*Elżbieta Niemczyk-Cieślak, Lidia Zawadzka-Głos
Otosclerosis
Otoskleroza
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Associate Professor Lidia Zawadzka-Głos, MD, PhD
Streszczenie
Otoskleroza jest pierwotnym schorzeniem dziedzicznym torebki ucha, dotykającym najczęściej obszar okienka owalnego. Umocowanie płytki strzemiączka powoduje unieruchomienie łańcucha kosteczek słuchowych, co prowadzi do postępującego przewodzeniowego ubytku słuchu. Inne objawy obejmują czuciowo-nerwowy komponent utraty słuchu, szum w uszach i objawy przedsionkowe. Kliniczna otoskleroza występuje częściej u kobiet, a pierwsze objawy pojawiają się zwykle po porodzie w trzeciej dekadzie życia. Etiologia obejmuje czynniki genetyczne, infekcyjne, zapalne, autoimmunologiczne i hormonalne. Diagnostyka audiologiczna otosklerozy obejmuje zestaw uzupełniających się testów, a wzajemne powiązanie ich wyników ma wysoką wartość predykcyjną. Istnieje kilka klasyfikacji choroby, z których większość opiera się na kryteriach radiologicznych. Badania obrazowe obejmują głównie tomografię komputerową kości skroniowej o wysokiej rozdzielczości, która ma stosunkowo wysoką czułość i swoistość w wykrywaniu ognisk otosklerotycznych. Pomimo dostępności szerokiej gamy technik diagnostycznych, ostateczna diagnoza jest nadal potwierdzana śródoperacyjnie. Stapedotomia pozostaje rozsądną pierwotną interwencją dla większości pacjentów z otosklerozą.
Summary
Otosclerosis is a primary hereditary disorder of the otic capsule, affecting most commonly the area of the oval window. Stapes footplate fixation results in the immobility of the ossicular chain, which leads to progressive conductive hearing loss. Other symptoms include a sensorinerural component of hearing loss, tinnitus, and vestibular symptoms. Clinical otosclerosis occurs more frequently in women, and the first symptoms usually appear after childbirth in the 3rd decade of life. The etiology includes genetic, infectious, inflammatory, autoimmune, and hormonal factors. Audiological diagnostics for otosclerosis involves a battery of tests that complement one another, and the interrelation of their outcomes has a high predictive value. There are a few classifications of the disease, the majority of which are based on radiological criteria. Imaging studies mainly involve temporal bone high-resolution computed tomography, which has a relatively high sensitivity and specificity for detecting otosclerotic foci. Despite the availability of a wide variety of diagnostic techniques, the final diagnosis is still confirmed intraoperatively. Stapedotomy remains a reasonable primary intervention for the majority of patients with otosclerosis.
Introduction
Antonio Maria Valsalva, a Bologna-born surgeon and anatomist, described footplate fixation for the first time in 1735. J. Toynbee discovered a hereditary predisposition for this condition over than a century later and postulated that prolonged inflammation of the lining of the tympanic cavity would result in ankylosis of the footplate and progressing hearing loss. A. von Tröltsch used the term otosclerosis in 1869 to describe the disease’s last, dormant stage. In 1873, H. Schwartze noted the occurrence of a blood-stained promontory lining via the thin, atrophic eardrum. A. Politzer examined 16 temporal bones with stapes fixation in the late 1800s and concluded that it was the consequence of a disorder involving the entire otic capsule. In the early 1900s, F. Siebenmann proposed the term otospongiosis to describe the presence of bony regions with a spongy structure that Schwartze noticed during the disease’s active phase (1-4).
Epidemiology
In 90% of patients, the first symptoms appear between 15 and 45 years of age (most commonly in the 3rd decade). They occur less frequently in the pediatric population and in elderly (3, 5).
Clinical otosclerosis (lesion that fixes the footplate of stapes) occurs more frequently in women than men (1.8-3:1). It is observed in 0.1-2.1% (0.3-1%) of Caucasians, in whom it occurs about 10 times more often than in Africans and Asians. In contrast, the prevalence of the histologic otosclerosis (without fixing the stapes footplate) among Caucasians is estimated to be 8.3-13%, almost equally common among men and women (7:6) (1, 3, 6, 7).
Otosclerosis affects 70-85% of both ears, and the severity of the hearing loss is usually asymmetrical and more pronounced on the side where symptoms first appear. This pattern is more common in women. Unilateral hearing loss is relatively more common in men (3).
Location of lesions
Otosclerosis affects the periosteal, endochondral, and endosteal layers of the otic capsule. The most common location is anterior to the oval window, referred to as the fissula ante fenestram (which accounts for approximately 80-96% of lesions), followed by the region of the round window (30-36%), the fissula post fenestram (11-28%), the periaqueductal region (21%), and the internal auditory canal region 19%) (1, 6, 8-10).
Much less frequently, the disease process may affect other parts of the inner ear, such as the semicircular canals, the area of the VIII nerve’s, and the area of the endolymphatic duct. The term cochlear otosclerosis is used when the bony capsule of the cochlea is affected exclusively (6, 10).
Histopathology
The process of ossification of the otic capsule is completed by the end of the first year of life. From this point on, bone remodeling is limited in the healthy individual, and the number of osteoblasts and osteoclasts in the inner ear bone capsule is negligible. Otosclerotic bone undergoes a remodeling process in which normal bone is replaced by otosclerotic bone. The endochondral layer is the starting point for otosclerotic lesions. It is represented by globuli interossei which indicates small regions of immature connective tissue (1, 6, 11).
