© Borgis - Postępy Nauk Medycznych 7/2016, s. 462-470
*Joanna Dangel
Foetal arrhythmia – what every obstetrician should know
Zaburzenia rytmu serca płodu – co każdy położnik wiedzieć powinien
Reference Prenatal Cardiology Centre, Ultrasound Clinic, The Warsaw Hospice for Children Foundation Head of Clinic: Professor Joanna Szymkiewicz-Dangel, MD, PhD
Perinatology and Perinatal Cardiology Clinic, 2nd Department of Obstetrics and Gynecology, Medical University of Warsaw
Head of Department: Professor Krzysztof Czajkowski, MD, PhD
Streszczenie
Zaburzenia rytmu serca są łatwe do zobaczenia, ale trudniejsze do precyzyjnego zdiagnozowania w okresie prenatalnym. Arytmie nie są wskazaniem do wcześniejszego zakończenia ciąży, płody powinny być monitorowane badaniem ultrasonograficznym, a nie kardiotokograficznym.
Arytmie dzielimy na: 1. Nieregularny rytm serca, czyli skurcze dodatkowe (80-85%): a) adkomorowe PAC (ang. premature atrial contractions), b) komorowe PVC (ang. premature ventricular contractions) – sporadycznie. 2. Tachyarytmie: a) tachykardia zatokowa (10-15%), b) częstoskurcz nadkomorowy, c) trzepotanie/migotanie przedsionków, d) częstoskurcz komorowy – niezmiernie rzadko. 3. Bradyarytmie (5-10%): a) bradykardia zatokowa – należy wykluczyć przyczyny położnicze, b) bradykardia spowodowana zablokowanymi skurczami dodatkowymi, c) rytm pozazatokowy – przedsionkowy, d) bloki przedsionkowo-komorowe.
Skurcze dodatkowe są najczęstszą, łagodną postacią arytmii. Zazwyczaj nie wymagają leczenia i ustępują w okresie okołoporodowym. Bigeminia przedsionkowa może imitować całkowity blok przedsionkowo-komorowy.
Płody z częstoskurczem nadkomorowym wymagają leczenia przezłożyskowego. Sposób leczenia uzależniony jest od rodzaju częstoskurczu, co może zdiagnozować kardiolog prenatalny. Konwersję do rytmu zatokowego można uzyskać w ponad 90% przypadków. Przedwczesne rozwiązanie ciąży bez konsultacji w ośrodku referencyjnym kardiologii prenatalnej powinno być uznane za błąd.
Całkowity blok przedsionkowo-komorowy bez wady strukturalnej jest chorobą nabytą wewnątrzmacicznie z powodu uszkodzenia układu bodźcowo-przewodzącego płodu najczęściej przez przeciwciała SS-A i SS-B. Pacjentki z dodatnimi przeciwciałami muszą być objęte specjalnym programem nadzoru kontroli czasu przewodzenia przedsionkowo-komorowego u płodów od 16. tygodnia w każdej ciąży. Płody z blokiem całkowitym powinny rodzić się w terminie porodu, gdyż wcześniactwo w sposób istotny pogarsza ich dalszy rozwój.
Całkowity blok przedsionkowo-komorowy z wadą serca i niewydolnością krążenia płodu jest wadą letalną.
Ścisła współpraca położniczo-kardiologiczna zapewnia optymalne wyniki leczenia w przypadkach arytmii u płodów.
Summary
Heart rhythm abnormalities are easy to visualise but more difficult to precisely diagnose in the prenatal period. Arrhythmia is not an indication for premature delivery, however, foetuses should be monitored using ultrasound, not cardiotocography.
Foetal arrhythmia is classified as follows: 1. Premature contractions (80-85%): a) premature atrial complexes PAC, b) premature ventricular complexes PVC – very rare. 2. Tachyarrhythmia: a) sinus tachycardia (10-15%), b) supraventricular tachycardia (SVT), c) atrial flutter/fibrillation, d) ventricular tachycardia – sporadic. 3. Bradyarrhythmia (5-10%): a) sinus bradycardia – obstetric causes should be excluded, b) blocked atrial contractions, c) non-sinus atrial rhythm, d) atrioventricular blocks.
