Agata Wasilewska, *Lidia Zawadzka-Głos
Retroauricular region involvement during otitis externa caused by P. aeruginosa
Odczyn na wyrostku sutkowatym w przebiegu zapalenia ucha zewnętrznego o etiologii P. aeruginosa
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Associate Professor Lidia Zawadzka-Głos, MD, PhD
Streszczenie
Wstęp. Rozlane zapalenie przewodu słuchowego zewnętrznego jest jedną z przyczyn bólu ucha, szczególnie dzieci w wieku szkolnym. Chorobie sprzyja uszkodzenie skóry w wyniku czyszczenia przewodu słuchowego, narażenia na wilgoć, czynniki anatomicznie oraz schorzenia dermatologiczne.
Cel pracy. Celem pracy było przedstawienie obrazu klinicznego, diagnostyki różnicowej i metod leczenia rozlanego zapalenia przewodu słuchowego zewnętrznego na podstawie przypadków pacjentów hospitalizowanych w Klinice Otolaryngologii Warszawskiego Uniwersytetu Medycznego.
Materiał i Metody. Dokonano retrospektywnej analizy obrazu klinicznego oraz wyników badań dodatkowych u 12 pacjentów z rozpoznanym rozlanego zapalenia ucha zewnętrznego hospitalizowanych w Klinice Otolaryngologii Dziecięcej Warszawskiego Uniwersytetu Medycznego okresie od 1 marca 2017 do 1 marca 2018.
Wyniki. Najczęstszym czynnikiem etiologicznym rozlanego zapalenia ucha środkowego był Pseudomonas aeruginosa. Ponad połowa pacjentów prezentowała odczyn okolicy zausznej w przebiegu zapalenia ucha zewnętrznego. U wszystkich pacjentów zastosowano antybiotykoterapię miejscową i dożylną.
Wnioski. Nietypowy przebieg związany z szerzeniem się stanu zapalnego na okolice zauszną sprzyja błędnemu rozpoznaniu zapalenia ucha zewnętrznego jako powikłania zapalenia ucha środkowego. Leczenie jest trudne ze względu na silne dolegliwości bólowe oraz oporność P. aeruginosa na większość antybiotyków.
Summary
Introduction. Diffuse otitis externa is one of the causes of ear pain, especially in school-age children. Risk factors for the disease include skin damage during cleaning audito
ry canal, moisture exposure, anatomical factors, and dermatological comorbidities.
Aim. The aim of the study was to present clinical picture, differential diagnosis and method of treatment of diffuse otitis externa based on cases of patients hospitalized in the Department of Pediatric Otolaryngology of the Medical University of Warsaw.
Material and Methods. A retrospective analysis of the clinical presentation and diagnostic tests of 12 cases of children with diffuse otitis externa hospitalized in the Department of Pediatric Otolaryngology of the Medical University of Warsaw from 1st March 2017 to 1st March 2018 was conducted.
Results. The most common etiological factor of diffuse otitis externa was Pseudomonas aeruginosa. Over half of the patients presented an involvement of retroauricular region during otitis externa. All the patients were treated with local and intravenous antibiotics.
Conclusions. Atypical course associated with the spread of inflammation to the retroauricular region may lead to an erroneous diagnosis of otitis externa as a complication of otitis media. Treatment is difficult due to severe pain and resistance of P. aeruginosa to most antibiotics.
Introduction
Diffuse otitis externa is one of the causes of ear pain, especially in school-age children (1-3). Risk factors of otitis externa include anatomical predisposition (narrow ear canal), immune disorders, diabetes, dermatological comorbidities, such as contact dermatitis and psoriasis, as well as foreign bodies in the auditory canal (1, 2, 4, 5). In addition, there are risk factors that are more specific to otitis externa, which include injuries during ear cleaning, humidity and skin maceration caused by long baths (1, 2, 4, 5).