Otosclerotic lesions are classified as cellular (spongiotic), fibrotic, and sclerotic. The cellular type is characterized by the recruitment and activation of monocytes, macrophages, osteoblasts, and osteoclasts; the fibrotic type is characterized by extensive bone fibrosis; and the sclerotic type is characterized by a paucity of bone cells. The otosclerotic and otospongiotic lesions can occur simultaneously, with neither necessarily preceding the other (12, 13). Criteria of histological activity in an otosclerotic focus are shown in table 1.
Tab. 1. Criteria of histological activity in an otosclerotic focus according to Schuknecht and Barber (14)
| 1. areas of non-osseous tissue showing increased cellularity |
| 2. evidence of osteoclastic bone resorption and/or osteoblastic new bone formation |
| 3. increased vascularity and fibrous thickening of overlying mucosa |
| 4. affinity of the osseous tissue for acidophilic stains |
Etiology
Otosclerosis is a multifactorial condition. The etiology takes includes genetic, infectious, inflammatory, autoimmune, and hormonal factors:
1. Genetic factors – otosclerosis is inherited autosomally dominantly, with 20-40% penetrance (1, 6, 8). Half of all cases of this disease are considered to be sporadic. So far, nine familially occurring monogenic loci associated with the disease have been identified (OSTC1, OTSC2, OTSC3, OTSC4, OTSC5, OTSC7, OTSC8, OTSC10). TGFß1 family genes (BMP2, BMP4), renin-angiotensin system (ACE, AGT) genes, central nervous system development genes (RELN), collagen type I (COL1A1, COL1A2) genes, and HLA system genes may play a role in the development of otosclerosis (1, 7, 8, 15-17).
2. Infectious factors – in otosclerotic foci, filamentous structures resembling measles virus nucleocapsids were discovered, as was its RNA in the stapes footplate. In addition, the expression of IgG and IgA antibodies in the intrachondral ossification area of otosclerotic subjects was demonstrated. After the introduction of universal measles vaccination in the German population, a decline in the incidence of otosclerosis was observed. In addition, the measles and rubella viruses within otosclerotic foci has been identified (1, 6, 9, 18, 19).
3. Inflammatory and autoimmune factors – the etiology of otosclerosis may involve autoimmune reactions against osteoprotegerin and various types of collagen (including II and IX) (1, 6, 20).
4. Hormonal factors – the role of sex hormones in the development of otosclerosis is undisputed. Estrogens have an effect on the RANK (receptor activator of nuclear kappa-ß) system, resulting in a decreased osteoclast response to the RANK ligand complex, which induces apoptosis. In addition, prolactin, whose level rises under the influence of estrogen and progesterone, inhibits the action of osteoprotegerin, resulting in an increase in osteolysis and calcium imbalance. This explains why some women experience an increase in disease symptoms during pregnancy and when using oral contraceptives (6).
Clinical manifestation
The typical otosclerosis patient is a woman between the ages of 20 and 30 with a positive family history and a progressive, asymmetric bilateral hearing loss that began or worsened after childbirth.
The patient’s medical history plays an important role in making a correct diagnosis. An estimated two-thirds of patients have a family history of hearing impairment. The disease is initially asymptomatic. Patients notice hearing loss at a threshold of 25-30 dB HL and report bilateral or, less frequently, unilateral progressive hearing loss over the years. The disease’s progression may occur during pregnancy, breastfeeding, and while taking estrogen-containing medications. Eighty percent of patients have conductive hearing loss, and air-bone gap (ABG) does not exceed 50-60 dB HL. In 15% of cases, otosclerotic lesions also affect the cochlea, resulting in a mixed hearing loss. Five percent of patients suffer from isolated cochlear otosclerosis (1, 6, 10).
Sixty percent of patients suffer from tinnitus (75% of women and 56% of men). Occasionally, it precedes hearing loss by several month or years. Tinnitus can manifest as a constant buzzing, whooshing, or even hissing. It may be persistent, chronic, and proportional to the sensory impairment or the degree of the conductive hearing loss (1). If the otic capsule in vestibular region is affected by a disease process, dizziness and balance disturbances may occur (1). Otosclerosis may contribute to the development of the superior semicircular canal dehiscence. The incidence of objectively confirmed vestibular impairment is estimated to be 7-50% (25-47%) of cases (20, 21).
At the time of taking a patient’s medical history, quiet speech is noted. In cases of conductive hearing loss, patients report better hearing in noise (paracusis Willisi). An increase in intensity, pitch structure voice for enhanced audibility in noisy environments is known as the Lombard effect. It is an involuntary response speakers experience in the presence of noise during voice communication. Moreover, the sensorineural component of hearing loss results in impaired speech comprehension in noise.
On otoscopic examination, no abnormalities are detected. In some patients, the tympanic membrane and skin of an ear canal are thin, and there is reduced production of cerumen. In some cases the Schwartze sign is present (1, 6, 10).
Diagnosis
When otosclerosis is suspected, audiologic, otoneurologic, and imaging tests are administered. Nevertheless, the definitive diagnosis is still made at the time of surgery by manual assessment of ossicular chain mobility (1, 10).
