© Borgis - New Medicine 1/2013, s. 28-30
*Mihály Dió1, Tibor Deutsch1, Judit Mészáros2
Conceptual design of an intelligent ‘telediabetology” system
1Department of Medical Imaging and Technology, Faculty of Health Sciences, Semmelweis University, Budapest, Hungary
Head of Department: Éva Kis, PhD
2Faculty of Health Sciences, Semmelweis University, Budapest, Hungary
Dean of the Faculty of Health Sciences: Prof. Judit Mészáros, PhD
Summary
The widespread adoption of information-communication technology in everyday life including the Internet and mobile phones provides a great opportunity to improve the organisation of Diabetes Mellitus (DM) care delivery. This paper presents the conceptual design of an intelligent information system to provide tele-monitoring and tele-care services for insulin-treated diabetic patients twenty four hours per day at the point and time where and when it is needed. The proposed system supports a new visit form called virtual visit during which the patient contacts a computer program instead of a real doctor or nurse for assistance, guidance or advice. In addition to patient self-management, health care personnel are also supported by a wide range of information management and decision support services. We expect that the new architecture shall improve efficiency, patient satisfaction and health results.
Introduction
Diabetes management is far from having reached the desired therapeutic targets. To the contrary, because of the increase of DM prevalence, ageing population and health care costs the current situation shall become worse (1). Several difficulties are consequences of inadequate information management and problem solving.
Traditionally patients and providers communicate during personal encounters called contact visits. Between those visits, however, diabetic patients make hundreds of choices each day but patients lack the knowledge and/or motivation to manage themselves as required. To enable patients to be effective self-managers of their diabetes, they need to be provided with the information and support necessary to make informed decisions day and night. Similarly, between two subsequent visits care providers do not know what is happening to their patients. Clearly they should be notified about impending or actual problems to enable timely feedback or action.
To improve patient safety and also the efficiency and quality of diabetes care, several chronic care models have been developed. These include the ‘self-management” and ‘collaborative management” models (2). The widespread adoption of ICT in everyday life, including the Internet and mobile phones, is providing a great opportunity to improve the organisation of DM care delivery (3-6). Several tele-medicine systems have been published in the literature (7, 8).
Aim of the study
We intend to develop an intelligent information system, which provides comprehensive tele-monitoring and tele-care services for insulin-treated diabetic patients day and night. Patients” home monitoring and life style data are continuously monitored/interpreted and the management team (including the patient) is informed/assisted in the decision making process. The system incorporates a novel chronic care model in which traditional face to face (contact) visits are supplemented by automatic and on-demand virtual visits (9). During such virtual visits patients contact an intelligent agent (computer program) instead of a real doctor/nurse for assistance, guidance or advice. Such intelligent agents serve as a partner in intensive management utilising automated alerts, reminders, reports, advices or guides just-in-time coaches.
THE SYSTEM
The system is composed of three major units. The patient unit (PU) is able to acquire data and provide first-level advice to the patient. The patient unit also facilitates interaction with the health care centre, by automatically uploading data and receiving back any therapeutic plan supplied by the physician or the intelligent system. Portable wireless devices are used in automating data collection. On the patient”s side the mobile phone uses Bluetooth technology and therefore acts as a hub for a wireless network, possibly including several devices (e.g. balance, blood pressure monitor, step-counter, etc.) in addition to the glucometer.
The medical unit (MU) is available through the Health Care Centre (HCC) intranet and consists of a Web application integrating several functionalities, helping the physician in visualising and analysing patients” data, supporting his/her decision and therapy planning, and exchanging messages and/or therapeutic advice with his/her patients (10). The unit is fully integrated with a health care information system and is enhanced by guideline-based reminders and alerts. Furthermore, the MU is equipped with software accepting incoming point-to-point connections from PU and HCC units through standard modems for data, therapies, and messages exchange.
The third unit is the Health Care Centre unit, which receives patient data, hosts databases and runs various programs that organise visits, mediate between patients and care providers and offers different decision support functions. Here everything is monitored in a personal health record. The programs track measurements such as profile information, blood glucose, A1c history, behavioural assessments, vists, etc. This unit is responsible for selecting the appropriate form of feedback and visit including the organisation/scheduling of these visits. The power of HCC unit is that the right information goes to the right person at the right time and in the right format. The visit organiser decides when it is a good time to engage the team, and which team members to involve.
Figure 1 illustrates the architecture of the system, emphasising the communication paths between patient, care provider and HCC highlighting the main loops through which advice is conveyed. The mobile phone acts as the patient unit and hosts the front-end application, providing access to the whole system. Each time the patient uses the glucometer, this application automatically acquires new glycaemia readings using Bluetooth technology, stores data on the local diary, and performs a simple analysis, suggesting in real time the therapeutic actions (virtual visit). This interaction matches the small loop on the left side of the figure.
