.
The most frequently used one is the American Academy of Periodontology classification (1999). Its main disease division consists of gingivitis, chronic periodontitis, aggressive periodontitis, periodontitis concomitant with general diseases, acute periodontitis muco-gingival abnormalities (2, 3).
The criteria which differentiates gingivitis and periodontitis is clinical attachment loss caused by bone destruction due to chronic inflammation. CAL is also a key factor classifying the severity and form of periodontitis.
Following the AAP, we distinguish different stages of chronic periodontitis:
– light (CAL – 1-2 mm)
– moderate (CAL – 3-4 mm)
– severe (CAL > 5 mm)
and two forms of chronic periodontitis:
– localized (CAL present in less than 30% examined surfaces)
– generalized (CAL present in 30% and more examined surfaces)
The AAP classification also includes the etiology which allows to differentiate the disease between chronic, aggressive and periodontitis concomitant with general diseases – when the clinical attachment level is present or between gingiva diseases if there is no clinical attachment loss.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Armitage GC: Periodontal diagnoses and classification of periodontal diseases. Periodontology 2000; Vol. 34, 2004, 9-21. 2. Banach J, Dembowska E, Górska R et al.: Praktyczna periodontologia kliniczna. Wydawnictwo Kwintesencja 2004; 245-247. 3. Armitage GC: Development of a classification system for periodontal diseases and conditions. Ann Periodontol 1999; 4(1): 1-6. 4. Offenbacher S, Barros SP, Beck JD: Rethinking Periodontal Inflammation. J Periodontol 2008; 79(8): 1577-1584.