Audiological diagnostics for otosclerosis involves a battery of tests that complement one another, and the interrelation of their outcomes has a high predictive value (22).
Due to the frequent occurrence of bilateral hearing loss, the Weber test is of limited utility. In unilateral disease with mixed or conductive hearing loss, Weber test lateralizes to that ear. In ears with conductive hearing loss for ABG exceeding 20 dB HL at 512 Hz and 25 dB HL at 1024 Hz, the Rinne test will be negative. There are additional tests of historical significance that are not implemented in the present diagnostic process of otosclerosis. The Gellè test (pathological in typical otosclerosis), the Schwabach test (extended in typical otosclerosis), the Bing test (negative in typical otosclerosis), and the Miodoński test (positive in typical otosclerosis) (1, 23).
Pure tone audiometry and speech audiometry are also a part of diagnostic process. In the initial stages of the disease, an ABG is observed. As a result of fixation of the footplate of stapes and reduction of ossicular chain resonance, Carhart’s notch (an increase of bone conduction threshold by 10-20 dB, most pronounced at 2000 Hz) may occur. More advanced forms of otosclerosis are characterized by a reduction of ABG and an increase of the bone conduction threshold, particularly at higher frequencies. The presence of moderate-to-severe sensorineural hearing loss is relatively common in isolated cochlear otosclerosis. Speech audiometry is not routinely administered to otosclerosis patients (1, 6, 10, 21, 22).
Impedance audiometry and wideband acoustic immitance measurements (including wideband tympanometry) are useful components of diagnosis of otosclerotic ears. The average compensated admittance (compliance) of the group of all otosclerotic ears decreases. A large dispersion in the admittance values is associated with a substantial number of the overlap with normal values (24, 25). Type A tympanograms are typical, while type As tympanograms are less common (26, 27). Otosclerotic ears are characterized by an absence of ipsilateral acoustic (stapedial) reflexes. Due to the stiffening of the auditory ossicular chain, the resonant frequency of the middle ear increases significantly and reach values between 1055 Hz and 1262 Hz (27-29). In wideband tympanometry, the absorbance decreases at frequencies below 1000 Hz (26, 30, 31). The test has a high sensitivity for detecting otosclerosis (82%) but a low specificity (17.2% of results are false positive) (26). Due to the overlap of results with normal values, wideband tympanometry is not currently the sufficient diagnostic technique for detecting otosclerosis (26, 32, 33).
Otoneurological diagnosis focuses on a small group of patients suffering from vertigo. Electronystagmography/videonystagmography, caloric testing, vHIT (video head impulse test), rotatory chair testing, cervical and ocular myogenic vestibular evoked potentials (cVEMP and oVEMP) are included (1, 22).
Imaging studies mainly involve temporal bone high-resolution computed tomography imaging (HRCT). HRCT scans of the temporal bones have a relatively high sensitivity (45-94%) and specificity (42-100%) for detecting otosclerotic foci (34-44). According to estimates, the likelihood of detecting lesions is determined by their size (> 0.4-0.6 mm in diameter) and density that differs from that of the surrounding healthy bone (39, 41). Active (otospongiotic) lesions are therefore more susceptible to radiological evaluation than inactive (otosclerotic) lesions (6). Despite its high sensitivity and specificity, HRCT examination of the temporal bones is insufficient to make a definitive diagnosis in patients suspected of having otosclerosis (37).
Other tests which may be helpful in making a diagnosis of cochlear otosclerosis are: magnetic resonance scans, densitometry, PET/CT (18-F Sodium Fluoride) may be useful in the diagnosis of cochlear otosclerosis (1, 45-47).
Differential diagnosis
Otosclerosis must be distinguished from: tympanosclerosis, congenital ankylosis of the stapes, attic fixation of head of the malleus, discontinuity of the ossicular chain, isolated superior semicircular canal dehiscence, osteogenesis imperfecta (van der Hoeve and de Kleyn disease), Paget’s disease, congenital cholesteatoma, limited fibrous dysplasia, and syphilis of the inner ear (1, 6, 10, 45, 48-50).
Otosclerosis classification
The majority of otosclerosis classifications are based on radiological criteria. Veillon et al. (51) proposed a classification system for otosclerotic foci based on its advancement and location in relation to oval window (tab. 2).
Tab. 2. Criteria for radiologic advancement of otosclerosis (51)
| Grade |
| 1 | A | Foci restricted to the footplate of stapes; footplate in relation to otic capsule: hypodense, thickened (greater than 0.6 mm), and irregular |
| B | Hypodense lesion < 1 mm, anterior to the oval window at the level of the fissula antre fenestram, with or without footplate involvement |
| 2 | | Hypodense lesion > 1 mm, anterior to the oval window, without endosteum involvement, with or without footplate involvement |
| 3 | | Hypodense lesion > 1 mm, anterior to the oval window, with endosteum involvement, with or without footplate involvement |
| 4 | A | Extensive hypodense foci located in the middle layer of the otic capsule, laterally, medially, and anterior to the cochlea |
| B | Extensve hypodense foci around the semicircular canals, affecting the medial wall of the vestibule |
The aforementioned classification correlates with the air conduction threshold in otosclerotic ears. In addition, the early-stage types have an average ABG of 24.3 dB (SD = 10 dB) whereas advanced forms of otosclerosis are associated with an ABG of 32.7 dB (SD = 12.0 dB). Isolated otosclerosis of the round window is rare (10.8-13%), but may affect the degree of ABG closure after surgery (52-55).
