*Konrad Wroński1, 2, Maciej Żechowicz1, 3, Leszek Frąckowiak1, 4, Mariusz Koda5
Primary woman neuroendocrine breast tumor – case report and review of the literature
1Department of Oncology, Faculty of Medicine, University of Warmia and Mazury, Olsztyn, Poland
Head of Department: prof. Sergiusz Nawrocki, MD, PhD
2Department of Surgical Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department: Andrzej Lachowski, MD
3Department of Internal Diseases, Gastroenterology, Cardiology and Infectiology Faculty of Medicine, University of Warmia and Mazury, Olsztyn, Poland
Head of Department: prof. Piotr Zaborowski, MD, PhD
4Department of Gynecology and Gynecologic Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department: Leszek Frąckowiak, MD, PhD
5Department of Pathomorphology, Białystok Oncology Centre, Poland
Head of Department: prof. Waldemar Famulski, MD, PhD, DSc
Summary
Primary neuroendocrine breast carcinoma (NEBC) is extremely rare type of breast tumor and has been reported sporadically. Most neuroendocrine tumors are located in the gastrointestinal tract. This type of breast cancer was first time recognized by the WHO in 2003. Because of its rarity, there is little knowledge about its epidemiology, biology and there is no standard treatment protocol and a large variety of chemotherapy protocols have been employed in treating this disease.The primary neuroendocrine breast carcinomas may give distant metastasis to bone and liver but also to other sites include: lungs, mediastinal lymph nodes, adrenal glands, fallopian tubes, colon, ileum and pancreas. The treatment of neuroendorcine breast carcinomas need multimodal therapy. So that it is important to treat women in high specialized oncological centers.
The authors of this article presented a case of a 45-year-old Caucasian woman who was treated in the hospital because of primary neuroendocrine breast cancer. The authors performed a literature review on primary neuroendocrine breast cancer diagnosis and treatment.
INTRODUCTION
Primary neuroendocrine breast carcinoma (NEBC) is extremely rare type of breast tumor and has been reported sporadically (1, 2). This type of breast cancer was first time recognized by the WHO in 2003 (3, 4). Because of its rarity, there is little knowledge about its epidemiology, biology and there is no standard treatment protocol and a large variety of chemotherapy protocols have been employed in treating this disease.
CASE REPORT
A 45-year-old Caucasian woman was referred to the Department of Surgical Oncology due to breast tumor discovered incidentally in ultrasound examination. The size of this tumor in ultrasound was 22 x 18 mm and it was located in the outer upper quadrant of the right breast. She had no any other symptoms, there was no history of weight loss and loss of appetite. The patient was not treated for chronically diseases. She had no surgeries and there was no history of carcinoma in patient family. Blood test and other routine hematological examinations and biochemical tests were within normal limits.
In the Department of Surgical Oncology the patient had open surgical biopsy of breast tumor. After biopsy due to condition of the patient. Next day after the biopsy, the patient left the department.
