© Borgis - Postępy Nauk Medycznych 6/2014, s. 384-388
*Joanna Musialik1, 2, Henryk Karkoszka1, Andrzej Więcek1
Masywne stłuszczenie przeszczepionej wątroby u chorego zakażonego wirusem HCV o genotypie 3
Severe steatosis of transplanted liver in patient with genotype 3 hepatitis C virus infection
1Department of Nephrology, Endocrinology and Metabolic Diseases, School of Medicine in Katowice, Medical University of Silesia, Katowice
Head of Department: prof. Andrzej Więcek, MD, PhD
2Departament od Basic Biomedical Science, School of Pharmacy with Division of Laboratory Medicine in Sosnowiec, Medical University of Silesia, Katowice
Head of Department: prof. Barbara Błońska-Fajfrowska, MD, PhD
Streszczenie
Wstęp. Stłuszczenie wątroby jest częstym zjawiskiem obserwowanym u chorych przewlekle zakażonych wirusem C zapalenia wątroby (HCV) i może być zależne zarówno od czynników metabolicznych, jak i związanych z samym wirusem. Częstość występowania stłuszczenia waha się w szerokich granicach 40-80% i jest bardziej nasilona u chorych zakażonych wirusem HCV o genotypie 3. Do nawrotu infekcji HCV w wątrobie przeszczepionej dochodzi w większości przypadków, ale epidemiologia stłuszczenia wątroby u chorych zakażonych wirusem HCV o genotypie 3 jest słabo poznana z uwagi na niewielką liczbę chorych przeszczepionych i równocześnie zakażonych tym genotypem wirusa HCV.
Cel pracy. Ocena nasilenia stłuszczenia w wątrobie przeszczepionej u chorego zakażonego wirusem HCV o genotypie 3.
Materiał i metody. Przedstawiamy przypadek chorego zakażonego wirusem HCV o genotypie 3, u którego przeszczepienie wątroby zostało wykonane z powodu niewyrównanej marskości tego narządu z ogniskiem raka wątrobowokomórkowego.
Wyniki. Sześć miesięcy po ortotopowym przeszczepieniu wątroby wykazano we krwi chorego wysoką wiremię HCV – 2,4 x 107 IU/ml, a w badaniu histopatologicznym wątroby masywne stłuszczenie obejmujące 90% hepatocytów z obecnością nietypowego włóknienia.
Wnioski. Sądzimy, że w przedstawionym przypadku, nasilone i szybko postępujące stłuszczenie wątroby jest związane przede wszystkim z nawrotem zakażenia wirusem HCV o genotypie 3 w przeszczepionej wątrobie z wysoką wiremią będącą wynikiem intensywnego leczenia immunosupresyjnego we wczesnym okresie po transplantacji. Nasilenie stłuszczenia związane jest z pojawieniem się włóknienia w wątrobie. Ta obserwacja ma implikacje kliniczne u chorych po przeszczepieniu wątroby. Chorzy zakażeni wirusem HCV o genotypie 3, u których stwierdzono istotne stłuszczenie w wątrobie, powinni być kwalifikowani do pilnego rozpoczęcia terapii przeciwwirusowej, niezależnie od stopnia nasilenia włóknienia.
Summary
Introduction. Hepatic steatosis is a common feature of CHC infection and can be related to both metabolic and viral specific factors. The prevalence of steatosis ranges from 40 to 86% and is more frequent and more severe in patients infected with HCV genotype 3. The recurrence of HCV infection after liver transplantation is universal but epidemiology of liver steatosis in patients infected with genotype 3 HCV after liver transplantation is poorly explored because of relatively small number of transplanted patients infected with HCV genotype 3.
Aim. The aim of the study was assessment of severity of steatosis of transplanted liver in patient infected with HCV genotype 3.
Material and methods. We present a patient in whom the liver transplantation was done due to decompensated liver cirrhosis with focus of hepatocellular carcinoma infected with genotype 3 HCV.
Results. Six months after orthotopic liver transplantation (OLTx), high HCV viremia in patient’s serum – 2.4 x 107 IU/ml and severe steatosis comprising 90% of hepatocytes with atypical fibrosis in liver biopsy was found.
