© Borgis - Postępy Nauk Medycznych 8/2015, s. 567-569
*Andrzej Głowniak, Adam Tarkowski, Anna Jaroszyńska, Marek Jankiewicz, Andrzej Wysokiński
Przejściowe objawowe uniesienie odcinka ST po nakłuciu transseptalnym podczas zabiegu izolacji żył płucnych
Transient symptomatic ST-segment elevation following transseptal puncture for pulmonary vein isolation
Chair and Department of Cardiology, Medical University, Lublin
Head of Department: prof. Andrzej Wysokiński, MD, PhD
Streszczenie
Zabieg izolacji żył płucnych (PVI) jest standardowym postępowaniem w przypadku nawracającego, lekoopornego migotania przedsionków. Dostęp do miejsca aplikacji uzyskiwany jest poprzez wykonanie punkcji transseptalnej, niosącej ze sobą ryzyko potencjalnych powikłań. Przedstawiamy opis przypadku przejściowego, objawowego uniesienia odcinka ST, które wystąpiło u 57-letniego mężczyzny poddanego zabiegowi izolacji żył płucnych bezpośrednio po wykonaniu nakłucia transseptalnego. Zmiany odcinka ST oraz objawy kliniczne ustąpiły w ciągu kolejnych 5 minut, niemniej z uwagi na obecne czynniki ryzyka zdecydowano o przerwaniu zabiegu oraz wykonaniu pilnej angiografii naczyń wieńcowych, która nie wykazała obecności istotnych zmian mogących odpowiadać za stwierdzone przejściowe zmiany odcinka ST. Zabieg skutecznej izolacji żył płucnych wykonano następnego dnia bez powikłań. Poniżej dokonujemy przeglądu literatury opisującej podobne przypadki oraz omawiamy możliwe przyczyny tego zjawiska. Przedstawione dane sugerują, że wystąpienie przejściowego uniesienia odcinak ST podczas nakłucia transseptalnego jest rzadko obserwowanym powikłaniem, jednak nie powinno być ono przeciwwskazaniem do wykonania zabiegu izolacji żył płucnych po wnikliwej ocenie stanu pacjenta.
Summary
Pulmonary vein isolation (PVI) become a standard procedure in atrial fibrillation (AF) treatment, proved to be more effective than antiarrhythmic medication alone. The procedure of PVI requires access to the left atrium, provided by the transseptal puncture (TSP), which carries potential risk of complication. We describe a case of transient, symptomatic ST-segment elevation in 57 year old male following TSP during PVI procedure. The symptoms resolved completely within next 5 minutes, however, concerning the potential risk factors we decided to discontinue the procedure and perform coronary angiography, which revealed no significant changes in the coronary arteries. Successful pulmonary vein isolation procedure was performed the next day without complications. We review the literature and discuss the possible causes of this phenomenon. The data suggest that transient ST-segment elevation is a rare incident associated with transseptal puncture, yet it should not impede continuation of the ablation procedure after thorough evaluation of the patient.

Introduction
The transseptal puncture for left atrial (LA) access is a fundamental method of catheter ablation of LA-originating arrhythmias, including atrial fibrillation (AF) (1-3). ST-segment elevation associated with transseptal puncture has been recognized as a rare complication of this procedure (4-12). We describe a case of ST-segment elevation with concomitant stenocardia that appeared soon after the transseptal puncture. Additionally, we review the literature on ST-segment elevation associated with transseptal puncture and discuss the potential underlying mechanisms.