The ear canal is a tube running from the external opening of the ear to the tympanic membrane (6). It consists of two parts: outer and inner. The outer, cartilaginous part is covered by thicker skin and contains multiple sebaceous and ceruminous glands, as well as hair follicles (6). In the inner, bone part, periosteum, richly supplied with nerve fibers, is directly covered by thin skin (6). For this reason, even a relatively benign inflammatory process in this region causes severe pain (6). The cerumen protects the skin against external factors, e.g. water, and ciliated epithelium transports secretions and dirt outside (6).
Superior to ear canal is the middle cranial fossa, anterior – temporomandibular joint and parotid gland, medial – tympanic membrane, posterior – mastoid process, inferior – base of skull and neck region (6). Potentially, complications of otitis externa may develop in these directions (4, 6).
Otitis externa is manifested by a sudden ear pain associated with pruritus and discomfort (1, 2, 4, 5). Discharge may also be present, which is perceived as wetness of the ear. The patient may also report tinnitus and decreased hearing (1, 2, 4, 5). Strong tenderness of the tragus is characteristic (1, 2, 4, 5). In otoscopy, congestion and edema of ear canal is observed, moreover, purulent discharge may be present (1, 2, 4, 5). Tympanic membrane may be normal, red or invisible due to edema (1, 2, 4, 5).
In otitis externa, inflammation easily passes to the surrounding tissues – parotid gland, skin, lymph nodes and auricular cartilage (1, 4-6). This may be manifested by protruding auricular cartilage and swelling of the retroauricular region. The clinical presentation may be similar to mastoiditis in the course of otitis media (4, 5).
Aim
The aim of the study was the analysis of cases of patients with diffuse otitis externa hospitalized in the Department of Pediatric Otolaryngology of the Medical University of Warsaw from 1st March 2017 to 1st March 2018.
Material and Methods
Clinical presentation and test results were analyzed retrospectively. All the patients were hospitalized and diagnosed with diffuse otitis externa. The patient treated in the out-patient clinic were not included in the study. Signs and symptoms, as well as results of ear canal swab culture, were analyzed.
Results
The study group included 12 patients with diffuse otitis externa aged 5 to 16 years. Mean age of the patients was 11.9 years. The largest number of hospitalizations occurred during summer (May-August) and autumn (September-November) – 5 patients each (41.5%). During the winter (December-February), 2 patients (16.8%) were hospitalized.
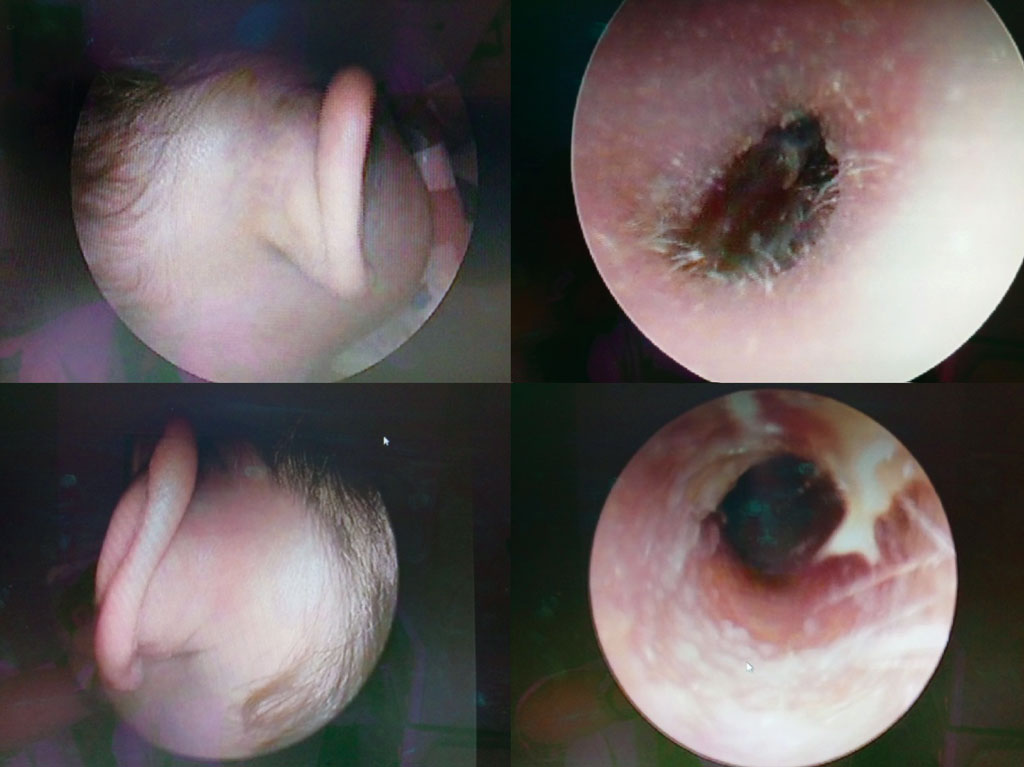
