© Borgis - New Medicine 3/2003, s. 57-60
Krzysztof Chizynski1, Jacek Kusmierek2, Ryszard Jaszewski1, Janusz Zaslonka1
Myocardial perfusion scintigraphy with thallium-201 in elderly patients after internal mammary artery revascularisation
1 Institute of Cardiology, Medical University, Lodz, Poland
Head: prof. Janusz Zaslonka, MD, PhD
2 Department of Nuclear Medicine, Medical University, Lodz, Poland
Head: prof. Jacek Kusmierek, MD, PhD
Summary
Introduction: The aim of the study was to investigate the problem of sufficient or insufficient myocardial perfusion during exercise in elderly patients after internal mammary artery (IMA) bypass, and to define the possible relationship between IMA flow and postoperative myocardial perfusion.
Material and methods: The study group was 81 patients aged 70-86 yrs. (mean 76 yrs.) who underwent IMA bypass surgery. IMA flow was measured during surgery in all patients (performed off bypass with no resistance), and thallium 201 perfusion scintigraphy was performed 3 months after bypass procedure.
Results: The IMA flow in our study was 40 to 200 ml/min (mean: 117). Good surgical results, defined as normal perfusion in both exercise and rest scintigrams, or very small perfusion defects in exercise scintigrams and normal perfusion in rest ones, were observed in 66 patients (81.5%). Thallium-201 perfusion scintigrams were analyzed separately in patients with IMA flow below 100 ml/min and over 100 ml/min. Good bypass results were observed in 53 patients (94.6%%) with IMA flow over 100 ml/min, but only in 13 patients (52%) with IMA flow below 100 ml/min (p <0.001). Poor surgical results were found in 12 patients (48%) with IMA flow below 100 ml/min, and only in 3 patients (5.4%) with IMA flow over 100 ml/min (p <0.001).
Conclusion: IMA flow measured intraoperatively has an important influence on coronary operation results in elderly patients. If we use IMA only in cases where the minimal flow is at least 100 ml/min, we could improve the outcome of coronary operations.
Introduction
The use of saphenous vein grafts in coronary artery bypass graft (CABG) surgery is the mainstay of surgical treatment of coronary artery disease. Saphenous vein graft failures are about 15 to 20% at 1 year, and at 5 years, about 65% of grafts remain patent. Five to ten percent of patients undergo repeat CABG surgery, most because of graft occlusion (1). The internal mammary artery (IMA) to the left anterior descending coronary artery (LAD) is now used as a conduit of choice. Despite several difficulties such as lower flow rates, longer operative time, and anatomical considerations, the IMA is superior graft material and can be recommended as a graft of choice mainly because of superior long-term patency. Based upon the low incidence of significant atherosclerosis in the IMA, it has been considered as a „protected vessel” (2, 3). In long-term study the results with IMA grafts are significantly better. IMA grafts are patent in 90% after 5 years and in 83% after 10 years. Not only the left IMA but also the right are used as a conduit (4,5). An IMA graft was used in only 57.7% of older patients compared with 97.1% in younger ones (6). An opinion exists that flow in an IMA anastomosed vessel during exercise may be insufficient. Flemma et al. (7) have reported that the flow in a saphenous vein bypass graft can be twice that in an IMA anastomosed to the same left descending artery, despite the use of an IMA 2 mm or more greater in diameter and flow rates of 100 ml per minute. Contrast angiography of native and graft circulations at rest does not demonstrate whether the flow in IMA anastomosed vessel in elderly patients is sufficient during exercise.
The aim of the study was to analyse the problem of sufficient or insufficient myocardial perfusion during exercise in elderly patients after IMA bypass, and to define the possible relationship between IMA flow and the post-operative myocardial perfusion as an outcome of a coronary operation.
Material and methods
The study group was 81 patients aged 70 to 86 yrs. (mean 76 yrs.), who underwent internal mammary artery bypass surgery. Most of the patients were operated on because of severe angina refractory to pharmacological therapy. They had no history of myocardial infarction, and no other heart diseases such as valvular heart disease or left ventricle hypertrophy. Patients with vasospastic angina were excluded from the study. There were 38 patients (47%) with unstable angina in the study group.
Preoperative study: Selective coronary angiography was carried out in all patients according to the Judkins technique. In 43 patients (53%) with stable angina the study protocol consisted of, the history of the angina, clinical examination, exercise test, and thallium-201 myocardial scintigraphy. In 38 patients (47%) with unstable angina the study protocol included only the history of the angina and a clinical examination.
Perioperative study: During surgery, IMA flow was measured in all patients (performed off bypass with no resistance) in the manner described by Hamby (8). Nitroglycerine was injected retrograde to the IMA to eliminate the possibility of a spasm.
