*Konrad Wroński1, 2, Przemysław Stefaniak2
New type of prophylactic gastroenterostomy in patient with unresectable pancreatic head carcinoma
1Department of Oncology, Faculty of Medicine, University of Warmia and Mazury, Olsztyn, Poland
Head of Department: prof. Sergiusz Nawrocki, MD, PhD
2Department of Surgical Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department: Andrzej Lachowski, MD
Summary
Pancreatic cancer is a important public health problem all over the world. Up to 80% patients with carcinoma of head of the pancreas are unresectable because of local vascular invasion or distant metastasis. Optimal treatment of such patients is surgical bypass. The number of patients with unresectable pancreatic head cancers is increasing and their optimal treatment is a big economic problem for health care. Traditional prophylactic gastroenterostomy has many complications in postoperative period. Because of complications period of stay in hospital extended and generates additional costs. In this article the authors presented a case of a Caucasian woman who was admitted to the hospital because of unresectable pancreatic head cancer. The patient underwent new type of prophylactic gastroenterostomy and in the sixth day after surgery was discharged home. The authors invented this new type of anastomosis and applied it successfully in several patients with unresectable carcinoma of head of the pancreas.
INTRODUCTION
Pancreatic cancer is a important public health problem all over the world. Up to 80% patients with carcinoma of head of the pancreas are unresectable because of local vascular invasion or distant metastasis (1). Optimal treatment of such patients is surgical bypass. The number of patients with unresectable pancreatic head cancers is increasing and their optimal treatment