Conclusions. We conclude that massive and rapid steatosis is connected in our patient primarily with genotype 3 infection and high HCV viremia as a result of intensive immunosuppression in the early time after LTx. The severity of steatosis was correlated with the liver fibrosis state. This observation has practical implication for management in patients after LTx. Patients infected with HCV genotype 3 and presenting with liver steatosis should be offered antiviral therapy, irrespective of other considerations, as quickly as possible.

Introduction
Hepatitis C virus (HCV) infection is a major cause of chronic liver disease which induces end-stage liver disease and liver insufficiency due to cirrhosis or hepatocellular carcinoma. Currently it is the leading indication for liver transplantation (LTx) in most countries. Unfortunately, reinfection of new liver begins during reperfusion of the graft and accelerates liver disease and recurrent HCV disease is the most frequent cause of graft loss. First histological patterns of acute HCV appear usually between 4 and 12 week after transplantation. After 1 year features of chronic of chronic HCV appear in 70-90%, and after 5 years in 90-95% recipients. Chronic hepatitis C (CHC) can progress to cirrhosis quickly, affecting 10-30% of patients within 5 years after LTx (1, 2).
Steatosis, which is defined as increased fat content of the liver, is one of the factors exerting a significant impact on both liver fibrosis progression and response to antiviral therapy in native liver. There are two types of steatosis: micro- and macrosteatosis. Microsteatosis is defined as hepatocyte fat globules smaller than the size of the nucleus without macrovesicular deposit. Macrosteatosis occurs when large fat globules take up most of the cytoplasm, displacing the nucleus to the periphery. There is consensus that macrosteatosis affects liver graft function and survival more than microsteatosis. The clinical parameters used in classifying steatosis include less than 30% – mild steatosis, 31-60% – moderate steatosis and more than 60% – severe steatosis (3).
In patients with chronic hepatitis C, the prevalence of steatosis ranges from 40 to 86%. Almost 80% of patients with steatosis have mild steatosis affecting less than 30% of hepatocytes. Steatosis is more frequent and more severe in patients infected with HCV genotype 3 because this viral genotype, more often and more significantly than other genotypes, would be directly involved in the accumulation of triglycerides in hepatocytes (so called “viral” steatosis). Additionally, especially in patients with genotype 3, the severity of steatosis correlates with the level of HCV replication (4). In our paper we present a patient infected with genotype 3 HCV with severe steatosis of the liver graft as the form of HCV reinfection.
Aim
The aim of the study was assessment of severity of steatosis of transplanted liver in patient infected with HCV genotype 3.
Material and methods
We present a patient, who was a 57 years old man, who underwent liver transplantation for end--stage liver cirrhosis and focus of hepatocellular carcinoma (HCC) infected with genotype 3 HCV (an unknown pre-LTx viral load). The native liver removed at OLTx showed active cirrhosis and HCC focus. Steatosis was not evident on multiple sections of the explanted, native liver (fig. 1a, b, c).

Fig. 1a. Histology of explanted liver. H&E x 200. Typical cirrhotic regenerative noduli separated by fibrous septa in explanted liver of HCV patient.
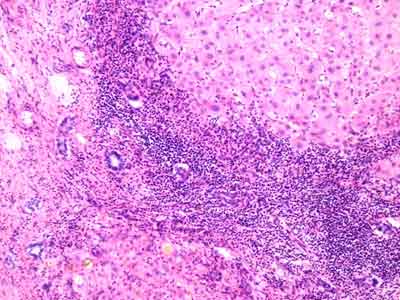
Fig. 1b. Histology of explanted liver. H&E x 200. Active cirrhosis. Dense mononuclear inflammatory infiltrate localized within and around the fibrous septa with interface hepatitis.
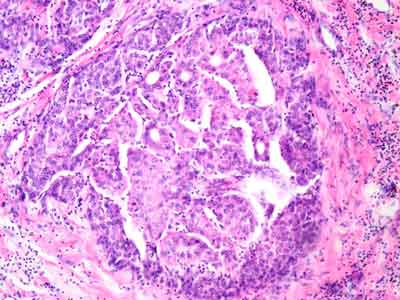
Fig. 1c. Histology of explanted liver. H&E x 200. Focus of hepatocellular carcinoma (trabecular-sinusoidal structure) in cirrhotic liver.
RESULTS
The donor was a healthy 19-year old man without diabetes mellitus (DM), hyperlipidemia, or history of obesity and with a BMI of 24 and normal liver function tests. The donor wedge liver biopsy obtained after reperfusion was unremarkable (fig. 2a, 2b).