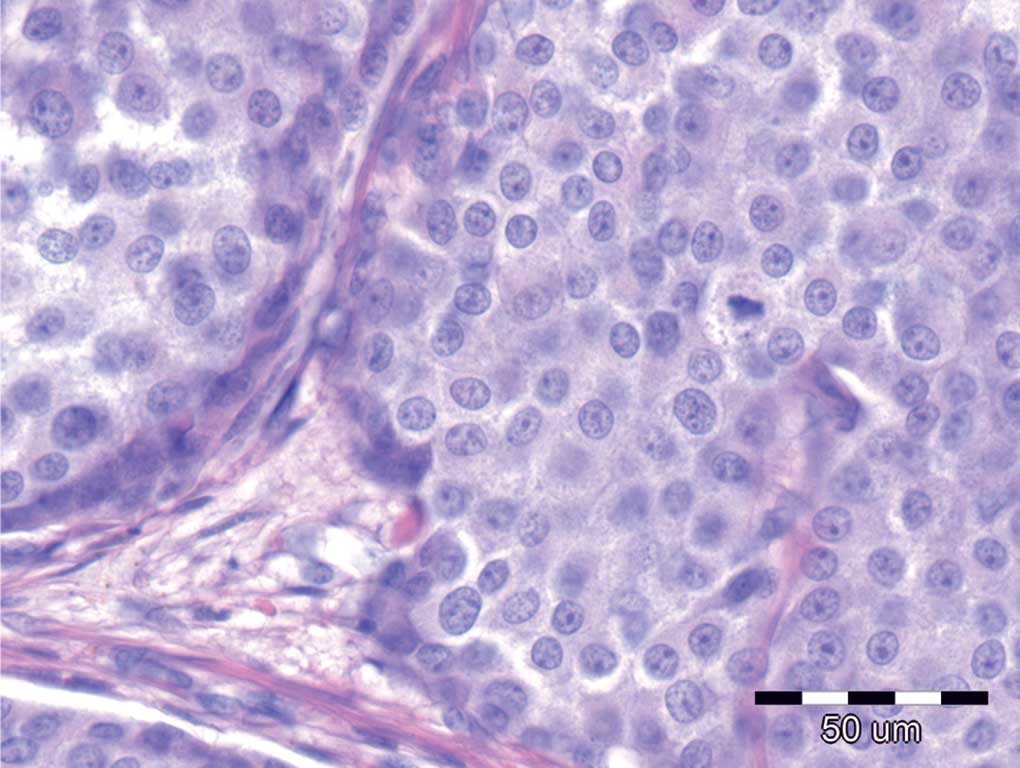
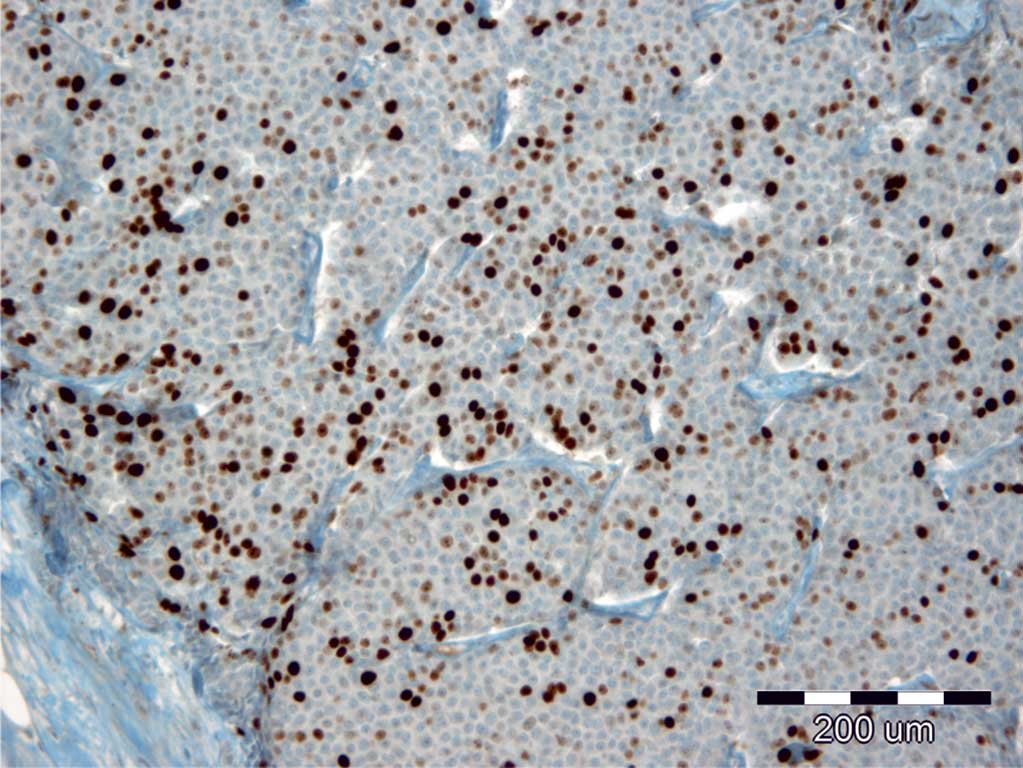
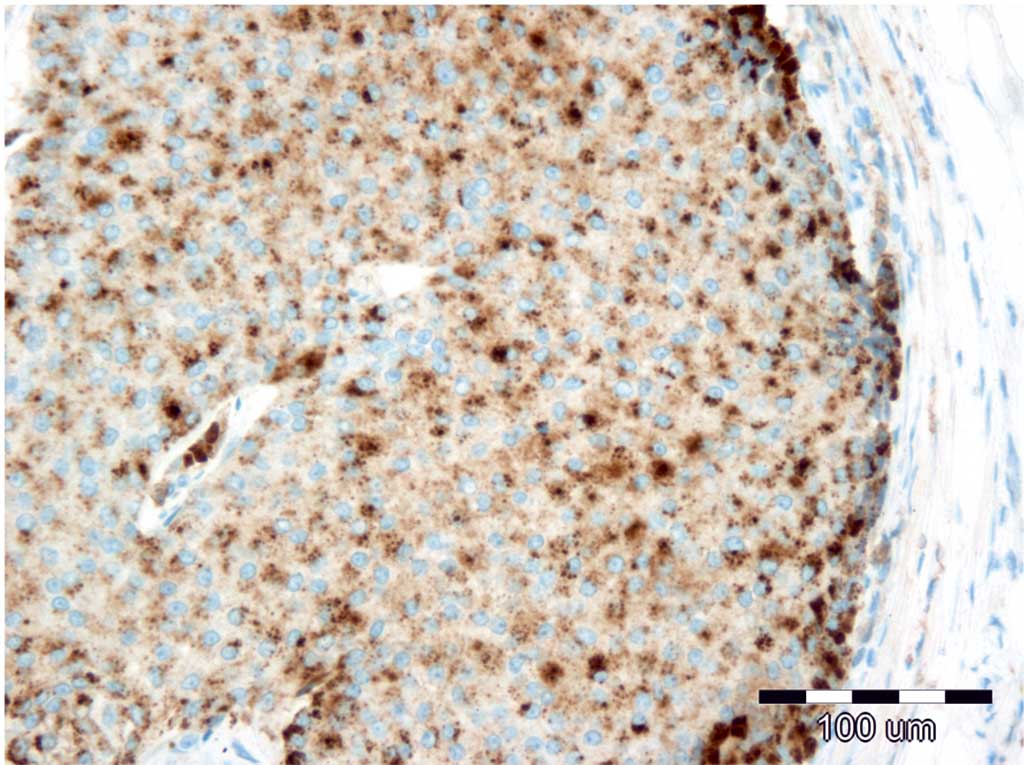
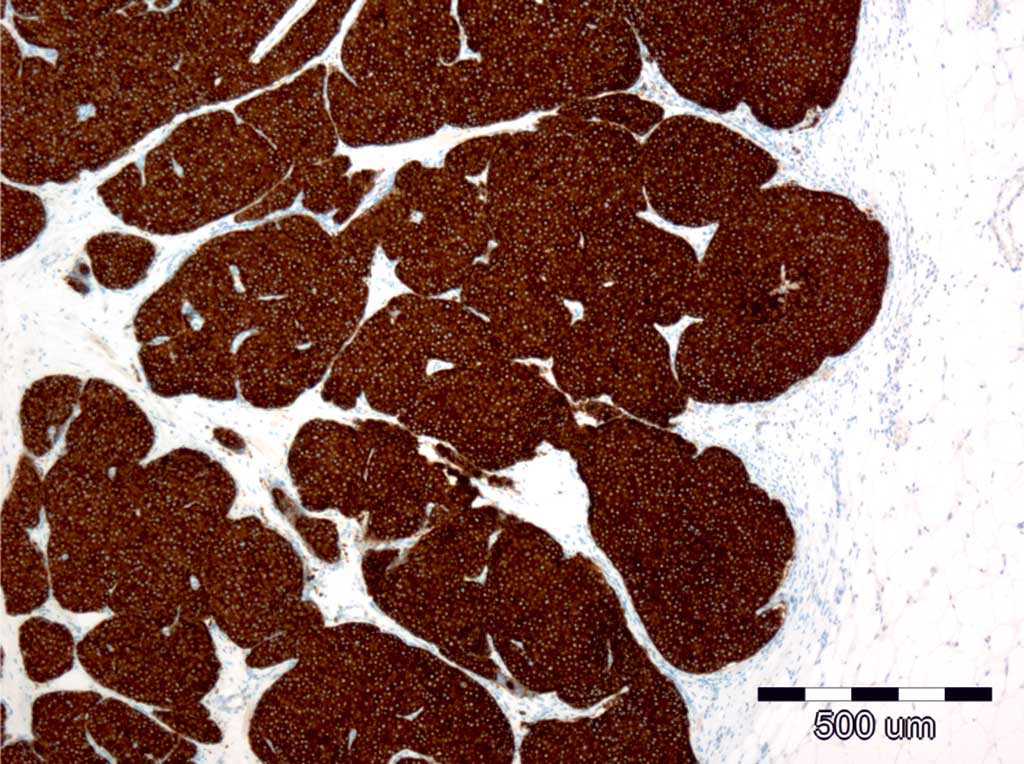
Pathological diagnosis showed neuroendocrine tumor well-differentiated (fig. 1, 