is a big economic problem for health care. Traditional prophylactic gastroenterostomy has many complications in postoperative period. Because of complications period of stay in hospital extended and generates additional costs. In this article the authors presented a case of a Caucasian woman who was admitted to the hospital because of unresectable pancreatic head cancer. The patient underwent new type of prophylactic gastroenterostomy and in the sixth day after surgery was discharged home. The authors invented this new type of anastomosis and applied it successfully in several patients with unresectable carcinoma of head of the pancreas.
CASE REPORT
A 71-year-old woman, Caucasian race, with pancreatic head tumor, was admitted to the Department of Surgical Oncology because of obstructive symptoms of upper gastrointestinal tract. The patient did not eat the food for last 2 weeks, drank only water. Within a month, she lost about 20 kg. She was treated chronically with hypertension and ischemic heart disease.
Blood examination of the patient showed low levels of hemoglobin, erythrocytes, albumin and total protein. Other laboratory tests were normal.
On physical examination, in the epigastrium area there was palpable a tumor. CT examination showed a pathological mesogastric lumpy mass in the region of the descending duodenum and the head of the pancreas, which the size was approximately 75 x 68 x 45 mm. The rest of the pancreas was not enlarged. On CT scan a tumor of the pancreas head infiltrated and compressed the duodenum causing obstruction of the upper gastrointestinal tract.
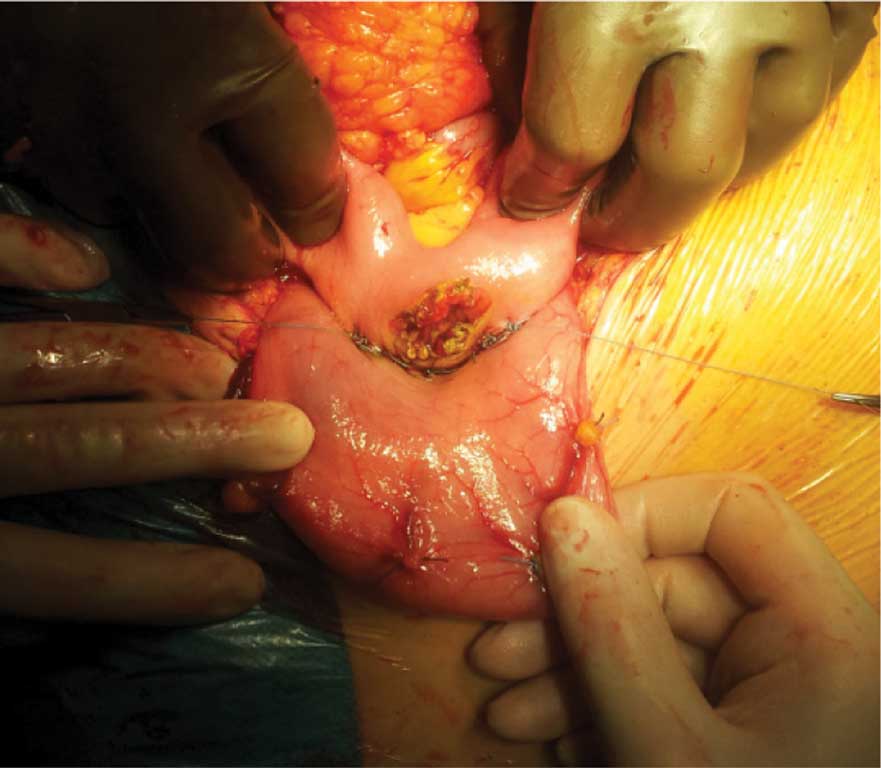
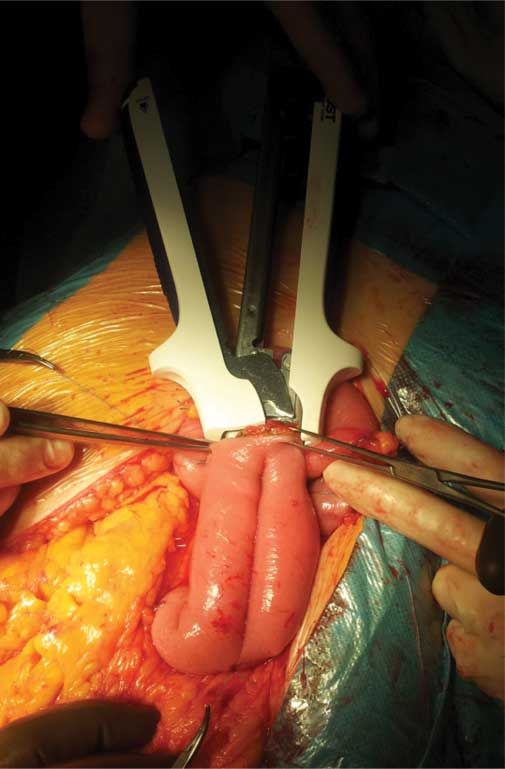
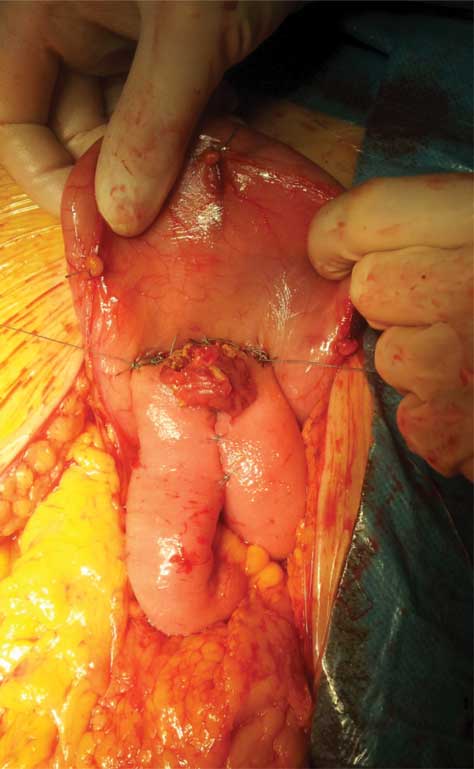
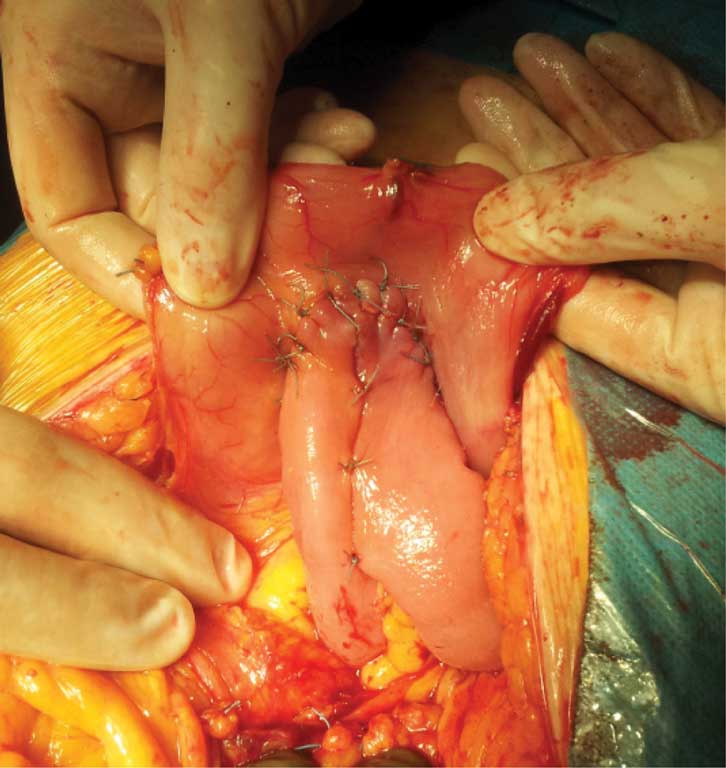
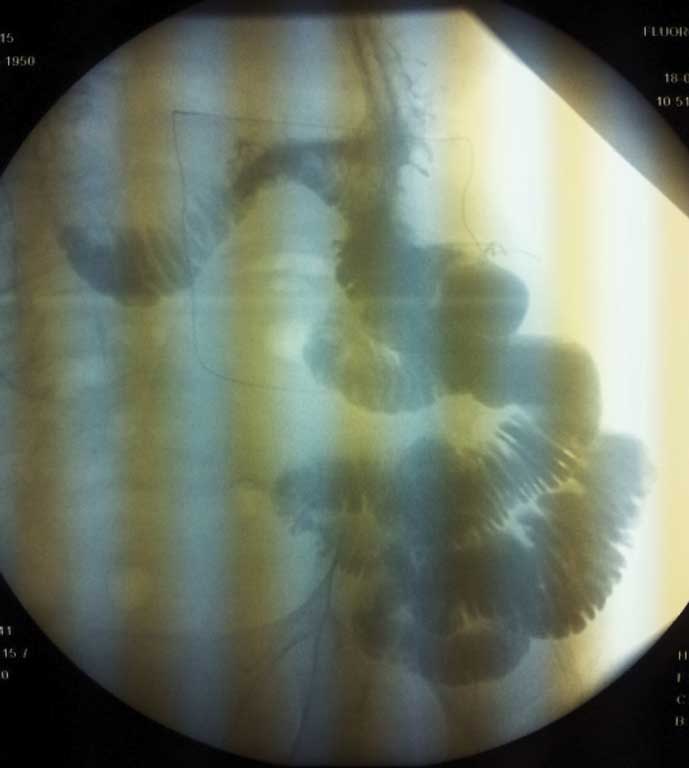