Postoperative study: The study protocol included a clinical examination, exercise test, and thallium imaging.
Exercise thallium-201 imaging: After obtaining a baseline ECG and blood pressure, the patients were subjected to exercise with a bicycle ergometer starting at a workload of 25 W, increasing by 25 W increments every 3 minutes until the onset of limiting symptoms (chest pain, dyspnoea, or leg fatigue). The response to exercise was considered an indication of the presence of ischaemia if the ECG showed a ST segment depression equal to or greater than 1.5 mm when measured 0.08 seconds after the J point. Thallium-201 at a dose of 2 mCi was given intravenously at an exercise endpoint maintained for approximately one-and a-half to two minutes after tracer administration. After a 5-minute recovery period, acquisition was performed in subjects in a supine position using a GCA 401 TOSHIBA scintillation camera connected to a computer system. Three views of the myocardium were acquired: anterior, left anterior oblique (LA0) 45° and left lateral projection. Exposures with 200 000 counts in 5 min per image were acquired using a 20% window. In all patients delayed images in the same projections were repeated three hours later.
Thallium-201 image analysis: Exercise and rest thallium images were displayed, side-by-side, on a computer screen for interpretation. Two independent observers interpreted the thallium images without knowledge of the clinical history or graft surgery results. The left ventricle was divided into three segments in each of the three projections: the anterior view was divided into antero-lateral, apical, and infero-posterior segments, and the 45° left anterior oblique view was divided into septal, apico-inferior, and postero-lateral segments. The left lateral view was divided into anterior, apico-inferior, and posterior segments. Perfusion (thallium activity) was defined semi-quantitatively on a scale ranging from 0.0 (absent activity) to 2.0 (normal activity) with 0.5 increments. Scores estimated by the observers were averaged (9, 10).
Statistical analysis: The significance of differences between the frequencies of surgery results (scintigrams) and odds ratios (OR) were analysed with the use of a chi2 test with Yates´ correction. The odds ratio for good surgery results with a 95% confidence interval was calculated. Differences with p values of less than 0.05 were considered statistically significant (11).
Results
Internal mammary artery flow measured was 40 to 200 ml/min (mean flow: 117+ 29.7 ml/min). As shown in Fig. 1 IMA flow was below 80 ml/min only in 8 patients (10%), 80 to 100 ml/min in 17 patients (21%), 100 to 120 ml/min in 34 patients (42%), and over 120 ml/min in 22 patients (27%).
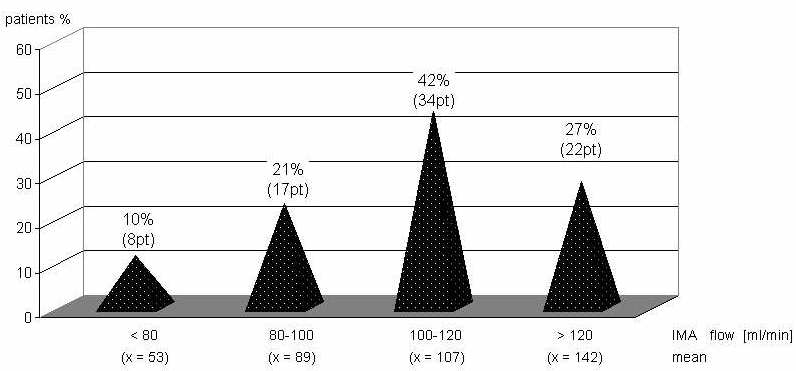
Fig. 1. Distribution of patients according to internal mammary flow values.
Exercise test results: In the preoperative study (43 patients with stable angina) the patients were exercised at a workload from 25 to 100 watts (mean 58.3 ± 18.7 watts). In 37 patients (86%) there was an ST segment depression equal to or exceeding 1.5 mm during exercise. In the postoperative study in this group the workload was 75 to 175 watts, mean load 131± 26.5 watts. It was significantly greater than before the operation (p <0,01). In the whole group (81 patients with and without preoperative stress tests), the patients were exercised at a workload from 75 to 175 watts, mean 123 ± 27.6 watts. In 5 patients (6.2%) there was an ST segment depression equal to or more than 1.5 mm during exercise. In other patients there were no signs of ischaemia in the ECG obtained during exercise.
Thallium-201 myocardial perfusion scintigraphy results: In preoperative scintigrams in all 43 patients there were serious perfusion defects after exercise and normal perfusion at rest. In this group perfusion scintigraphy identified critical LAD stenosis with a sensitivity of 94% and a specificity of 89%.