Case report
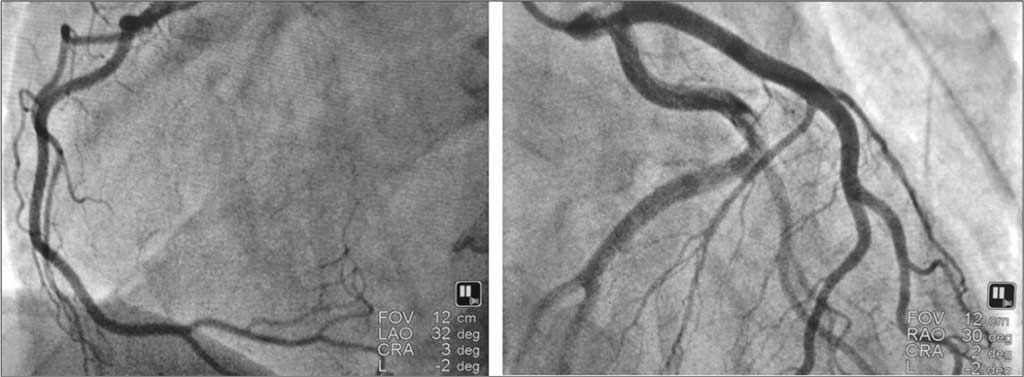
A 57-year old male with symptomatic (EHRA III) paroxysmal atrial fibrillation was referred to our center for AF ablation. The patient had the history arterial hypertension and smoking (10 cigarettes per day for 30 years). Physical examination, ECG, transthoracic and transesophageal echocardiography revealed no abnormalities. CT scan performed before hospitalization presented normal anatomical configuration of 4 pulmonary veins. The procedure was performed in fasting state, with interrupted oral anticoagulation (rivaroxaban). Fluoroscopy-guided transseptal puncture was performed with 8.5 F transseptal sheath and Brockenborough’s needle applying standard technique. Once the sheath was introduced to left atrium, the bolus of heparine (10 000 u) was given to avoid thromboembolic complication. Approximately 2 min after the transseptal puncture the patient reported increasing heart pain, with the drop of blood pressure from 135/75 to 85/50. The 12-lead ECG revealed ST-segment elevation in leads II, III and aVF with “mirror” depression in leads I and aVL (fig. 1). The ECG abnormalities resolved spontaneously in the following 5 minutes and normal blood pressure was restored, however, considering the risk factors of potentially co-existing coronary artery disease we decided to stop the ablation procedure. Coronary angiography performed afterwards revealed no significant abnormalities (fig. 2). Successful AF ablation was performed on the following day with no complications.
Fig. 1. ECG recorded 1 min after transseptal puncture, presenting ST-segment elevation in leads II, III and aVF.

Fig. 2. Coronary angiography showing the LAO 30° projection of the right coronary artery (left panel) and RAO 30° projection of the left coronary artery (right panel).
Discussion
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Croft CH, Lipscomb K: Modified technique of transseptal left heart catheterization. J Am Coll Cardiol 1985; 5: 904-910.
2. Wazni OM, Marrouche NF, Martin DO et al.: Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA 2005; 293: 2634-2640.
3. Calkins H, Kuck KH, Cappato R et al.: 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendations for Patient Selection, Procedural Techniques, Patient Management and Follow-up, Definitions, Endpoints, and Research Trial Design. Europace 2012; 14: 528-606.
4. Simon RD, Gill JS: Coronary ischemia induced by radiofrequency ablation in the left atrium. J Cardiovasc Electrophysiol 2003; 14: 186-190.
5. Arita T, Kubota S, Okamoto K et al.: Bezold-Jarisch-like reflex during brockenbrough’s procedure for radiofrequency catheter ablation of focal left atrial fibrillation: report of two cases. J Interv Card Electrophysiol 2003; 8: 195-202.
6. Schwab JO, Burkhardt D, Yang A et al.: ECG signs mimicking acute inferior wall myocardial infarction associated with elevated myocardial enzymes during isolation of pulmonary veins for focal atrial fibrillation. Europace 2004; 6: 111-115.
7. Tada H, Naito S, Oshima S et al.: Vasospastic angina shortly after left atrial catheter ablation for atrial fibrillation. Heart Rhythm 2005; 2: 867-870.
8. Risius T, Lewalter T, Lüderitz B et al.: Transient ST-segment-elevation during pulmonary vein ablation using circumferential coiled microelectrodes in a prospective multi-centre study. Europace 2006; 8: 178-181.
9. Efremidis M, Letsas KP, Xydonas S et al.: ECG findings of acute myocardial infarction and atrioventricular block during a transseptal procedure for left atrial ablation. Hell J Cardiol 2008; 49: 284-287.
10. Michael KA, Redfearn DP, Simpson CS et al.: Anunusual complication of a pulmonary vein isolation. J Interv Card Electrophysiol 2009; 25: 203-205.
11. Le BH, Black JN, Huang SK: Transient ST-segment elevation during transseptal catheterization for atrial fibrillation ablation. Tex Heart Inst J 2010; 37: 717-721.
12. Ishigaki D, Takanori A, Tadateru I et al.: ST-segment elevation and ventricular fibrillation shortly after transseptal puncture for left atrial catheter ablation. J Arrhythmia 2013; 29: 296-299.