The patient was qualified for surgery. After opening the abdomen and reaching the pancreas, surgeons found a large tumor of the pancreatic head diameter about 70 mm infiltrating on celiac trunk, duodenum and superior mesenteric artery. The case was considered as an inoperable. Tumor stage was assessed on: cT4NXM0. Samples were collected for intra histopathological examination from unresectable pancreatic tumor. Pathological examination revealed the presence of cancer cells. The patient had performed new type of prophylactic gastroenterostomy with formation of the small intestine tank (fig. 1-4). The duration of surgery was 70 minutes. Patient after surgery felt good and did not complain of pain. The postoperative period was uncomplicated and the patient left the ward in the sixth day after operation. In the first day after operation the patient had X-ray scan which showed the free flow of contrast through the place of gastroenterostomy (fig. 5). On the second day the patient underwent gastroscopy in which there is no swelling of the tissues around the anastomosis and the free passage of the endoscope from the stomach into the small intestine. The patient is in the care of outpatient surgical oncology and was pre-qualified for palliative chemotherapy.
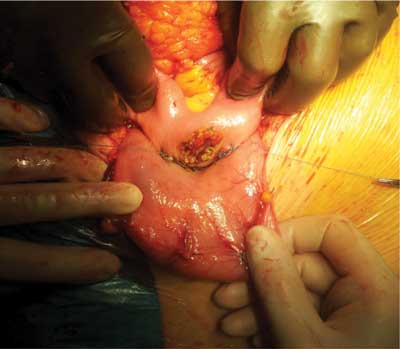
Fig. 1. Photo after the anastomosis posterior wall of the stomach and small intestine.
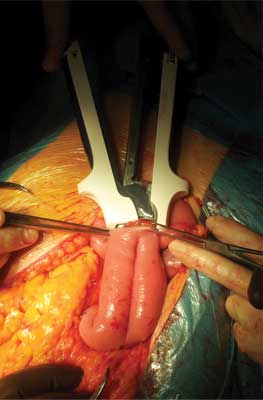
Fig. 2. Creation of the container on the small intestine using a stapler.

Fig. 3. Image showing status after formation of the small intestine tank.

Fig. 4. New type of prophylactic gastroenterostomy.
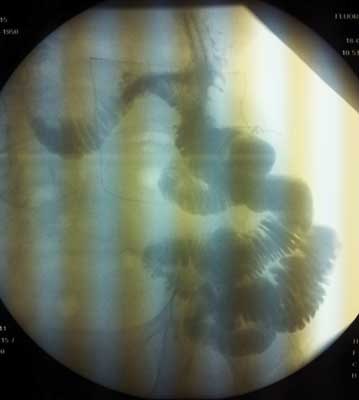
Fig. 5. X-ray picture showing the free flow of contrast through the place anastomosis in the first postoperative day.