Premature contractions are the most common and mild form of arrhythmia. In most cases, they do not require treatment and resolve spontaneously in the perinatal period. Atrial bigeminy can mimic a complete atrioventricular block. Foetuses with supraventricular tachycardia require transplacental treatment. The method of treatment will depend on the type of tachycardia, which can be diagnosed by a prenatal cardiologist. Conversion into the sinus rhythm can be achieved in more than 90% of cases. Premature delivery without consultation in the reference foetal cardiology center is a mistake. Complete heart block (CHB) without structural heart defect is an intrauterine acquired condition due to foetal electrical conduction system damage, most often caused by SS-A and SS-B antibodies. Women with positive antibodies should be included in a special surveillance program to monitor atrioventricular (AV) conduction time in foetuses from 16 weeks gestation. Foetuses with complete heart block should be born at term, as prematurity significantly affects their further development. Complete heart block with structural heart defect and foetal heart failure is a lethal disorder. Close cooperation between obstetrician and foetal cardiologists enables optimal treatment outcomes in foetuses and neonates with prenatally diagnosed arrhythmia.

INTRODUCTION
For many years, cardiotocography (CTG) has been a gold standard in foetal monitoring. A close cooperation between obstetricians and cardiologists has shown that CTG is not “a gold standard” for the assessment of foetal rhythm abnormalities or foetal condition during arrhythmia. CTG involves a simultaneous registration and graphical presentation of heart rate, uterine contractions and foetal movements. The results are presented graphically in the form of curves on a scale paper. In the case of foetal arrhythmia, CTG recordings show ‘averaged’ heart rhythm. This gives rise to completely incorrect readings in premature contractions, which do not pose a threat to foetal development and should not be an indication for premature delivery. The CTG recording is illegible for slow (below 60 bpm) or fast (> 200 bpm) heart rate (1). This information is very important as foetal arrhythmia diagnosis and foetal condition assessment are only possible based on ultrasonography and echocardiography.
Foetal rhythm disturbances are the second most common prenatal cardiovascular pathology. They occur in 1-3% of foetuses and are an indication for echocardiography in about 15% of cases in our centre. Foetal rhythm abnormalities are classified into three large groups: irregular heartbeat, tachycardia and bradycardia (2).
In 2004, The Polish National Registry for Foetal Cardiac Pathology (available at www.orpkp.pl) was launched. Since the programme is voluntary, it contains incomplete data. Table 1 shows the number of life-threatening foetal arrhythmias diagnosed and registered on www.orpkp.pl between 2004 and 2015.
Tab. 1. The most common type of foetal arrhythmia in Poland and in refernce center for fetal cardiology in Warsaw
| Type of arrhythmia | Poland | Warsaw Centre |
| Supraventricular tachycardia | 157 | 82 (52%) |
| Atrial flutter | 22 | 12 (55%) |
| Atrial fibrillation | 5 | 3 (60%) |
| Paroxysmal atrial tachycardia | 11 | 7 (64%) |
| Complete block | 95 | 55 (58%) |
DIAGNOSIS
An ultrasound examination allows for the diagnosis of foetal arrhythmia, while echocardiography determines its type.
The first step is to investigate whether the foetal heart rhythm is regular or not. Decreases in foetal heart rate, including a complete few-second arrest, which are a physiological phenomenon unrelated to pathology of the electrical conduction system, but to its immaturity, are often observed up to 25 weeks gestation. This is not an indication for echocardiography. Embrio heart rate should be assessed using M-mode ultrasound from the first trimester as decreased or increased heart rate may be the first symptom of foetal disease. Foetal heart rate in numbers is absolutely necessary between 11.0-13.6 weeks of gestation. Physicians using the FMF software need to enter the heart rate values in order to calculate the risk of chromosomal aberrations. Unfortunately, sometimes foetal heart rate of 140 is automatically entered into the report during the first trimester scanning, which is a considerable mistake as such slow heart rate is not normal in this period of foetal development as opposed to the later stages of pregnancy. Heart rate of 140 bpm is automatically entered in the first trimester ultrasound, which is abnormal in a healthy foetus as it indicates bradycardia. In the case of doubts about heart rate in the mid-pregnancy, the number of 140 bpm in the first trimester may indicate problems occurring already in this period and if not documented in an image, interpretation of this result is impossible.