Mansour et al. (54) proposed a classification of isolated round window otosclerosis based on HRCT scans of the temporal bones (tab. 3).
Tab. 3. Classification of isolated round window otosclerosis (54)
| Grade | Prevalence | Radiological criteria | Average (SD) ABG | Effects on hearing after surgery |
| RW-I | 17.1% | Isolated round window edge hypodensities | 30.7 (5.3) dB | No effect |
| RW-II | 31.7% | Partial thickening of the round window membrane | 32.7 (3.9) dB | No effect |
| RW-III | 34.7% | Global thickening of the round window membrane, but still a persistent air-filled recess that permits delineation | 38.2 (6.4) dB | Increased bone and air conduction thresholds, postoperative ABG 15 dB |
| RW-IV | 34.1% | A totally filled round window recess that obliterates access to the membrane | 41.4 (4.8) dB | High bone and air conduction thresholds, postoperative ABG 30 dB |
| Cochlear otosclerosis with the round window involvement RW-V | Overgrowing otosclerotic foci in far-advanced otosclerosis largely covering the round window recess aperture and possibly involving the cochlea |
This classification corresponds to bone and air conduction thresholds as well as the efficacy of surgical treatment. The key point is the obliteration in the region of the round window membrane, which disrupts the mechanoacoustic properties of the inner ear by stiffening it. The RW-I and RW-II stages have no effect on audiological parameters or surgical outcomes. Grade RW-III results in elevated bone and air conduction thresholds and a small ABG. Grade RW-IV denotes significant hearing loss and surgical failure (54).
Malafronte et al. (56) classified otosclerosis according to the intraoperative appearance of the stapes footplate:
– degree I: blue footplate – the most common (71.8%); the otosclerotic process from the oval window rim involves only anterior (94.5%) or posterior (4%) or both (1.35% of patients),
– degree II: white footplate – occurs in 21.4% of cases; the otosclerotic process from the oval window rim involves most of the footplate (diffuse otosclerosis) in 77.2% of patients, or the focus arises in the middle of footplate involving the entire footplate with a well-delimitated rim (biscuit-type footplate) in 22.8 of patients,
– degree III: obliterative otosclerosis (nonvisible footplate) – the rarest (6.8%), massive otospongiotic focus completely covers the footplate.
The classification is very useful in informing the surgeon, before making any maneuvers on the stapes regarding the different degrees of difficulty of surgery.
Management and treatment
The treatment of otosclerosis includes observation, stapes surgery, hearing aids device installation and cochlear implantation. There are currently no effective pharmaceutical treatments (1, 6, 10).
The primary objective of pharmaceutical treatments is to stop the progression of disease associated with active phase of the disease (bone remodeling around the oval window and otic capsule). Pharmacotherapy should be administered independently from other treatment methods (6). Vestibular disorders and progressive mixed and sensorineural hearing loss are indications for its use. Long-term sodium fluoride therapy inhibits resorbing enzymes and induces otospongiotic bone to transform into otosclerotic bone. It is estimated that 50% of patients will experience disease stabilization as a consequence (49). It is believed that bisphosphonates (sodium alendronate), which are commonly used to treat osteoporosis, could be effective in the treatment of otosclerosis because they inhibit osteoclast activity noticeably (6).
Wait and see policy should be considered in an otosclerosis involving one ear or in the early stages of bilateral otosclerosis (6, 10). It is the treatment of choice for patients with bilateral otosclerosis when surgery is contraindicated.
Surgical treatment of otosclerosis includes stapes surgery, bone anchored hearing system devices (BAHA), middle ear implants, and cochlear implants. Stapes surgery is the treatment of choice for otosclerosis and will be discussed later. Bone anchored hearing system devices alternative to stapes surgery because of the negligible risk of sensorineural hearing loss. This solution may work well in the case of otosclerosis if the only hearing ear is affected (6). Middle ear implants, such as the Med-El™ Vibrant Soundbridge, interacts with the round window to enhance acoustic stimulation in patients who are disqualified from a cochlear implantation and are no longer beneficial from hearing aids or stapedotomies (6, 41). The Cochlear™ CODACS™ is an implant combined with a passive prosthesis commonly used in stapedotomy procedures and designed for patients with severe or profound mixed hearing loss at an advanced stage of disease (57). For advanced forms of bilateral cochlear otosclerosis accompanied by bilateral profound sensorineural hearing loss and incipient cochlear ossification, cochlear implants should be considered (6).
Stapes surgery
Stapes surgery is a treatment dedicated for otosclerosis located in the oval window region. It does not prevent the disease’s progression. The primary objective is to reduce the ABG to below 10 dB HL. Improvements in hearing are observed in 90-95% of cases. Thirty four percent of surgical patients report tinnitus reduction (1, 6).
Depending on the author, indications for stapes surgery include bilateral ABG exceeding 15-20-25 dB at frequencies in the speech range of 500 to 4,000 Hz. In unilateral otosclerosis, a 30 dB increase in the air threshold curve is associated with a speech discrimination of less than 80 percent. Patients should consider hearing aids prior to surgery. There are no age restrictions for this type of surgery (1, 6, 10, 58).