The postoperative scintigrams were divided into 4 categories: A – patients with normal perfusion in exercise and rest images, B – patients with small exercise-induced perfusion defects and normal perfusion at rest, C – patients with middle exercise-induced perfusion defects and normal perfusion in rest images, and D – patients with severe perfusion defects after exercise and in rest images. There were 35 patients (43%) with scintigrams in the A category, and they have very good perfusion and surgery results, and 31 patients (38%) with scintigrams in the B category who have good perfusion and surgery results. These results indicate that myocardial perfusion was good or sufficient, and the same the surgery, in 66 patients (81.5%). In 15 patients (18.5%) worse scintigraphy results (class C and D) were observed. These results indicate that insufficient myocardial perfusion was associated with a worse surgical outcome.
To answer the question whether myocardial perfusion in scintigraphy and the same surgical results depends on IMA flow we employed the following approach; thallium-201 myocardial perfusion scintigrams were analysed separately in patients with IMA flow to below 100 ml/min (56 patients) and over 100 ml/min (25 patients) (Fig. 2). Good bypass results (A and B category scintigrams) were observed in 53 patients (94.6%) with IMA flow over 100 ml/min, but only in 13 patients (52%) with IMA flow below 100 ml/min (p <0.001). Poor surgical results were seen in 12 patients (48%) with IMA flow below 100 ml/min, and only in 3 patients (5.4%) with IMA flow over 100 ml/min (p <0.001). The odds ratio for having good surgery results in patients with IMA flow over 100 ml per minute was 16.31 (95% CI, 4.83-55.02).
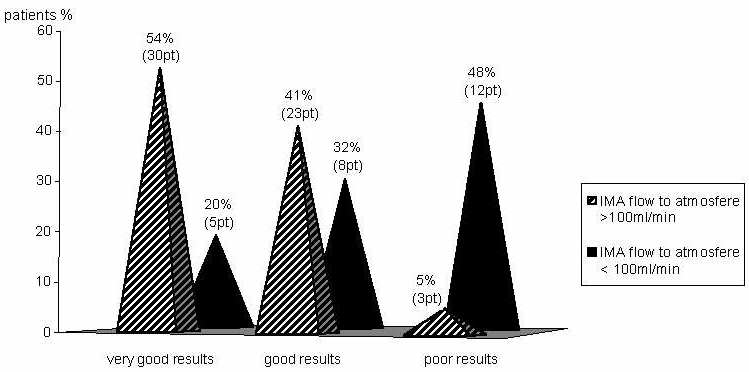
Fig. 2. Proportions of differentiated surgical outcome quality in patients subjected to IMA graft surgery under various conditions of IMA flow
Discussion
Internal mammary arteries have a peculiar resistance to atherogenic diathesis. Vein graft patency is now 88% in the early period, 81% at 1 year, 75% at 5 years, and 50% at 15 years (12). After a CABG operation the freedom rate from return of angina is 94%, 82%, 61% and 38% at 1, 5, 10 and 15 years (13,14). The operation results suggest that a patent-IMA to the left anterior descending coronary artery protects against recurrent angina and death from cardiac causes, and should be the conduit of choice (2). Now IMA grafts are used in 82% of patients; of these 97.2% have left IMA grafts (15).
For successful early bypass results the most important factor is adequate myocardial perfusion at rest and in exercise. A surgical bypass operation permits total revascularisation and an increased quality of life. The question of adequate flow has always prevailed the claim of increased patency when IMA is used (9, 10). To solve the problem of adequate perfusion after bypass (at rest and after exercise) studies measuring blood flow in the IMA after bypass, using DSA, transthoracic doppler ultrasonography, magnetic resonance, and transluminar doppler ultrasonography at rest and after dipyridamol (16, 17, 18) were performed. Accumulation of thallium 201 in viable cells mostly depends on coronary flow, and these observations were also confirmed in our study. Thallium 201 myocardial perfusion scintigraphy was used to measure postoperative perfusion. The minimum necessary IMA flow to render the IMA acceptable as a coronary conduit has been discussed as follows. In Hall´s et al. (19) study the IMA flow measured prior to bypass was 50 to 180 ml/min; mean 102 ml/min. In our studies IMA flow was 40 to 200 ml per minute (mean 117 ml/min). In our study, in 56 patients with an IMA flow of 100 ml/min or higher, good results were found in 53 patients (94.6%). In 25 patients with an IMA flow below 100 ml/min, good results were only found in 13 patients (52%). The bypass grafts were located in the same areas of the LAD (it is always possible that more distally-placed grafts used smaller – more distal parts of the internal mammary artery and therefore had lower flows) in two groups. In our study the IMA flow measured intraoperatively had an important influence on the coronary operation results.
Conclusion
IMA flow measured intraoperatively has an important influence on coronary operation results in elderly patients. If we use IMA only in cases where the minimal flow is at least 100 ml/min, we could improve the outcome of coronary operations.
Piśmiennictwo
kchizyn@poczta.onet.pl