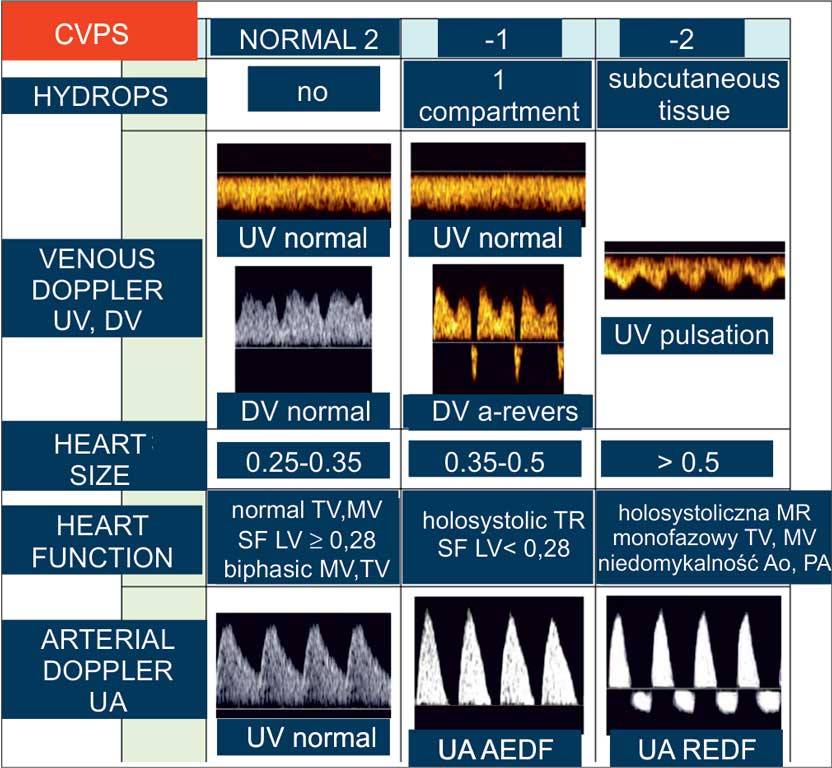
Foetal Cardiovascular Profile Score was introduced into prenatal cardiology by J. Huhta (fig. 1) (3). Using foetal ultrasound, Doppler and echocardiography, foetal cardiovascular system can be precisely evaluated. The scale allows foetal monitoring as well as prediction of neonatal condition. A newborn with prenatal score below 5 is known to have little chance of survival, especially if born prematurely. Implementation of appropriate transplacental therapy enables effective treatment.
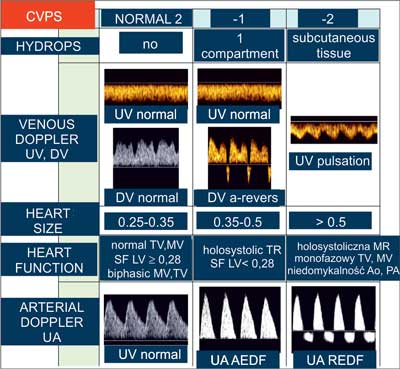
Fig. 1. Huhta’s cardiovascular scale. A healthy foetus is given a score of 10. One or two points are taken for every diagnosed abnormality – in accordance with the table
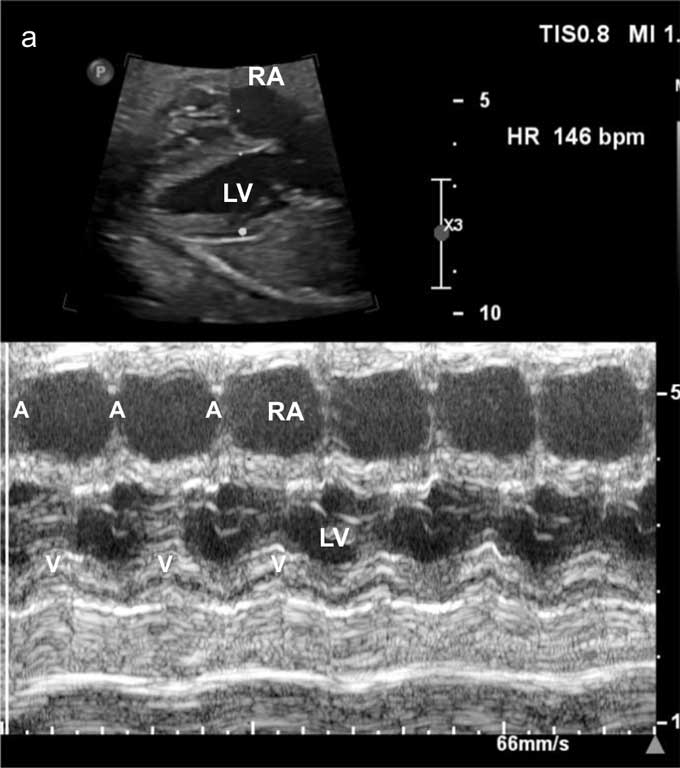