An absolute contraindications to stapes surgery includes active infection of the external or middle ear. The relative contraindications are as follows: otosclerosis in the only hearing ear, poor general condition of the patient, and socioeconomic factors such as piloting, diving, working at high altitude (6, 58).
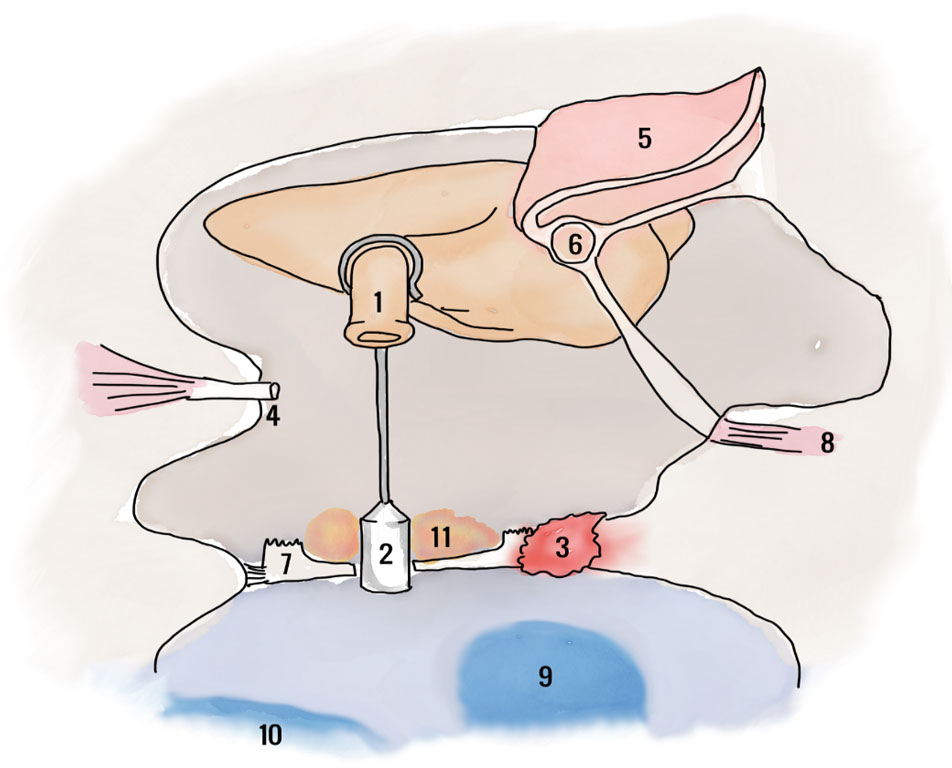
Stapes procedures can be performed under general or local anesthesia. Stapedectomy involves removal of the entire stapes with its footplate which is replaced with a prosthesis after covering the oval window with a venous graft or temporal muscle fascia. Partial stapedectomy is a technique with removal of 25% of the footplate plate with subsequent sealing of the prosthesis piston area with connective tissue (1, 10, 59). Stapedotomy is a stapes suprastructure removal, creation of a small hole in the footplate, the diameter of which matches the prosthesis piston (fig. 1). The hole can be made with a perforator, drill or CO2 laser. Stapedotomy provides better hearing improvement at higher frequencies (10, 58). Multiple modifications of stapedotomy have been developed. One of them is Fisch reverse stapedotomy with preservation of the stapes suprastructure and stapedial tendon. When necrosis of the long process of the incus is present (at the time of revision surgery), malleovestibulopexy is performed (6, 10). Anatomical conditions that may cause intraoperative complications or alter the procedure’s course include: dehiscence and overhang of the facial nerve over the oval window, complete obliteration of the round window, malleus fixation, persistent stapedial artery, and biscuit-type footoplate.

Fig. 1. Anatomical constellations of the middle ear following stapedotomy. The figure shows a prosthesis attached the long process of the incus. The piston is inserted into the inner ear and sealed with connective tissue to stabilize it in the footplate opening. 1 – long process of incus; 2 – piston; 3 – otosclerotic focus; 4 – stapedial tendon; 5 – derutated tympanic membrane; 6 – handle of malleus; 7 – footplate of stapes (without its suprastructure); 8 – tensor tympani muscle; 9 – urticle; 10 – sacculus; 11 – connective tissue sealing the area of the prosthesis piston
Stapes surgery may be performed as a one-day surgery. Then, it is necessary to ensure that the patient can contact the ENT department in case of alarming symptoms. After approximately 7 days, the dressing in external auditory canal and skin sutures are removed. A follow-up audiometric examination should be performed after 4 to 6 weeks (6). Stapedotomy and stapedectomy procedures carry the risk of intraoperative complications, early and late (tab. 4).