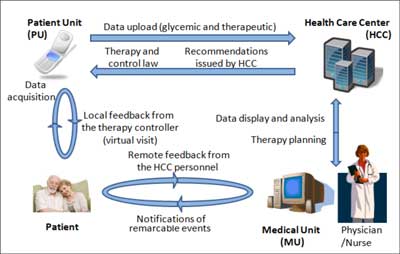
Fig. 1. Conceptual architecture of the telediabetology system.
The patient is then asked to revise those actions and acknowledge them so that they may be forwarded with the readings to the HCC where more comprehensive checks are performed and the caring physician may possibly review the whole case if needed. Whenever an exceptional event is noticed by the HCC unit, a text message is sent automatically to the mobile phone of the caring physician so that he/she is informed immediately.
Finally, whenever the physician perceives the need for a therapy change, he/she enters the new plan in the medical unit, which is later forwarded automatically to the patient”s unit, with any informational message the physician may have enclosed, as illustrated by the bigger loop shown in the bottom part of the figure.
Discussion
Telediabetology systems typically offer a suite of applications that streamline information flow in chronic disease management. A typical scenario involves the patient using a smart modem or mobile phone periodically to send his BGL measurements taken through a glucometer at home. Data are received and stored in a central database so that they can be analysed in order to detect metabolic alterations and automatically generate alarms. The physician is notified of data reception and analysis results so that he/she may use the visualisation and decision support tools integrated into the device for reviewing the patient”s metabolic condition. The physician may also modify the therapy of a patient, who will be notified automatically of any change.
The proposed system incorporates a novel chronic care model in which the traditional face to face (contact) visits are supplemented by automatic and on-demand virtual visits (9). We propose a new visit form called virtual visit. During such visits patients contact a computer program instead of a real doctor/nurse for assistance, guidance or advice in order to close the loop automatically and limit the personal patient-provider encounters to when they are absolutely needed. Patient self-management is supported by various resources and tools including customized patient education, reminders, advice and alarms along with persuasive techniques to activate patients. Sophisticated online analytics, trend analysis and other charting capabilities make review of patient data fast and easy. Alerts can be customized to include messaging for high/low readings, trend warnings, low testing frequency, and other parameters that are vital to improving personal care.
Conclusions
The proposed intelligent telediabetology system aims at offering a variety of telemonitoring and telecare services for insulin-treated diabetic patients 24 hours per day at the point and time where and when it is needed. Patients can contact intelligent computer programs instead of a real doctor/nurse for assistance, guidance or advice in order to limit the personal patient-provider encounters to scenarios in which they are really needed. The system also helps to prepare the person with diabetes for doctors” visits with a thorough checklist of items to bring, questions to ask the medical team, and what to expect at a check-up agents).
In addition to computer-assisted patient self management, health providers can also rely on different decision support services such as intelligent data analysis, context-sensitive information supply and consultation with a knowledge-based expert system in order to customize management protocols for the patients” individual needs.
We expect that the new architecture will improve efficiency, patient satisfaction and health outcomes. In additions, it will give patients assurance, information and support when human health providers are not available.
Piśmiennictwo
1. Roglic G, Green A, Sicree R, King H: Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004; 27(5): 1047-1053. 2. Sperl-Hillen J, O”Connor PJ, Carlson RR et al.: Improving diabetes care in a large health care system: an enhanced primary care approach. Jt Comm J Qual Improv 2000; 26(11): 615-622. 3. Klonoff DC: Diabetes and telemedicine: is the technology sound, effective, cost-effective, and practical. Diabetes Care 2003; 26(5): 1626-1628. 4. Farmer A, Gibson OJ, Tarassenko L, Neil A: A systematic review of telemedicine interventions to support blood glucose self-monitoring in diabetes. Diabet Med. 2005; 22(10): 1372-1378. 5. Ma C, Warren J, Phillips P, Stanek J: Empowering patients with essential information and communication support in the context of diabetes. Int J Med Inform 2006; 75(8): 577-596. 6. Jaana M, Paré G: Home telemonitoring of patients with diabetes: a systematic assessment of observed effects. J Eval Clin Pract 2007; 13(2): 242-253. 7. Lanzola G, Capozzi D, D”Annunzio G et al.: Going mobile with a multiaccess service for the management of diabetic patients. J Diabetes Sci Technol 2007; 1(5): 730-737. 8. Obstfelder A, Engeseth KH, Wynn R: Characteristics of successfully implemented telemedical applications. Implement Sci 2007; 2(1): 25. 9. Deutsch T, Gergely T: An intelligent partner system for improving chronic illness care. Informatics in Primary Care 2003; 11(1): 13-19. 10. Deutsch T, Gergely T, Trunov V: A computer system for interpreting blood glucose data. Computer Methods and Programs in Biomedicine 2004; 76(1): 41-51.