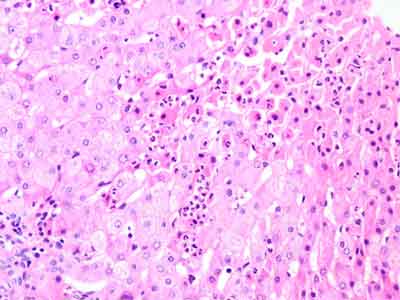
Fig. 2a. Histology of implanted liver. Postperfusion wedge liver donor biopsy. H&E x 200. One cell thick hepatocyte plates radiated out from the terminal venule. Note the accumulation of numerous neutrophils localized under the capsule within parenchyma, mark sites of hepatocellular necrosis. Typical features resulting from harvesting procedure.
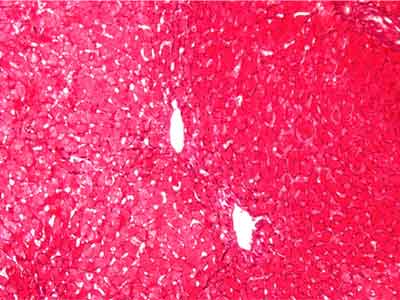
Fig. 2b. Histology of implanted liver. Wedge liver donor biopsy. Silver-methenamine x 200. Regular reticulin network between efferent hepatic venules.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Ciria R, Pleguezuelo M, Khorsandi SE et al.: Strategies to reduce hepatitis C virus recurrence after liver transplantation. World J Hepatol 2013; 5: 237-250.
2. Howell J, Angus P, Gow P: Hepatitis C recurrence: the Achilles heel of liver transplantation. Transpl Infect Dis 2013; 1: 1-16.
3. Turgeon NA, Sollingen HW, Fernandez LA et al.: Hepatic steatosis and liver transplantation. Curr Opin Organ Transplant 2004; 9: 123-129.
4. Negro F: Hepatitis C virus-induced steatosis – an overview. Dig Dis 2010; 28: 294-299.
5. Hubscher S: Steatosis and fibrosis progression in patients with recurrent hepatitis C infection: complex interactions providing diagnostic and therapeutic challenges. Liver Transplant 2011; 17: 1374-1379.
6. Rubbia-Brandt L, Fabris P, Paganin S et al.: Steatosis affects chronic hepatitis C progression in a genotype specific way. Gut 2004; 53: 406-412.
7. Rubbia-Brandt L, Quadri R, Abid K et al.: Hepatocyte steatosis is a cythopatic effect of hepatitis C virus genotype 3. J Hepatol 2000; 33: 105-115.
8. Gallegos-Orozco JF, Yosephy A, Noble B et al.: Natural history of post-liver transplantation hepatitis C: a review of factors that may influence its course. Liver Transpl 2009; 15: 1872-1881.
9. Bandman D, Pingitore A, Lai JC et al.: Hepatic steatosis at 1 year is an additional predictor of subsequent fibrosis severity in liver transplant recipients with recurrent hepatitis C virus. Liver Transpl 2011; 17: 1380-1386.
10. Firpi RF, Clark V, Soldevila-Pico C et al.: The natural history of hepatitis C cirrhosis after liver transplantation. Liver Transpl 2009; 15: 1063-1071.
11. Iacob S, Cicinnati VR, Hilgard P et al.: Predictors of graft and patient survival in hepatitis C virus (HCV) recipients: model to predict HCV cirrhosis after liver transplantation. Transplantation 2007; 84: 56-63.
12. Gordon FD, Kwo P, Ghalib R et al.: Peginterferon-α-2b and ribavirin for hepatitis C recurrence postorthotopic liver transplantation. J Clin Gastroenterol 2012; 46(8): 700-708.
13. Ghabril M, Dickson RC, Krishna M et al.: Explanted liver inflammatory grade predicts fibrosis progression in hepatitis C recurrence. Liver Transplant 2011; 17: 685-694.
14. Sampson MA, Khettry U, Gordon FD et al.: Explant periseptitis or inflammation > 2 is strongly associated with clinically significant hepatitis C (HCV) recurrence after liver tx (LTx). Liver Transplant 2009; 15: S94-S95.
