*Anna Mosiewicz1, Radosław Rola1, Barbara Mosiewicz-Madejska2, Robert Kaczmarczyk1, Tomasz Trojanowski1
Intramedullary cavernomas – an own experience and a review of the literature
Naczyniaki jamiste rdzenia kręgowego – doświadczenie własne i przegląd literatury
1Chair and Department of Neurosurgery and Paediatric Neurosurgery, Medical University in Lublin
Head of Department: Professor Tomasz Trojanowski, MD, PhD
2Chair and Department of Neurosurgery and Paediatric Neurosurgery, Students Medical Association, Medical University in Lublin
Protector of Association: Anna Mosiewicz, MD, PhD
Streszczenie
Wstęp. Naczyniaki jamiste są stosunkowo rzadkimi zmianami w centralnym układzie nerwowym. Jednakże ostatnio są one diagnozowane coraz częściej dzięki wprowadzeniu do diagnostyki rezonansu magnetycznego.
Cel pracy. Celem pracy była analiza przebiegu choroby u pacjentów leczonych w naszej Klinice oraz przegląd literatury na ten temat.
Materiał i metody. W ciągu ostatnich 10 lat w Klinice Neurochirurgii Uniwersytetu Medycznego w Lublinie było leczonych tylko 3 pacjentów z naczyniakiem jamistym rdzenia. Opisy tych przypadków stały się przyczynkiem do analizy opisywanych w literaturze objawów, obrazu klinicznego, procesu diagnostycznego i leczenia naczyniaków jamistych rdzenia.
Wyniki. Naczyniaki jamiste częściej występują w mózgu, w rdzeniu kręgowym są one zjawiskiem niezwykle rzadkim. Najczęstszą lokalizacją naczyniaków jamistych rdzenia jest jego odcinek piersiowy. Naczyniaki jamiste rdzenia są trudne do zdiagnozowania ze względu na ich rzadkie występowanie oraz mało charakterystyczny obraz kliniczny. Spektrum manifestacji klinicznych tej choroby rozciąga się od subtelnych objawów neurologicznych do gwałtownego wystąpienia ubytków czuciowych i ruchowych. Jednakże najczęstszym obrazem choroby jest powolna progresja ubytków neurologicznych związana z mikrokrwawieniami z naczyniaka.
Wnioski. Jedyną skuteczną metodą terapii i zapobiegania dalszemu postępowi deficytów neurologicznych jest leczenie chirurgiczne.
Summary
Introduction. Cavernous malformations constitute relatively rare vascular malformations of the centralnervous system (CNS). However, recently they are being diagnosed more often thanks to theintroduction of nuclear magnetic resonance.
Aim. The aim of this work was to analyse course of the disease of patients treated in our Department and to review literature on this subject.
Material and methods. Over the past ten years only three patients with spinal cavernomas were treated in the Department of Neurosurgery of the Medical University in Lublin. Following these cases we decided to review literature on symptomatology, clinicalcourse, diagnostics and treatment of intramedullary cavernomas.
Results. Being more prevalent in the brain, cavernomas hardly ever occur in the spinal cord. The most frequent location of cavernomas of the spinal cord is its thoracic part. Spinal cavernomas are difficult to diagnose due to their low incidence and nonspecific clinical course. Clinical manifestation of the disease varies from discrete neurological symptoms to rapid progression of motor and sensory deficits. However, the most common course of the disease is slow progression of neurological deficits due tomicrobleedings from the cavernoma.
Conclusions. The only effective way of treatment and prevention from further neurological deficits is surgery.

Introduction
Cavernous malformations are rare vascular malformations in the nervous system, mostly found in the hemispheric locations. Nonetheless, these malformations have been described within the cerebellum, cranial nerves, spinal roots, brain stem and spinal cord as well (1). It has been estimated that cavernous malformations constitute 5-12% of all vascular malformations within CNS (2, 3) and 3-5% of them are located in the spinal cord (3-5).
Pathogenesis of cavernomas remains unclear, however most of the existing theories suggest their developmental character (2, 4). Some imply that an angioblastic mesoderm dysplasia might occur during embryogenesis (2). Interestingly, they often coexist with developmental venous anomalies. It has been suggested that venous malformations play some role in the development of cavernous malformations.