2). Tumor cells were ER (+) in 90%, PR (+) in 90%, Ki67 (+) in 30%, chromogranin (+++), synaptophysin (++), E-cadherin (++) and Her2 (0) (fig. 3-7).
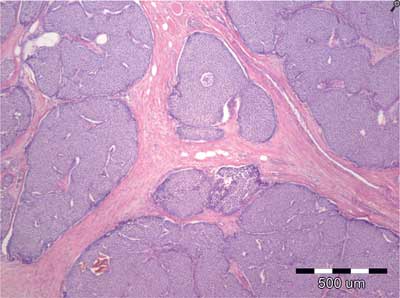
Fig. 1. Neuroendocrine tumor cells in the breast. Hematoxylin--Eosin staining, 40x.
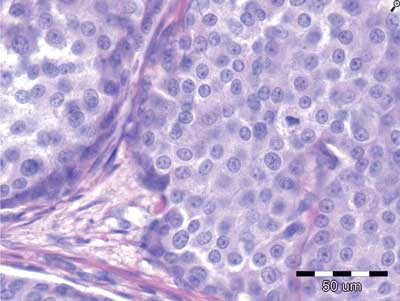
Fig. 2. Neuroendocrine tumor cells in the breast. Hematoxylin--Eosin staining, 400x.
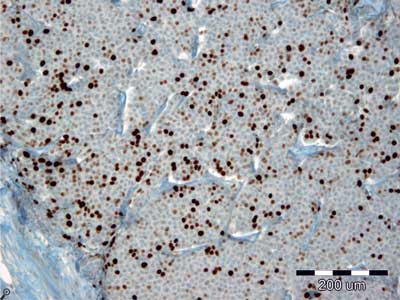
Fig. 3. Tumor cells are positive to Ki-67 in 30% (100x).
