*Jakub Noskiewicz1, Bartłomiej Kopaczewski2, Małgorzata Rzanny-Owczarzak1, Krzysztof Jarmusz2, Barbara Kocąb1, Przemysław Mańkowski1
Intestinal perforation caused by ventriculoperitoneal shunt
Perforacja jelita spowodowana przez dren otrzewnowy układu zastawkowego
1Department of Paediatric Surgery, Traumatology and Urology, Poznań University of Medical Sciences
Head of Department: Professor Przemysław Mańkowski, MD, PhD
2Section of Paediatric Neurosurgery, Karol Jonscher University Hospital in Poznań
Head of Section: Bartłomiej Kopaczewski, MD, PhD
Streszczenie
Wytworzenie przecieku komorowo-otrzewnowego jest jedną z najczęściej wykonywanych procedur w neurochirurgii dziecięcej. Pomimo że procedurę tę przeprowadza każdy neurochirurg i uznaje się ją za bezpieczną, może wiązać się ona z pewnymi powikłaniami. Około połowa z nich dotyczy drenu otrzewnowego układu zastawkowego. Samoistne wypadnięcie drenu przez odbyt zdarza się bardzo rzadko.
Czteromiesięczne niemowlę zostało przywiezione do szpitala z powodu samoistnego, bezobjawowego wypadnięcia drenu otrzewnowego układu zastawkowego przez odbyt. Dziecku włączono antybiotykoterapię dożylną i przyjęto je na Oddział Neurochirurgii Dziecięcej. Wdrożono postępowanie zabiegowe składające się z czasowego wyłonienia proksymalnego fragmentu drenu otrzewnowego oraz przezodbytowego wyjęcia części dystalnej drenu. Chłopiec nie wymagał usunięcia całego układu zastawkowego. Nie było też konieczności wykonania laparotomii. Wdrożono czasowe, całkowite żywienie parenteralne. Nie obserwowano żadnych powikłań ze strony przewodu pokarmowego na skutek tak prowadzonego postępowania terapeutycznego. Ostatecznie leczenie zakończono wszczepieniem nowego drenu otrzewnowego.
Summary
Ventriculoperitoneal shunt implantation is one of the most common procedures in paediatric neurosurgery. Although the procedure is used often in general neurosurgical practice and regarded as a safe intervention, it has several usual and unusual complications. About a half of these complications involve the peritoneal catheter. Spontaneous transanal protrusion of ventriculoperitoneal shunt is very rare.
A 4-month-old baby was admitted to hospital due to spontaneous, asymptomatic transanal protrusion of ventriculoperitoneal catheter. The boy was put on intravenous antibiotics and taken to surgery. Treatment consisted of extrusion of the peritoneal catheter through the anus and temporary externalisation of the proximal part of the shunt. The previously implanted valve was preserved. Laparotomy was not necessary. Postoperative parenteral nutrition was used. No gastrointestinal complications were found on postoperative observation. Finally, a new peritoneal catheter was implanted.

Introduction
Ventriculoperitoneal shunt implantation is one of the most common procedures in paediatric neurosurgery. It is used to displace excess cerebrospinal fluid into the peritoneal cavity, which is capable of absorbing it. This shunt is implanted in hydrocephalus or cerebral cyst therapy. Although the procedure is regarded as a safe intervention, it has several usual and unusual complications.