Since different ECG waves correspond to certain mechanical cardiac cycles, it is possible to identify the type of foetal rhythm disturbances. In M-mode with a four-chamber view, the rate of atrial and ventricular contractions should be calculated – under normal conditions each atrial contraction is followed by ventricular contraction and the heart rate is between 120 and 160 bpm (fig. 2a).

Fig. 2a. M-mode in a foetus with sinus rhythm of 146 bmp. A section through the right atrium (RA) and the left ventricle (LV)
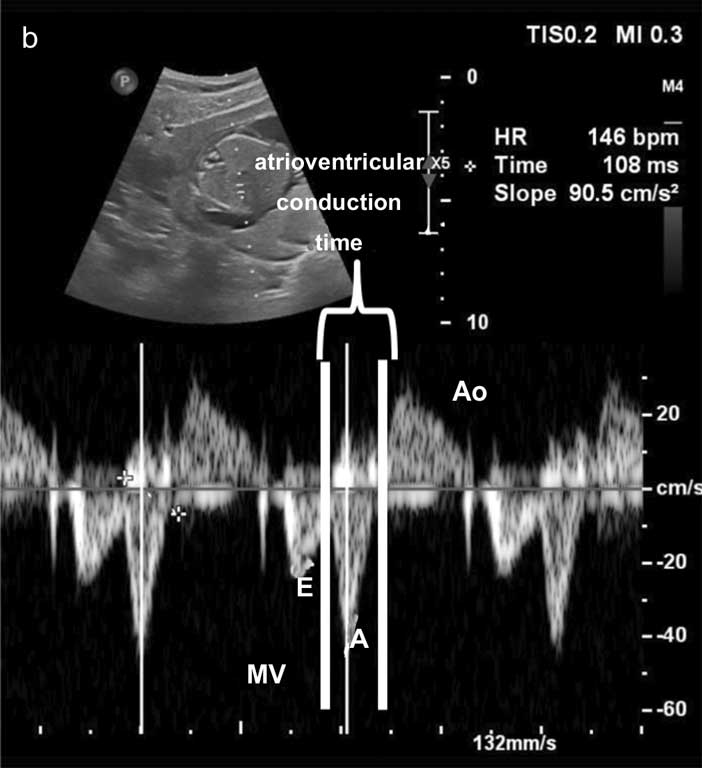
Doppler ultrasound evaluates the atrioventricular (AV) conduction time measured from A-wave (atrial contraction) of the mitral valve to aortic ejection. It corresponds to the “mechanical” PR interval on the ECG (fig. 2b) and is up to 150 ms in sinus rhythm.