At admission, all the patients reported auricular pain and tenderness of the tragus. In 6 patients (58.3%), retroauricular and mastoid edema or protruding auricle have been observed. Signs and symptoms presented by the patients are shown in table 1. At admission, otoscopy revealed redness of the external auditory canal in all patients and swelling of the external auditory canal in 8 patients (67%). Figure 1 presents the otoscopic picture and a photograph of the retroauricular region of one of the patients.

Fig. 1. Otoscopic picture and a photograph of the retroauricular region of one of the patients
Tab. 1. Signs and symptoms presented by the patients
| Sign or symptom | Number of patients (%) |
| Fever | 2 (16.6%) |
| Elevated inflammatory markers | 7 (58.3%) |
| Auricular pain | 12 (100%) |
| Hearing impairment | 5 (41.7%) |
| Tenderness of the tragus | 12 (100%) |
| Redness of external auditory canal | 12 (100%) |
Edema of external auditory canal
Including edema preventing the assessment of the tympanic membrane | 8 (66%)
4 (33.3%) |
| Purulent discharge from the external auditory canal | 6 (50%) |
| Retroauricular and mastoid edema or protruding auricle | 7 (58.3%) |
In all the patients, medical management involved obtaining external auditory canal swab and culture before the beginning of treatment and cleaning the external auricular canal with suction and 3% boric acid irigation. After cleaning the external auditory canal, topical treatment with ofloxacillin drops three times a day was introduced. In patients with prominent external auditory canal swelling, an ear tampon soaked in ofloxacillin and dexametazone was introduced into the auditory canal for a few hours. In addition to topical treatment, all but one patient (91.3% of patients) received intravenous antibiotics due to: accompanying inflammation of surrounding tissues, poor outcomes of previously administered topical or oral antibiotics, suspected or confirmed P. aeruginosa infection or infection with another antibiotic-resistant microorganism, and/or a comorbidity predisposing to the complications of otitis externa (psoriasis in one patient).
All the patients were administered ceftazidime because of the suspected or confirmed Pseudomonas aeruginosa infection. In 10 patients out of 12, P. aeruginosa aetiology was confirmed (tab. 2). In 6 of these patients (60%), retroauricular edema was observed (tab. 3).
Tab. 2. Culture results
| Pathogen | Number of patients (%) |
| Pseudomonas aeruginosa | 9 (75%) |
| Pseudomonas aeruginosa and Enterococcus faecium | 1 (8.3%) |
| S. epide rmidis and C. albicans | 1 (8.3%) |
| Physiological skin flora (S. caprae, S.haemolyticus, Brevibacterium casei) | 1 (8.3%) |
Tab. 3. Correlation of P. aeruginosa infection with retroauricular involvement
| Patients with retroauricular involvement (n = 7) |
| Patients with P. aeruginosa infection (n = 6) | Patients with infection other than P. aeruginosa (n = 6) |
Discussion
Otitis externa can be classified as diffuse otitis externa, chronic otitis externa, ear canal furuncle, malignant otitis externa with skull osteomyelitis and facial nerve paresis, and eczematous otitis externa (1, 4, 5).