Tab. 4. Stapes surgery complications (1, 6, 10, 60-62)
| The complication | Remarks |
| Intraoperative complications |
| Tympanic membrane perforation | Should be managed with the temporalis muscle fascia |
| Chorda tympani injury | Unilateral ageusia resolves spontaneously up to 6 months postoperatively |
| Facial nerve injury | 10% of healthy individuals have natural dehiscence of the facial nerve in the tympanic cavity, which increases the risk of nerve injury, especially at the time of revision surgery. Immediate decompression of the nerve is required |
| Bleeding | Should be controlled with electrocoagulation and intra- or postoperative administration of haemostatic drugs; the risk increases in the presence of vascular anomalies such as dehiscence of the juguar bulb or persistent stapedial artery |
| Gusher | A high-pressure flow of the perylimph immediately after opening of the footplate – a rare phenomenon occurring relatively often in patients with radiological evidence of vestibular aqueduct dilatation or internal auditory canal anomalies. The phenomenon carries a significant risk of postoperative deafness. Immediate head elevation and fistula sealing with a connective tissue supported by a prosthesis is recommended. Lumbar puncture may be considered |
| Biscuit-type footplate | The footplate should be removed |
| Aspiration of perylimph | It is critical to avoid suctioning the vestibule. Perilymph aspiration carries a significant risk of postoperative deafness; fluid loss can be supplemented with Ringer’s solution |
| Mechanical or acoustic injury of the inner ear | Systemic corticosteroid therapy should be administered |
| Early complications |
| Permanent deafness | 1% (primary surgery) to 4% (revision surgery) |
| Sensorineural hearing loss | A control hole created prior to proper surgery reduces a risk of postoperative sensorineural hearing loss |
| Transient dizziness and balance disorders | In 12 to 45% of cases, they are caused by the close relation of the prosthesis to the saccule and utricle. They can be followed by a spontaneous or positional nystagmus. The symptoms are caused by irritation of the labyrinth and resolve spontaneously several hours/days after surgery; a hearing test is recommended. If symptoms persist for an extended period of time, a perilymphatic fistula or excessively long prosthesis should be suspected |
| Increase in tinnitus | 5% of patients experience an increase in tinnitus, which may be related to a perilymphatic fistula or the inner ear damage |
| Delayed facial nerve paresis | |
| Granuloma | Occurs 2 to 6 weeks after surgery, commonly as a response to foreign bodies – fatty tissue, hemostatic dressings; causes progressive hearing loss; occasionally causes pain of the ear, increased tinnitus, and vertigo. Otoscopy reveals a gray-red granuloma, usually in the upper posterior quadrant. Steroid therapy, antibiotic therapy, or surgical revision with removal of inflammatory tissues may be considered |
| Perilymphatic fistula | Results from insufficient inner ear sealing; causes hearing loss, balance disorders, and ABG enlargement. Reconstruction and sealing of the oval window is suggested. Perilymphatic fistula raises the risk of labyrynthitis and meningitis |
| Late complications |
| Perilymphatic fistula | Discussed in early complications |
| Hyperacusis | The transection of the stapedial tendon causes hypersensitivity to loud sounds in 40% of operated patients; stapedotomy techniques with preservation or reconstruction of the stapedial tendon do not provide significant benefits |
| Granuloma | Discussed in early complications |
| Dislocation of the prosthesis | The ABG of up to 60 dB appears as a consequence of prosthesis piston dislocation in the oval window or necrosis of the long process of incus |
| Adhesive otitis media | Conductive hearing loss appears a few weeks after surgery; reoperation is recommended, hearing improvement is uncertain |
| Progressive sensorineural hearing loss | An increase in bone conduction threshold by 1dB every two years (5.5 dB in ten years), associated with disease progression and/or cochlear aging |
| Acquired endolymphatic hydrops | A result of postoperative trauma |
Conclusions
Otosclerosis is an otic capsule disorder. A number of audiological and otoneurological symptoms is strongly associated with the location of otosclerotic lesions. Different forms of otosclerotic foci in the region of the oval window indicate the type and course of surgery. In the majority of cases, the preferred treatment is stapedotomy, which improves hearing in nearly all patients. It should be remembered that surgical treatment does not stop the progression of the disease, and the progressive sensorineural hearing loss should be anticipated.
Piśmiennictwo
1. Chodynicki S, Olszewska E: Otoskleroza. [W:] Śliwińska-Kowalska M (red.): Audiologia kliniczna. MEDITON, Łódź 2005: 237-252.
2. Nazarian R, McElveen JT Jr, Eshraghi AA: History of Otosclerosis and Stapes Surgery. Otolaryngol Clin North Am 2018; 51(2): 275-290.
3. Crompton M, Cadge BA, Ziff JL et al.: The Epidemiology of Otosclerosis in a British Cohort. Otol Neurotol 2019; 40(1): 22-30.
4. Morawski K, Lachowska M: Otoskleroza. [W:] Niemczyk K (red.): Wykłady z otolaryngologii. Medipage, Warszawa 2012: 178-181.
5. Vincent R, Wegner I, Vonck BM et al.: Primary stapedotomy in children with otosclerosis: A prospective study of 41 consecutive cases. Laryngoscope 2016; 126(2): 442-446.
6. Baring D, Swan I: Otosclerosis. [In:] Hussain SM (ed.): Logan Turner’s Diseases of the nose, throat and ear: Head and neck surgery. 11 ed. Boca Raton: Taylor & Francis Group 2016: 433-441.
7. Chen W, Campbell CA, Green GE et al.: Linkage of otosclerosis to a third locus (OTSC3) on human chromosome 6p21.3-22.3. J Med Genet 2002; 39(7): 473-477.
8. Rudic M, Keogh I, Wagner R et al.: The pathophysiology of otosclerosis: Review of current research. Hear Res 2015; 330(Pt A): 51-56.