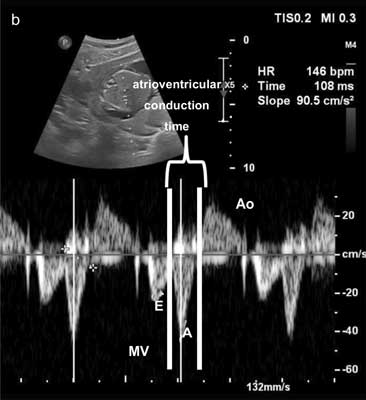
Fig. 2b. Doppler ultrasound – a gate inserted between the left ventricular inflow and outflow tracts, registering mitral valve (MV) and aortic (Ao) flow with atrioventricular (AV) conduction time measurement
CLASSIFICATION OF CARDIAC RHYTHM ABNORMALITIES
Foetal cardiac rhythm abnormalities:
1. Irregular heartbeat, i.e. premature contractions (80-85%):
a) premature atrial contractions,
b) premature ventricular contractions – sporadic.
2. Tachyarrhythmias:
a) sinus tachycardia (10-15%),
b) supraventricular tachycardia,
c) atrial flutter/fibrillation,
d) ventricular tachycardia – very rare.
3. Bradyarrhythmias (5-10%):
a) sinus bradycardia – obstetric causes should be excluded,
b) bradycardia secondary to blocked premature contractions,
c) non-sinus atrial rhythm,
d) atrioventricular blocks.
PREMATURE CONTRACTIONS
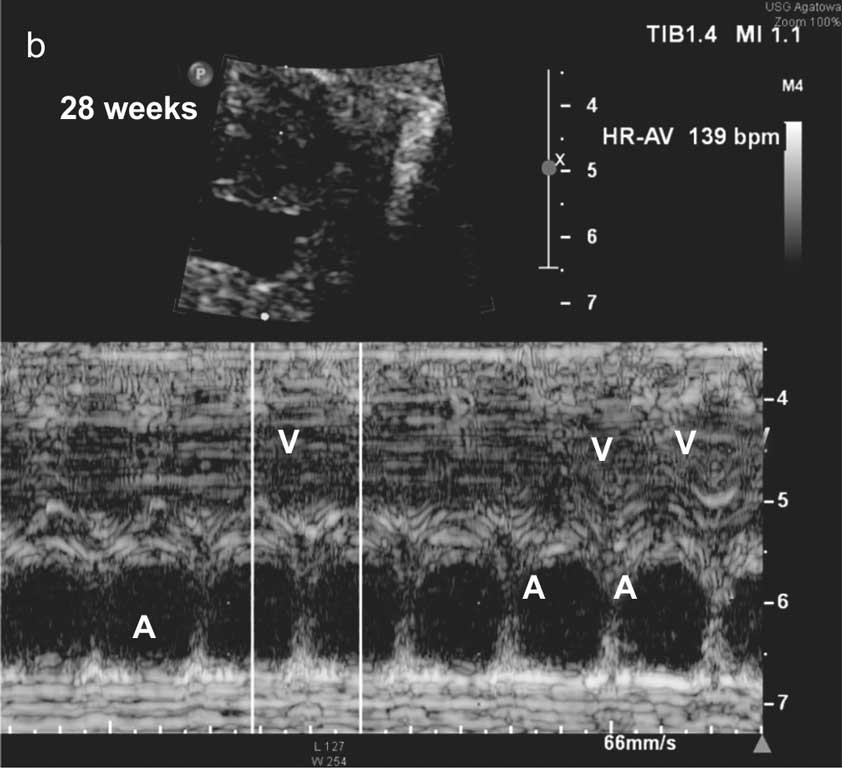
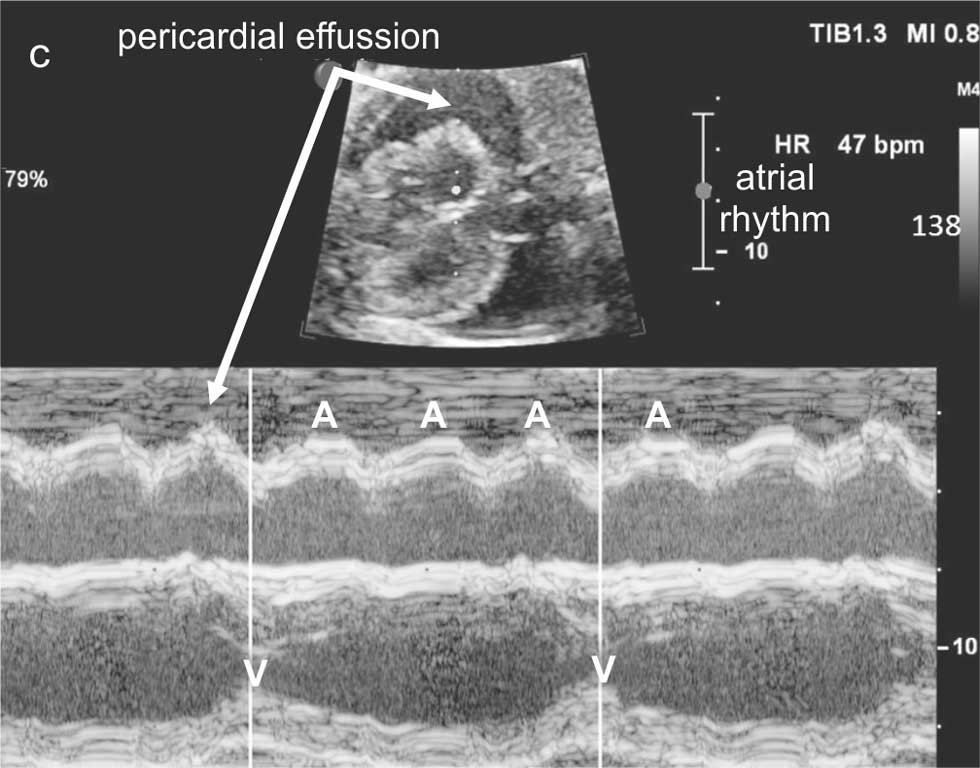
Premature contractions are a mild form of arrhythmia not requiring treatment. The long, floppy septum primum, which is called formen ovale aneurysm, hits the posterior wall of the left atrium during the cardiac cycle and is the mechanical cause of premature atrial contractions. Premature contractions may be conducted – when each premature contraction is followed by ventricular contraction, or non-conducted, when atrial contraction is not followed by ventricular contraction. Atrial bigeminy, when every other