Familiar occurrence as well as multiple localizations within the brain and spinal cord have been described (5-7). Candidate genes responsible for the development of cavernomas were identified in cases with familiar occurrence (4). Reports also exist on “de novo” generation of cavernomas following radiotherapy for other spinal lesions (8).
First case of intramedullary cavernoma was described by Hadlich in 1903 based on post mortem examination (9). Schultze performed the first successful surgery for intramedullary cavernoma in 1912 (9). Only 19 cases were described in the literature up to the mid-eighties of the last century (4, 9). It was most likely related to the efficacy of the available diagnostic tools i.e. myelography that had not been able to detect intramedullary lesions like small cavernous malformations. Spinal angiography had not been able to detect these lesions either. Detectability of cavernomas both, in the spine as well as in the brain (in particular those with previous hemorrhage) increased significantly with introduction of diagnostic MRI (4, 6, 9). Zevgaridis et al. (9) performed the largest to date analysis of 117 intramedullary cavernomas published in the literature between 1903 and 1996 and, based on their personal experience, described symptomatology, diagnosis and outcome of intramedullary cavernoma treatment.
Own series
1 SG
32-year-old male suffered from slow, progressive paraparesis of the lower extremities over a period of more than 12 years prior to the Department admission. Initially symptoms involved left, but subsequently involved right leg as well. He also reported transient difficulties with miction initiation that worsened over last few months prior to admission. Persistent neck pain, radiating to the left shoulder with concomitant numbness of the upper extremities was also reported. Paraparesis of the lower extremities, particularly the right one, has aggravated over the last year – patient was barely able to ambulate with elbow crouches.
Neurological examination revealed severe, spastic paraparesis of the lower extremities with clonic reflexes and bilaterally positive Babinski sign along with sensory deficits below Th6 level.
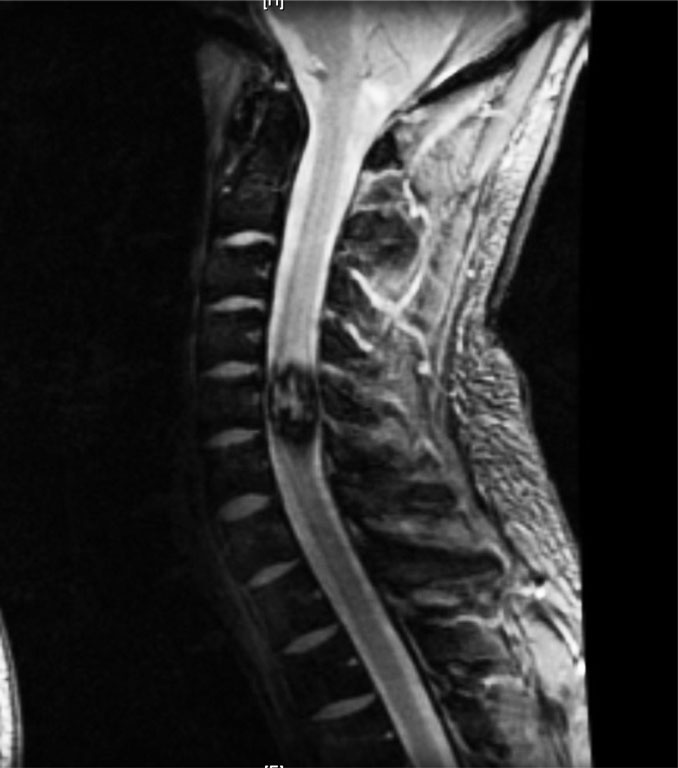
Spinal MRI revealed central, cervical disc herniation at C5/C6 level with reduction of the anterior buffer space with coexisting small, T2-hiperintensive lesion, possibly ischemic (fig. 1). Intramedullary, MRI revealed a T2-hiperintensive area approx. 17 x 9 mm in diameter that showed no contrast enhancement at the Th5 level. Similar smaller lesion was found at Th2 level (fig. 2).