DISCUSSION
Pancreatic neoplasms account for 3% of all cancers in Poland (2). A large number of patients with unresectable pancreatic head cancer is a growing challenge for health care (3, 4). In the case of such patients, a prospective randomized controlled trial confirmed that prophylactic gastrojejunostomy should be done (5). If prophylactic gastroenterostomy is not done it connection with 20% die because of some symptoms of duodenal obstruction and up to 21% second laparotomy with gastrojejunostomy due to symptoms of duodenal obstruction (6-8).
The authors of this article found in Pubmed base many article which describe complications of prophylactic gastroenterostomy in inoperable head of the pancreas carcinoma. One of the unfavorable symptoms after gastroenterostomy is delay gastric emptying (DGE). Delay gastric emptying is defined by the International Study Group of Pancreatic Cancer as a problem, which has been linked to tumor involvement of the coeliac axis and interruption of splanchnic innervations (1 ,4, 5).
In Raymond et al. research mortality after gastrojejunostomy was 18% and after combined biliary and duodenal bypass surgery 5%. In this research 26% patients had delayed gastric emptying postoperatively from 9 to 31 days. The authors of this article think that delayed gastric emptying is frequent and serious problem for patients with unresectable pancreatic cancer (9).
In Lesurtel et al. article 4.8% patients developed late gastric obstruction symptoms after bypass surgery. The authors of this article believe that biliary and gastric bypass done together reduce problem with delay gastric emptying (10). Horstmann et al. estimate that the delay gastric emptying occurs in 9 to 26% of patients after gastrojejunostomy bypass (11).
According to the authors of this article correct technique of new prophylactic gastroenterostomy helps to reduce to a minimum complications in postoperative period. The authors of this article believe that formation of the small intestine tank in bypass is the key to reduce postoperative complication and inclusion in the first day after surgery the patient nutrition.
CONCUSIONS
The authors of this article, having an experience in the treatment of patients with unresectable cancer of the pancreatic head believes, that new type of prophylactic gastroenterostomy can be new „the gold standard” in the treatment of such patients. This new type of gastroenterostomy is easy and safely procedure, and reduces costs of health care due to postoperative complications after traditional gastroenterostomy.
There is a need for further multicenter study on a larger group of patients with inoperable pancreatic cancer to understand confirm the good effects of a new anastomosis in such patients. Patients who underwent surgery will be monitored in our surgical outpatient.
Piśmiennictwo
1. Watanapa P, Williamson RC: Surgical palliation for pancreatic cancer: developments during the past two decades. Br J Surg 1992; 79: 8-20. 2. Krzakowski M, Warzocha K (red.): Zalecenia postępowania diagnostyczno-terapeutycznego w nowotworach złośliwych 2013 rok. Via Medica, Gdańsk 2013. 3. Hwang SI, Kim HO, Son BH et al.: Surgical palliation of unresectable pancreatic head cancer in elderly patients. World J Gastroenterol 2009; 15: 978-982. 4. Huser N, Michalski CW, Schuster T et al.: Systematic review and meta-analysis of prophylactic gastroenterostomy for unresectable advanced pancreatic cancer. Br J Surg 2009; 96: 711-719. 5. Jacobs PP, van der Sluis RF, Wobbes T: Role of gastroenterostomy in the palliative surgical treatment of pancreatic cancer. J Surg Oncol 1989; 42: 145-149. 6. Weaver DW, Wiencek RG, Bouwman DL et al.: Gastrojejunostomy: is it helpful for patients with pancreatic cancer? Surgery 1987; 102: 608-613. 7. Doberneck RC, Berndt GA: Delayed gastric emptying after palliative gastrojejunostomy for carcinoma of the pancreas. Arcg Surg 1987; 122: 827-829. 8. Smith AC, Dowsett JF, Russell RC et al.: Randomised trial of endoscopic stenting versus surgical bypass in malignant low bileduct obstruction. Lancet 1994; 344: 1655-1660. 9. Doberneck RC, Berndt GA: Delayed gastric emptying after palliative gastrojejunostomy for carcinoma of the pancreas. Arch Surg 1987; 122: 827-829. 10. Lesurtel M, Dehni N, Tiret E et al.: Palliative surgery for unresectable pancreatic and periampullary cancer: a reappraisal. J Gastrointest Surg 2006; 10(2): 286-291. 11. Horstmann O, Kley CW, Post S, Becker H: Cross-section gastroenterostomy in patients with irresectable periampullary carcinoma. HPB (Oxford) 2001; 3: 157-163.