atrial contraction is blocked, results in a slow ventricular rhythm, usually about 70-90 bpm, is the greatest concern for an obstetrician. This type of foetal heart rhythm should be differentiated from a complete heart block (CHB). Blocked atrial contractions resolve spontaneously and do not require treatment (fig. 3a-3c). In contrary to CHB, atrial and ventricular contractions are quite regular, with blocked every other atrial contraction. In CHB, the atrial and ventricular rhythms are independent of one another.

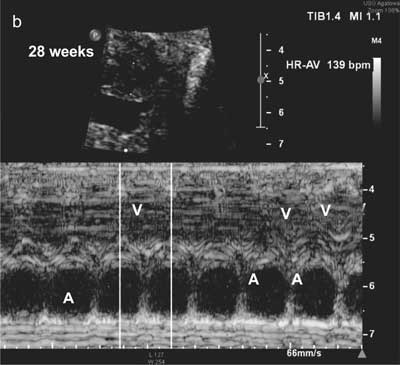
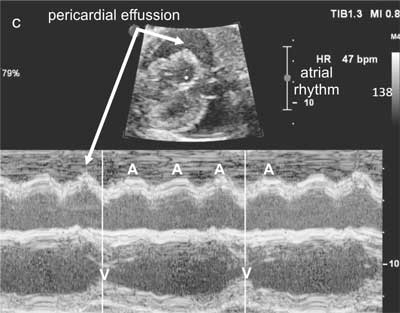
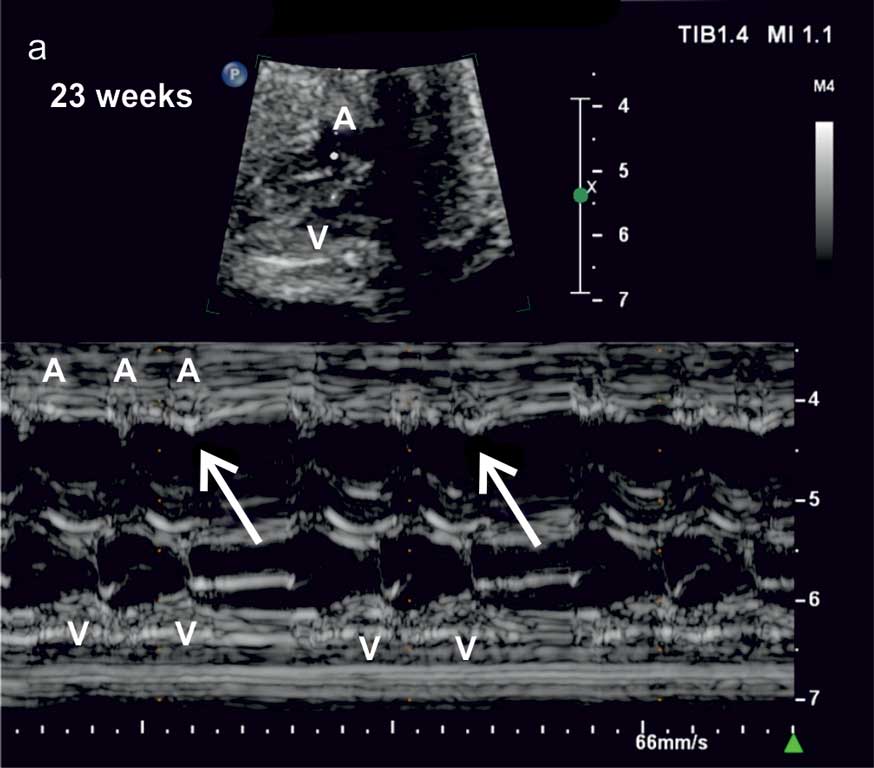
Fig. 3a-c. The use of M-mode in the diagnostics of rhythm and conduction disturbances:
a. M-mode in a foetus with blocked atrial premature contractions (bold arrows) causing foetal bradycardia of 80-90 bpm. A – atrial contractions, V – ventricular contractions
b. The same foetus at 28 weeks gestation; regular atrial and ventricular contractions, no treatment
c. A foetus at 29 weeks gestation with complete heart block and significant pericardial effussion indicating heart failure
In about 10-15% of cases premature atrial contarctions can cause more dangerous arrhyhmia, like supraventricular tachycardia. Isolated extrasystoles, even when multiple, do not require transplacental treatment or any other therapy. They are not an indication for premature delivery, but for transplacental treatment.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