Case report
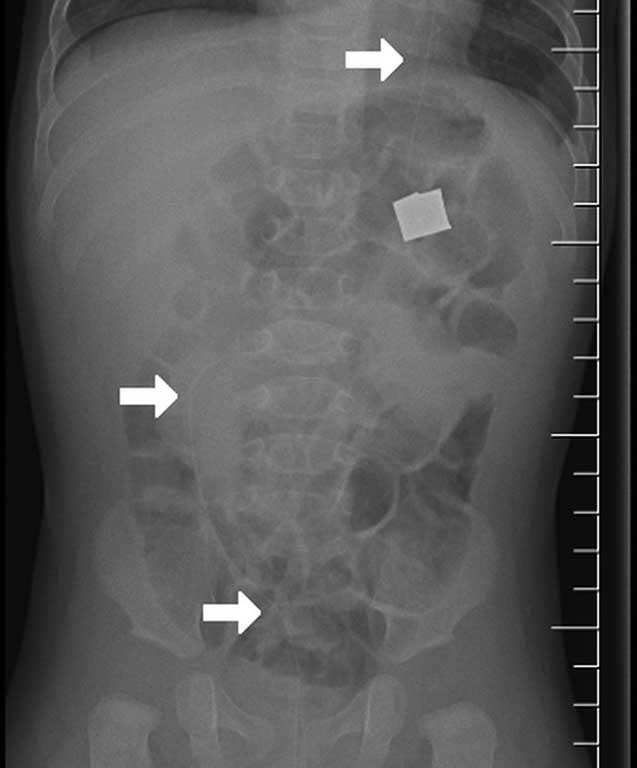
A 4-month-old baby was admitted to hospital due to spontaneous transanal protrusion of a ventriculoperitoneal catheter for the length of 10 cm (fig. 1). The boy was known as a patient with hydrocephalus and multiple cerebral cysts located in the left hemisphere and between hemispheres. Previous treatment involved implantation of ventriculoperitoneal shunt at 1 month after birth. The shunt joined the ventricular system with cysts and the peritoneal cavity. On physical examination on admission, the boy did not have any fever, nausea, vomiting or abdominal pain. The tension of the anterior fontanelle was normal. Abdominal examination did not reveal any significant findings, and peritoneal signs were negative. Abdominal sonography and radiography showed the distal part of the peritoneal catheter within the intestine, but the place of perforation was not found (fig. 2). Furthermore, there was no fluid or free air in the peritoneal cavity. No significant abnormalities were found in laboratory examinations either. The boy was put on intravenous antibiotics (cefuroxime and metronidazole) and taken to surgery. The insertion place of the peritoneal catheter into the intra-abdominal cavity was located subcutaneously, and the catheter was cut. The proximal part of the catheter was taken out from a separate cut on the neck and connected with external drainage. The distal part was extruded through the anus. The previously implanted valve was preserved. Laparotomy was not necessary. Postoperative parenteral nutrition was used. Normal age-adjusted diet was started on the 8th day after operation. No abdominal abnormalities were found on postoperative observation. Finally, a new peritoneal catheter was implanted and connected with the valve.

Fig. 1. Transanal protrusion of the peritoneal catheter of ventriculoperitoneal shunt
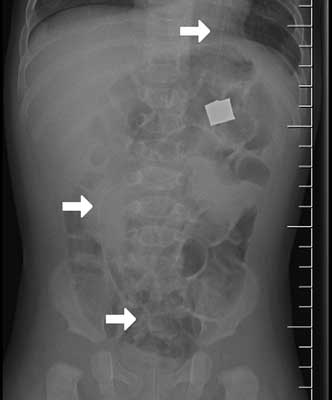
Fig. 2. Abdominal X-ray examination (arrows show the course of the peritoneal catheter)
Discussion
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Borcek AO, Civi S, Golen M et al.: An unusual ventriculoperitoneal shunt complication: spontaneous knot formation. Turkish Neurosurg 2012; 22: 261-264.
2. Sathyanarayana S, Wylen E, Baskaya M et al.: Spontaneous bowel perforation after ventriculoperitoneal shunt surgery: case report and a review of 45 cases. Surg Neurol 2000; 4: 388-396.
3. Mihajlović M, Tasić G, Raicević M et al.: Asymptomatic Perforation of Large Bowel and Urinary Bladder as a Complication of Ventriculoperitoneal Shunt: Report of Two Cases. Srp Arh Celok Lek 2012; 140: 211-215.
4. Berhouma M, Messerer M, Houissa S et al.: Transoral protrusion of a peritoneal catheter: a rare complication of ventriculoperitoneal shunt. Pediatr Neurosurg 2008; 44: 169-171.
5. Hai Al, Rab AZ, Ghani I et al.: Perforation into gut by ventriculoperitoneal shunts: A report of two cases and review of the literature. J Indian Assoc Pediatr Surg 2011; 16: 31-33.
6. Sharifian A, Abdollahi A, Maddah G et al.: Spontaneous transanal protrusion of ventriculoperitoneal catheter: a case report. Acta Med Iran 2013; 51: 135-138.
7. Bodeliwala S, Agrawal A, Mittal A et al.: Transanal protrusion of ventriculoperitoneal shunt via appendicular perforation: A rare case report. J Pediatr Neurosci 2016; 11: 274-266.