9. Arnold W: Some remarks on the histopathology of otosclerosis. Adv Otorhinolaryngol 2007; 65: 25-30.
10. Niemczyk K: Otoskleroza. [W:] Janczewski G (red.): Otorynolaryngologia praktyczna. 1. Via Medica, Gdańsk 2005: 169-174.
11. Wang PC, Merchant SN, McKenna MJ et al.: Does otosclerosis occur only in the temporal bone? Am J Otol 1999; 20(2): 162-165.
12. Lim DJ, Robinson M, Saunders WH: Morphologic and immunohistochemical observation of otosclerotic stapes: a preliminary study. Am J Otolaryngol 1987; 8(5): 282-295.
13. Parahy C, Linthicum FH Jr: Otosclerosis and otospongiosis: clinical and histological comparisons. Laryngoscope 1984; 94(4): 508-512.
14. Schuknecht HF, Barber W: Histologic variants in otosclerosis. Laryngoscope 1985; 95(11): 1307-1317.
15. Schrauwen I, Ealy M, Fransen E et al.: Genetic variants in the RELN gene are associated with otosclerosis in multiple European populations. Hum Genet 2010; 127(2): 155-162.
16. Schrauwen I, Van Camp G: The etiology of otosclerosis: a combination of genes and environment. Laryngoscope 2010; 120(6): 1195-1202.
17. Thys M, Schrauwen I, Vanderstraeten K et al.: Detection of rare nonsynonymous variants in TGFB1 in otosclerosis patients. Ann Hum Genet 2009; 73(2): 171-175.
18. Potocka-Baklazec M, Sakowicz-Burkiewicz M, Kuczkowski J et al.: Expression of TNF-alpha, OPG, IL-1beta and the presence of the measles virus RNA in the stapes of the patients with otosclerosis. Eur Arch Otorhinolaryngol 2015; 272(8): 1907-1912.
19. Arnold W, Friedmann I: Otosclerosis – an inflammatory disease of the otic capsule of viral aetiology? J Laryngol Otol 1988; 102(10): 865-871.
20. Brookler KH: Electronystagmography in a patient with recent disequilibrium and a family history of otosclerosis. Ear Nose Throat J 2002; 81(11): 762.
21. Freeman J: Otosclerosis and vestibular dysfunction. Laryngoscope 1980; 90(9): 1481-1487.
22. Danesh AA, Shahnaz N, Hall JW 3rd: The Audiology of Otosclerosis. Otolaryngol Clin North Am 2018; 51(2): 327-342.
23. Gryczyński M, Pajor A: Badanie akumetryczne i próby stroikowe. [W:] Śliwińska-Kowalska M (red.): Audiologia kliniczna. MEDITON, Łódź 2005: 107-112.
24. Shahnaz N, Polka L: Standard and multifrequency tympanometry in normal and otosclerotic ears. Ear Hear 1997; 18(4): 326-341.
25. Keefe DH, Archer KL, Schmid KK et al.: Identifying Otosclerosis with Aural Acoustical Tests of Absorbance, Group Delay, Acoustic Reflex Threshold, and Otoacoustic Emissions. J Am Acad Audiol 2017; 28(9): 838-860.
26. Shahnaz N, Bork K, Polka L et al.: Energy reflectance and tympanometry in normal and otosclerotic ears. Ear Hear 2009; 30(2): 219-233.
27. Niemczyk E, Lachowska M, Tataj E et al.: Wideband tympanometry and absorbance measurements in otosclerotic ears. Laryngoscope 2019; 129(10): E365-E376.
28. Valvik BR, Johnsen M, Laukli E: Multifrequency tympanometry. Preliminary experiences with a commercially available middle-ear analyzer. Audiology 1994; 33(5): 245-253.
29. Miani C, Bergamin AM, Barotti A, Isola M: Multifrequency multicomponent tympanometry in normal and otosclerotic ears. Scand Audiol 2000; 29(4): 225-237.
30. Allen JB, Jeng PS, Levitt H: Evaluation of human middle ear function via an acoustic power assessment. J Rehabil Res Dev 2005; 42(4 Suppl 2): 63-78.
31. Nakajima HH, Pisano DV, Roosli C et al.: Comparison of ear-canal reflectance and umbo velocity in patients with conductive hearing loss: a preliminary study. Ear Hear 2012; 33(1): 35-43.
32. Nakajima HH, Rosowski JJ, Shahnaz N, Voss SE: Assessment of ear disorders using power reflectance. Ear Hear 2013; 34 Suppl 1: 48S-53S.
33. Niemczyk E, Lachowska M, Niemczyk K: Tympanometria szerokopasmowa – nowa metoda oceny ucha środkowego. Polski Przegląd Otorynolaryngologiczny 2016; 5: 65-74.
34. Lagleyre S, Sorrentino T, Calmels MN et al.: Reliability of high-resolution CT scan in diagnosis of otosclerosis. Otol Neurotol 2009; 30(8): 1152-1159.
35. Naumann IC, Porcellini B, Fisch U: Otosclerosis: incidence of positive findings on high-resolution computed tomography and their correlation to audiological test data. Ann Otol Rhinol Laryngol 2005; 114(9): 709-716.
36. Purohit B, Hermans R, Op de Beeck K: Imaging in otosclerosis: A pictorial review. Insights Imaging 2014; 5(2): 245-252.
37. Wegner I, van Waes AM, Bittermann AJ et al.: A Systematic Review of the Diagnostic Value of CT Imaging in Diagnosing Otosclerosis. Otol Neurotol 2016; 37(1): 9-15.