Diffuse otitis externa occurs commonly in pediatric patients. The highest incidence occurs in children aged 5 to 14 – 16% (1, 2) to 34% (3) of all cases are reported in this age group. Diffuse otitis externa occurs much less frequently in children under 4 years of age (1-3).
Diffuse otitis externa is caused almost exclusively by bacteria. The most common pathogen is Pseudomonas aeruginosa, which, according to the literature, is responsible for 33% (7) to 38% (8) of cases. In our material, Pseudomonas aeruginosa was responsible for 83.3% of cases. Antibiotic-resistant Staphylococcus epidermidis infection occurs less frequently and is responsible for 9.1% of cases (8), and methicyllin-sensitive Staphylococcus aureus (MRSA) is responsible for 7.8% (8) to 18% (7) of cases. In our material, 1 patient was infected with S. epidermidis and C. albicans. Anaerobic bacteria (Bacteroides, Peptostreptocci) are an etiological factor for otitis externa in 4 to 25% of patients (7, 8). Fungal infections are diagnosed in few percent of cases, usually after antibiotic therapy. Candida spp. is the most common pathogen causing fungal otitis externa (1, 2, 4, 5, 7, 8). It is worth noting that according to the literature, MRSA and anaerobic bacteria infection is associated with more severe signs and symptoms (9).
The clinical presentation of otitis externa may be similar to mastoiditis in the course of otitis media, due to retroauricular involvement and protruding auricle (4, 9, 10). Excluding this complication should be considered a priority, as it requires surgical management (4, 5). Differential diagnosis is made based on the clinical picture and laryngological examination, and, in unclear cases, based on the results of laboratory tests and imaging studies (4, 5, 9, 10).
Otitis externa is usually characterized by a sudden onset, and the symptoms are frequently preceded by an injury or exposure to water of the auditory canal (1, 2, 4, 5, 9, 10). Fever and subfebrile temperature occur rarely (1, 2, 4, 5, 9, 10). In otoscopy, auditory canal is swollen and reddened (1, 2, 4, 5, 9, 10). Tympanic membrane may be normal or reddened (1, 2, 4, 5, 9, 10). In mastoiditis, symptoms tend to appear gradually (4, 5, 9 10). Throbbing ear pain and fever may occur (4, 5, 9, 10). After a few days or week of the onset of the auricular pain, the symptoms worsen or recur, and tenderness and swelling of the mastoid process appear (4, 5, 9, 10). In otoscopy, tympanic membrane is reddened, bulging, and a pulsing, massive, purulent leak with tympanic membrane perforation may be present (4, 5, 9, 10). Auditory canal is not swollen, and the bulging of the superior-posterior wall of the canal may be visible. Conductive hearing loss is observed (4, 5, 9, 10).
Uncomplicated otitis externa is treated with topical antibiotic drops or antibiotic and steroid depending on the suspected aetiology. The empirical treatment should be active against P. aeruginosa and S. aureus. First-line topical treatment includes: ciprofloxacin combined with fluocinolone, ofloxacin, and combination of neomycin, polymyxin and hydrocortisone (1, 4, 5, 11). In addition, it seems beneficial to include acidifying ear drops (1, 4, 5, 11, 12), antiseptics, and topical corticosteroids (1, 4, 5, 11). In patients with severe clinical course, an ear tampon soaked in antibiotic and dexametazone should be introduced into the auditory canal (5, 11). Topical preparations including aminoglycosides are contraindicated in patients in whom tympanic membrane perforation cannot be excluded, such as post-traumatic patients and patients with ear tube drainage, due to the ototoxicity of this group of medications (1, 4, 11). Introduction of systemic antibiotic therapy does not improve clinical outcomes in uncomplicated, local otitis externa, and may result in unnecessary resistance development (11). If the inflammatory process is spreading to deeper tissues, systemic antibiotic therapy should be introduced (1, 4, 5, 11). In our patients, this also concerned patients with unsatisfactory response to previous local or systemic treatment, as well as patients infected with a resistant pathogen and suffering from comorbidities (psoriasis).