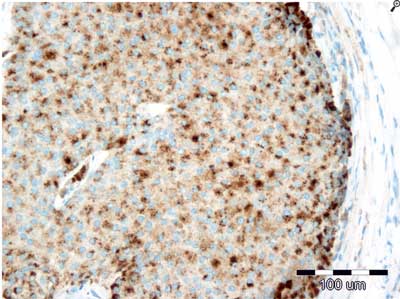
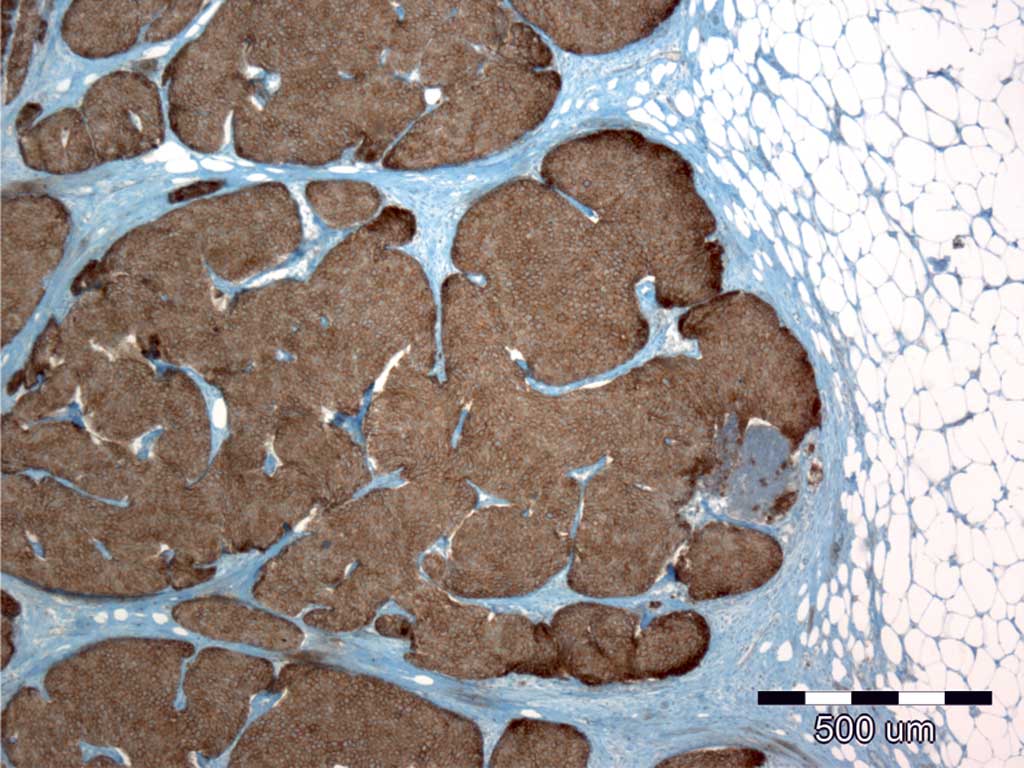
Fig. 4. Tumor cells are positive to chromogranin (200x).
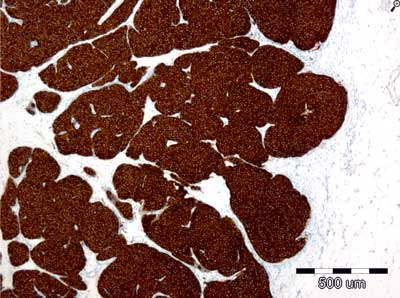
Fig. 5. Tumor cells are positive to synaptophysin (40x).
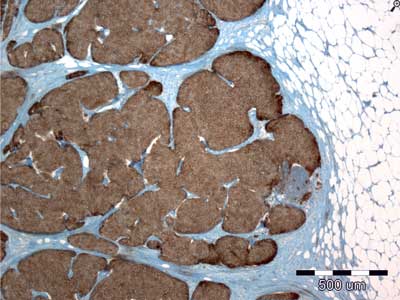
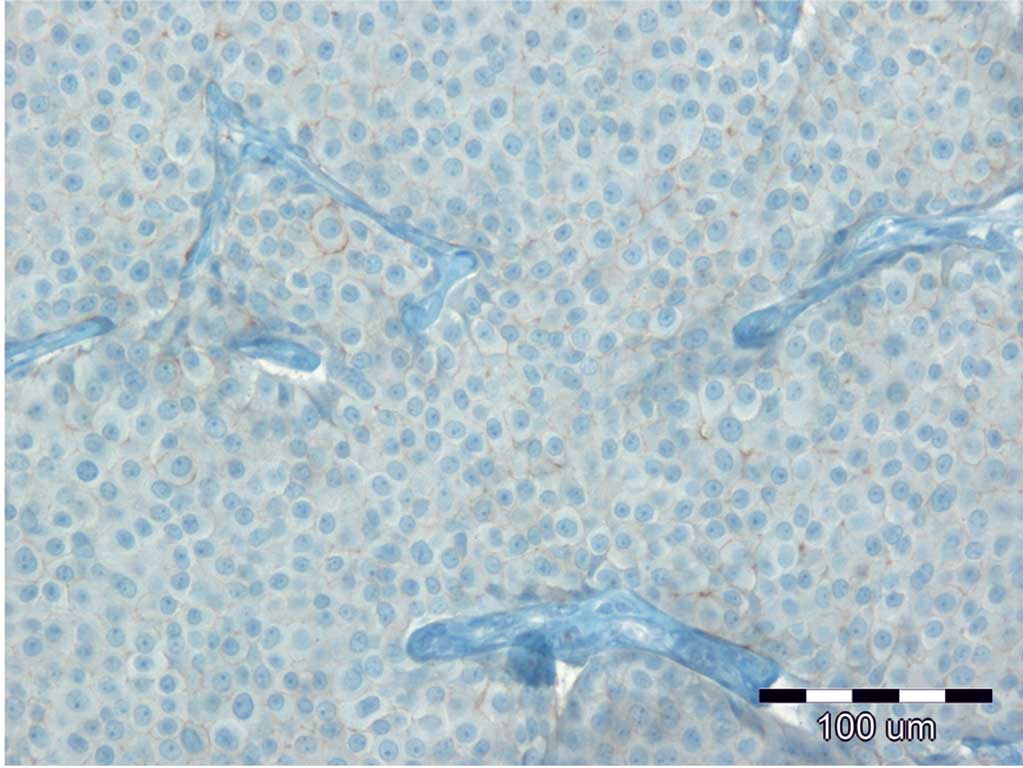
Fig. 6. Tumor cells are positive to E-cadherin (200x).
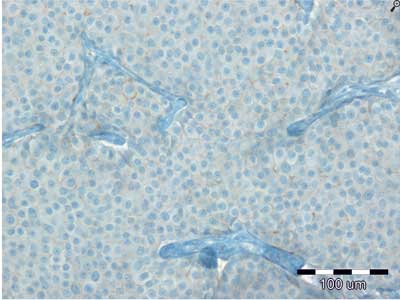
Fig. 7. Tumor cells had no Her2 (200x).
The patient was admitted to The Department of Surgical Oncology to comply quadrantectomy right breast and surgical biopsy of sentinel lymph node. Due to the unsuccessful attempt of sentinel lymph node marks, the patient was qualified to quadrantectomy right breast with axillary lymphadenectomy right-sided. She underwent surgery and left the Department two days after surgery.
Histopathology examination of material showed metastases in 13 among 20 removed lymph nodes in the right armpit (fig. 8). The patient was referred for further systematic treatment.

Fig. 8. Removed enlarged axillar lymph nodes.
DISCUSSION
Primary neuroendocrine breast carcinoma (NEBC) is extremely rare type of breast tumor and has been reported sporadically (1, 2). It is estimated that NEBC occurs from 0.3% to 0.5% of all breast cancer specimens (2, 5). According to Ogawa et al. (6), it accounts for less than 0.1% of all breast cancer and less than 1% of all neuroendocrine tumors, but according to the most recent World Health Organization (WHO) classification of breast and gynecologic tumors their incidence is estimated, approximately, to 1% of all breast carcinomas (3). This cancer occurs more often in white women (7). This type of breast cancer was first time recognized by the WHO in 2003 and defined as the expression of neuroendocrine markers in more than 50% tumor cells (3, 4). WHO divided neuroendocrine carcinomas into three subtypes:
1. neuroendocrine tumor, well-differentiated,
2. neuroendocrine carcinoma, poorly differentiated/small cell carcinoma and
3. invasive breast carcinoma with neuroendocrine differentiation.
Pathologists rely on using a two the most sensitive and specific neuroendocrine markers: chromogranin A or B and synaptophysin. More than 80% of neuroendocrine breast carcinomas express progesterone receptor (PR) or estrogen receptor (ER) (8). Her-2 expression is nonexistent or rarely present in this tumor (7, 9).