38. Shin YJ, Deguine O, Cognard C et al.: [Reliability of CT scan in the diagnosis of conductive hearing loss with normal tympanic membrane]. Rev Laryngol Otol Rhinol (Bord) 2001; 122(2): 81-84.
39. Liktor B, Revesz P, Csomor P et al.: Diagnostic value of cone-beam CT in histologically confirmed otosclerosis. Eur Arch Otorhinolaryngol 2014; 271(8): 2131-2138.
40. Kiyomizu K, Tono T, Yang D et al.: Correlation of CT analysis and audiometry in Japanese otosclerosis. Auris Nasus Larynx 2004; 31(2): 125-129.
41. Karosi T, Csomor P, Sziklai I: The value of HRCT in stapes fixations corresponding to hearing thresholds and histologic findings. Otol Neurotol 2012; 33(8): 1300-1307.
42. Marx M, Lagleyre S, Escude B et al.: Correlations between CT scan findings and hearing thresholds in otosclerosis. Acta Otolaryngol 2011; 131(4): 351-357.
43. Trojanowska A, Trojanowski P, Olszanski W et al.: How to reliably evaluate middle ear diseases? Comparison of different methods of post-processing based on multislice computed tomography examination. Acta Otolaryngol 2007; 127(3): 258-264.
44. Tringali S, Pouget JF, Bertholon P et al.: Value of temporal bone density measurements in otosclerosis patients with normal-appearing computed tomographic scan. Ann Otol Rhinol Laryngol 2007; 116(3): 195-198.
45. Waterval JJ, Vallinga M, Brans B et al.: 18F-fluoride PET/CT scan for quantification of bone metabolism in the inner ear in patients with otosclerosis--a pilot study. Clin Nucl Med 2013; 38(9): 677-685.
46. Saunders JE, Derebery MJ, Lo WW: Magnetic resonance imaging of cochlear otosclerosis. Ann Otol Rhinol Laryngol 1995; 104(10 Pt 1): 826-829.
47. Stimmer H, Arnold W, Schwaiger M, Laubenbacher C: Magnetic resonance imaging and high-resolution computed tomography in the otospongiotic phase of otosclerosis. ORL J Otorhinolaryngol Relat Spec 2002; 64(6): 451-453.
48. Arain Z, Abbas Y, Adams A: Pediatric otosyphilis – an unusual cause of conductive hearing loss. Radiol Case Rep 2020; 15(1): 65-70.
49. Behrbohm H, Kaschke O, Nawka T, Swift A: Choroby niezapalne otoczki błędnika. [W:] Behrbohm H, Kaschke O, Nawka T, Swift A (red.): Choroby ucha, nosa i gardła z chirurgią głowy i szyi. Edra Urban & Partner, Wrocław 2011: 83-85.
50. Molher J, Pujol EMD, Zounon ADS et al.: Middle Ear Osteoma Causing Mixed Hearing Loss: A Case Report. J Int Adv Otol 2018; 14(3): 493-496.
51. Veillon F, Riehm S, Emachescu B et al.: Imaging of the windows of the temporal bone. Semin Ultrasound CT MR 2001; 22(3): 271-280.
52. Meranger A, David A, Beigner BM et al.: Audiometric Results of Stapedotomy Surgery for Otoscelorsis: Influence of the Radiological Stage. Otol Neurotol 2019; 40(2): e75-e81.
53. Nadol JB Jr: Histopathology of residual and recurrent conductive hearing loss after stapedectomy. Otol Neurotol 2001; 22(2): 162-169.
54. Mansour S, Nicolas K, Ahmad HH: Round window otosclerosis: radiologic classification and clinical correlations. Otol Neurotol 2011; 32(3): 384-392.
55. Wiet RJ, Harvey SA, Bauer GP: Complications in stapes surgery. Options for prevention and management. Otolaryngol Clin North Am 1993; 26(3): 471-490.
56. Malafronte G, Filosa B, Cantone E: New macroscopic classification of stapedio-ovalar otosclerosis: a simplified rating for training in stapedotomy. Otol Neurotol 2008; 29(7): 889-892.
57. Olszewski Ł, Porowski M: Implanty ucha środkowego. [W:] Hojan E (red.): Protetyka słuchu. Wydawnictwo Naukowe UAM, Poznań 2014: 729-749.
58. Cheng HCS, Agrawal SK, Parnes LS: Stapedectomy Versus Stapedotomy. Otolaryngol Clin North Am 2018; 51(2): 375-392.
59. House HP, Hansen MR, Al Dakhail AA, House JW: Stapedectomy versus stapedotomy: comparison of results with long-term follow-up. Laryngoscope 2002; 112(11): 2046-2050.
60. Aantaa E, Virolainen E: The pre- and postoperative ENG findings in clinical otosclerosis and the late hearing results. Acta Otolaryngol 1978; 85(5-6): 313-317.
61. Pauw BK, Pollak AM, Fisch U: Utricle, saccule, and cochlear duct in relation to stapedotomy. A histologic human temporal bone study. Ann Otol Rhinol Laryngol 1991; 100(12): 966-970.
62. Ferster APO, Cureoglu S, Keskin N et al.: Secondary Endolymphatic Hydrops. Otol Neurotol 2017; 38(5): 774-779.