The group of antibiotic used for systemic treatment of complicated otitis externa with retroauricular involvement in adults is ciprofloxacin (1, 5). The safety of fluoroquinolones in children is debatable due to some reports of reversible arthropaties that occur after fluoroquinolone administration in children (13, 14). Therefore, this group of medications is reserved for life-threatening situations (13, 14). In children, third generation cephalosporins active against P. aeruginosa (e.g. ceftazidime) are administered intravenously as an alternative.
Conclusions
Diffuse otitis externa, also called “swimmer’s ear”, occurs commonly in children and adolescents. Despite its high incidence, diffuse otitis externa still constitutes a diagnostic and therapeutic challenge. Atypical course associated with the spread of inflammation to the retroauricular region may lead to an erroneous diagnosis of otitis externa as a complication of otitis media. Treatment is difficult due to severe pain and resistance of P. aeruginosa to most antibiotics.
Piśmiennictwo
1. Hassman-Poznańska E, Dzierżoniowska D, Poznańska M: Ostre rozlane zapalenie ucha zewnętrznego: Pol Prz Otolaryngol 2014; 3: 84-89.
2. Beers SL, Abramo TJ: Otitis externa review. Pediatr Emerg Care 2004; 20: 250-256.
3. Centers for Disease Control and Prevention (CDC): Estimated burden of acute otitis externa-United States, 2003-2007. MMWR Morb Mortal Wkly Rep 2011; 60(19): 605-660.
4. Chmielik M, Zawadzka-Głos L, Debska M, Zając B: Ucho. In: Chmielik M (ed.): Otolaryngologia dziecięca. 3rd ed., Dział Wydawnictw Akademii Medycznej w Warszawie. Warszawa 2004: 186-198.
5. Arcimowicz M, Balcerzak J, Bruzgielewicz A et al.: Schorzenia ucha zewnętrznego In: Janczewski G (ed.): Otorynolaryngologia praktyczna – tom I. 1st ed., Via Medica. Gdańsk 2005: 92-95.
6. Aleksandrowicz R, Ciszek B: Przestrzenie i trzewia głowy i szyi In: Aleksandrowicz R, Ciszek B: Anatomia Kliniczna Głowy i Szyi. Wydawnictwo Lekarskie PZWL. Warszawa 2007: 487-496.
7. Ghanpur AD, Nayak DR, Chawla K et al.: Comparison of Microbiological Flora in the External Auditory Canal of Normal Ear and an Ear with Acute Otitis Externa. J Clin Diagn Res 2017; 11(9): MC01-MC04.
8. Roland PS, Stroman DW: Microbiology of Acute Otitis Externa. Laryngoscope 2002; 112(7 Pt 1): 1166-1177.
9. Block SL: Mastoiditis mimicry: retro-auricular cellulitis related to otitis externa. Pediatr Ann 2014; 43(9): 342-347.
10. Hopkin RJ, Bergeson PS, Pinckard KC et al.: Otitis externa posing as mastoiditis. Arch Pediatr Adolesc Med 1994; 148(12): 1346-1349.
11. Rosenfeld RM, Schwartz SR, Cannon CR et al.: Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg 2014; 150(1 Suppl): S1-S24.
12. Kim JK, Cho JH: Change of external auditory canal pH in acute otitis externa. Ann Otol Rhinol Laryngol 2009; 118(11): 769-772.
13. Choi SH, Kim EY, Kim YJ: Systemic use of fluoroquinolone in children. Korean J Pediatr 2013; 56(5): 196-201.
14. Adefurin A, Sammons H, Jacqz-Aigrain E et al.: Ciprofloxacin safety in paediatrics: a systematic review. Arch Dis Child 2011; 96(9): 874-880.