Fig. 1. MRI of patient number one

Fig. 2. MRI of patient number one
Primarily, the patient underwent C5/C6 discectomy m. Smith-Robinson followed by an intervertebral, polycarbonate cage implantation. In result, neck and shoulders pain subsided along with urinary disturbances. Paraparesis of the lower extremities remained stable. Consequently, the patient underwent surgery three months later.
Initially Th5/Th6 laminectomy was performed; dural sack was incised in the middle.
Thick, yellowish spinal cord following midline incision 3-4 mm under the surface revealed red-gray lesion built of enlarged, tortuous veins. Cavernoma dissected from the surrounding relatively easily, yellowish tissue showed increased consistency when compared to normal spinal cord. A gross total resection was achieved. In the early postoperative period paraparesis transiently aggravated; it has returned to preoperative level within days. Patient required permanent bladder catheterization. Histopathology confirmed cavernoma weaving.
2 BT
27-year-old male presented with 3-month history of right shoulder pain and right, upper extremity numbness. On admission to the Department he showed mild, right-sided hemiparesis, more prominent in the upper extremity. Additionally, patient reported slight sensory deficit on the right. Neurological examination revealed significantly elevated patellar reflexes, predominantly on the right, bilateral foot clonus and bilaterally positive Babinski sign.
MRI examination revealed intramedullary lesion at C5 level (fig. 3). Subsequently, the patient underwent C5/C6 laminectomy; dural sack was incised in the middle.

Fig. 3. MRI of patient number two
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Ogilvy CS, Louis DN, Ojemann RG: Intramedullary cavernous angiomas of the spinal cord: clinical presentation, pathological features, and surgical management. Neurosurgery 1992; 31: 219-229.
2. El Mostarchid B, Lrhezzioui J, Akhddar A et al.: Intramedullary cavernous angioma. Two case-reports. Joint, Bone, Spine 2003; 70: 538-540.
3. Deutsch H, Jallo G, Faktorovich A, Epstein F: Spinal intramedullary cavernoma: clinical presentation and surgical outcome. J Neurosurg (Spine) 2000; 93: 65-70.
4. Lemole GM Jr, Henn JS, Riina HA et al.: Spinal cord cavernous malformations. Semin Cerebrovasc Dis Stroke 2002; 3: 227-235.
5. McCormick PC, Michelsen WJ, Post KD et al.: Cavernous malformations of the spinal cord. Neurosurgery 1988; 23: 459-463.
6. Krings T, Mull M, Gilsbach JM, Thorn A: Spinal vascular malformations. Eur Radiol 2005; 15: 267-278.
7. Vishteh AG, Zabramski JM, Spetzler RF: Patients with spinal cord cavernous malformations are at an increased risk for multiple neuraxis cavernous malformations. Neurosurgery 1999; 45: 30-32.
8. Maraire JN, Abdulrauf SI, Berger S et al.: De novo development of a cavernous malformation of the spinal cord following spinal axis radiation. Case report. J Neurosurg (Spine) 1999; 90: 234-238.
9. Zevgaridis D, Medele RJ, Hamburger C et al.: Cavernous haemangiomas of the spinal cord. A review of 117 cases. Acta Neurochir 1999; 141: 237-245.
10. Hsu F, Clatterbuck R, Kim L, Spetzler R: Intramedullary spinal cord cavernous malformations. Operat Tech Neurosurg 2003; 6: 32-40.
11. Cantore G, Delfini R, Cervoni L et al.: Intramedullary cavernous angiomas of the spinal cord: report of six cases. Surg Neurol 1995; 43: 448-451.
12. Zentner J, Hassler W, Gawehn J, Schroth G: Intramedullary cavernous angiomas. Surg Neurol 1989; 31: 64-68.
13. Canavero S, Pagni CA, Duca S, Bradac GB: Spinal intramedullary cavernous angiomas: a literature meta-analysis. Surg Neurol 1994; 41: 381-388.
14. Del Curling O Jr, Kelly DL Jr, Elster AD, Craven TE: An analysis of the natural history of cavernous angiomas. J Neurosurg 1991; 75: 702-708.