Prognosis seems to correlate with the stage of disease (10). There are no specific recommendation regarding surgical management. Patients should be treated similarly to invasive ductal carcinoma depends on clinical stage and location of the tumor (11). About 50% of the regional lymph nodes are involved at the time of diagnosis, similarly as in the case reported by the authors.
Adjuvant radiation and chemotherapy plays important role in systematic treatment of neuroendocrine breast carcinomas (12). Also patients with positive for estrogen and progesterone receptors should have hormonal therapy (13).
The primary neuroendocrine breast carcinomas may give distant metastasis (6, 7). The most common places for distant metastasis are: bone and liver (7). Other sites include: lungs, mediastinal lymph nodes, adrenal glands, fallopian tubes, colon, ileum and pancreas (7).
The treatment of neuroendorcine breast carcinomas need multimodal therapy. So that it is important to treat women in high specialized oncological centers.
CONCLUSIONs
1. Primary neuroendocrine breast carcinoma (NEBC) is extremely rare.
2. Most neuroendocrine tumors are located in the gastrointestinal tract.
3. Because of its rarity, there is no standard treatment protocol and a large variety of chemotherapy protocols have been employed in treating this disease.
4. The primary neuroendocrine breast carcinomas may give distant metastasis especially to: bones and liver.
Piśmiennictwo
1. Jundt G, Schulz A, Heitz PU et al.: Small-cell neuroendocrine (oat cell) carcinoma of the male breast. Immunocytochemical and ultrastructural investigations. Vurchows Arch A Pathol Anat Histopathol 1984; 404(2): 213-221. 2. Gunhan-Bilgen I, Zekioglu O, Ustun EE et al.: Neuroendocrine differentiated breast carcinoma: imaging features correlated with clinical and histopathological findings. Eur Radiol 2003; 13(4): 788-793. 3. Ellis P, Schnitt SJ, Sastre-Garau X: Invasive breast carcinoma. [In:] Tavassoli FA, Deyilee P (eds.): Tumors of the Breast and Female Genital Organ: Pathology and Genetics. IARC Press, Lyon 2003. 4. Lakhani S, Ellis I, Schnitt S et al.: WHO Classif. Tumours Breast. IARC Press, Lyon 2012: 62-63. 5. Lopez-Bonet E, Alonso-Ruano M, Barraza G et al.: Solid neuroendocrine breast carcinomas: incidence, clinic-pathological features and immunohistochemical profiling. Oncol Rep 2008; 20(6): 1369-1374. 6. Ogawa H, Nishio A, Satake H et al.: Neuroendocrine tumor in the breast. Radiat Med 2008; 26: 28-32. 7. Wei B, Ding T, Xing Y et al.: Invasive neuroendocrine carcinoma of the breast: a distinctive subtype of aggressive mammary carcinoma. Cancer 2010; 116(19): 4463-4473. 8. Alkaied H, Harris K, Brenner A et al.: Does hormonal therapy have a therapeutic role in metastatic primary small-cell neuroendocrine breast carcinoma? Case report and literature review. Clin Breast Cancer 2012; 12(3): 226-230. 9. Zekioglu O, Erhan Y, Ciris M et al.: Neuroendocrine differentiated carcinomas of the breast: a distinct entity. Breast 2003; 12(4): 251-257. 10. Papotti M, Macri L, Finzi G et al.: Neuroendocrine differentiation in carcinomas of the breast: a study of 51 cases. Semi Diagn Pathol 1989; 6: 174-188. 11. Richter-Ehrenstein C, Arndt J, Buckendahl AC et al.: Solid neuroendocrine carcinomas of the breast: metastases or primary tumors? Breast Cancer Res Treat 2010; 124: 413-417. 12. Tian Z, Wei B, Tang F et al.: Prognostic significance of tumor grading and staging in mammary carcinomas with neuroendocrine differentiation. Hum Pathol 2011; 42(8): 1169-1177. 13. Bourhaleb Z, Uri N, Haddad H et al.: Neuroendocrine carcinoma with large cell of the breast: case report and review of the literature. Cancer Radiother 2009; 13(8): 775-777.