Hamela-Olkowska A, Szymkiewicz-Dangel J, Romejko-Wolniewicz E et al.: Zapisy kardiotokograficzne u płodów z zaburzeniami rytmu serca – analiza przypadków. Ginekol Pol 2010; 81: 622-628.
Hamela-Olkowska A, Szymkiewicz-Dangel J: Zaburzenia rytmu serca i przewodzenia u płodów. [W:] Szymkiewicz-Dangel J (red.): Kardiologia płodu – zasady diagnostyki i terapii. OWN, Poznań 2007: 169-194.
Huhta JC: Fetal congestive heart failure. Semin Fetal Neonatal Med 2005 Dec; 10(6): 542-552.
Jaeggi ET, Carvalho JS, De Groot E et al.: Comparison of transplacental treatment of fetal supraventricular tachyarrhythmias with digoxin, flecainide, and sotalol: results of a nonrandomized multicenter study. Circulation 2011; 124(16): 1747-1754.
Eliasson H, Sonesson SE, Sharland G et al.: Fetal Working Group of the European Association of Pediatric Cardiology. Isolated atrioventricular block in the fetus: a retrospective, multinational, multicenter study of 175 patients. Circulation 2011; 124(18): 1919-1726.
Teliga-Czajkowska J, Czajkowski K, Majdan M: Rekomendacje postępowania położniczego oraz zasad współpracy reumatologiczno-położniczej u chorych na układowe choroby tkanki łącznej. Reumatologia 2014; 52(1): 38-48.
Fesslova V: The impact of treatment of the fetus by maternal therapy on the fetal and postnatal outcomes for fetuses diagnosed with isolated complete atrioventricular block. Cardiol Young 2009; 19: 282-290.