*Agnieszka Bruzda-Zwiech1, Natalia Ciesielska2, Joanna Szczepańska1
Conservative management of root-fractured primary incisor – case report
Zachowawcze postępowanie w przypadku złamania korzenia w mlecznym zębie siecznym – opis przypadku
1Department of Paediatric Dentistry, Medical University of Łódź
Head of Department: Professor Joanna Szczepańska, MD, PhD
2Resident, Department of Paediatric Dentistry, Institute of Dentistry, Central Teaching Hospital of the Medical University of Łódź
Head of Department: Professor Joanna Szczepańska, MD, PhD
Streszczenie
Urazy zębów mlecznych dotyczą zazwyczaj struktur podporowych zębów, tj. zwichnięć, natomiast złamania korzeni zębów mlecznych są znacznie rzadszym urazem. Różnica w częstości występowania zwichnięć i złamań korzeni w uzębieniu mlecznym wynika z plastyczności rozwijającej się kości wyrostka zębodołowego i słabszego osadzenia zęba w zębodole. Częstość występowania złamań korzeni wzrasta w wieku 3-4 lat w związku rozpoczęciem resorpcji fizjologicznej korzeni zębów siecznych i osłabieniem wytrzymałości korzenia. Urazowe uszkodzenia zębów mlecznych stanowią szczególny problem stomatologiczny, a ich leczenie często jest odmienne niż urazów zębów stałych. Podczas wyboru metody leczenia należy pamiętać o następstwach urazów zębów mlecznych dla rozwijających się zawiązków zębów stałych i tak dobrać metodę leczenia, aby zminimalizować ryzyko dalszych uszkodzeń stałych następców. W pracy przedstawiono przypadek 3-letniego dziecka po urazie mlecznych siekaczy przyśrodkowych – ekstruzji zęba 51 wymagającej leczenia chirurgicznego i leczonego zachowawczo złamania korzenia zęba 61 w 1/3 wierzchołkowej. Uzyskano pisemną zgodę rodziców/opiekunów prawnych pacjenta na przeprowadzenie badania. Ząb ze złamaniem korzenia pozostawał pod kontrolą kliniczną i radiologiczną przez okres 3,5 roku, do czasu zaawansowanej resorpcji korzenia. Prezentowany przypadek i cytowane przypadki z piśmiennictwa wskazują, że postępowanie zachowawcze jest preferowaną metodą leczenia złamań korzeni zębów mlecznych, które pozwala na utrzymanie zęba po urazie do czasu fizjologicznej resorpcji.
Summary
Most frequent trauma to primary dentitions are injures to the supporting tissue i.e. luxations, but root fractures are relatively uncommon. The difference in the trauma pattern favoring luxation rather than fracture has been found to be typical for the primary dentition, since the elasticity of the alveolar bone surrounding the primary teeth is high and primary tooth held in alveolar socket is less strong. Incidence of foot fractures increases at the age of 3-4 years where physiologic root resorption has begun, thereweakening the root. Traumatic injuries to the primary dentition present special problems and the management is often different as compared with the permanent dentition. Because of potential sequelae of trauma to primary teeth, a treatment method that minimizes any additional risks of further damage to the permanent successors should be selected. The report presents a case of 3.5 year-old boy after traumatic injury – extrusion of tooth 51, which required surgical treatment, and apical third horizontal root fracture of tooth 61 treated conservatively. Written consent from subject’s parents/subject’s legal guardians was obtained. Root-fractured primary tooth has been followed clinically and radiographically for 3.5 year, till advanced root resorption. Presented case and cases described in cited literature demonstrate that conservative treatment of root-fractured primary teeth is a favorable method of the treatment that allows the teeth to function naturally until the term of physiological resorption and exfoliation.

Introduction
In preschool children, head and facial injuries make up 40% of all injuries and oral injuries are covering as much as 18% (1). Andreasen et al. (2) report that one third of 5 year-old children have history of dental trauma, and a large proportion of minor traumatic injuries to deciduous teeth are not reported and not taken into account in the statistics (3). Predominantly deciduous maxillary central incisor teeth are involved, lateral incisors to a less degree and canines (4). The peak prevalence of injures to milk teeth occurs at 2-3 years of age, when motor coordination is still during development, but increased physical activity in children is observed (5). Most frequent trauma to primary dentitions are injures to the supporting tissue i.e. luxations, which account for between 21 and 81% of all dental trauma (3). Multiple luxation injuries and trauma to surrounding soft tissues are mainly reported in children 1-3 years of age and are typically as a result of falls (1). Whereas, isolated root fractures are rare entity among trauma to primary teeth. According to Andreasen and Andreasen (6), in primary dentition 2-4% of dental traumatic injuries were reported as root fractures. Similarly, Walczak et al. study (4) report that root fractures were observed in 2. 46% of dental trauma in children under the age of 6 years. The difference in the trauma pattern favoring luxation rather than fracture has been found to be typical for the primary dentition, since the surrounding bone is less dense and less mineralized and elasticity of the alveolar bone surrounding the primary teeth is high, also primary tooth held in alveolar socket is less strong. This is also due to teeth anatomy as deciduous teeth have shorter crowns than counterpart permanent teeth and roots have smaller sizes (3).
Incidence of foot fractures increases at the age of 3-4 years where physiologic root resorption has begun, thereby weakening the root (7). Root fractures are defined as fractures involving dentin, cementum, and pulp, without or with displacement of coronal fragment of the root. In a clinical examination, the coronal fragment is usually mobile and dislocated, transient pink or gray discoloration of the crown may appear (2, 8). Root fractures in the primary dentition are usually located at mid-root or in the apical third, with radiolucent lines separating the root into two or more fragments (8, 9).
Case report
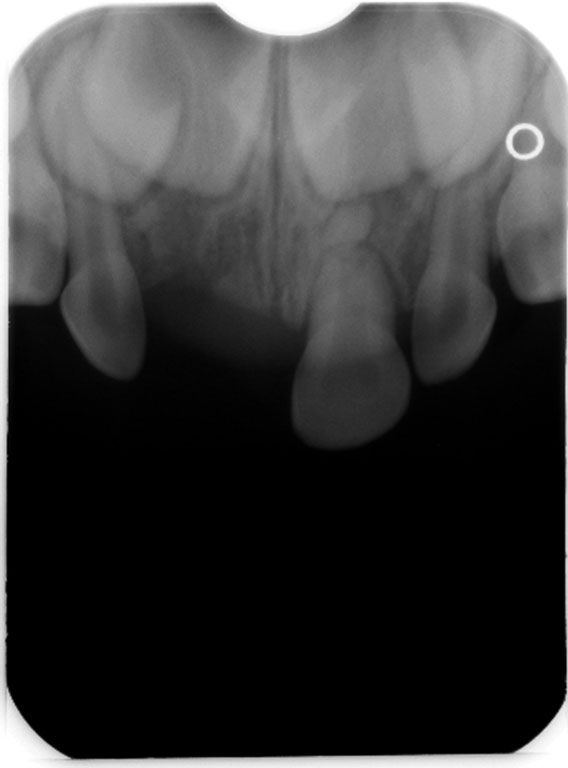
A 3-year-old boy was brought by his mother to the Department of Paediatric Dentistry Medical University of Łódź on 20th November, 2014, complaining of pain and increased mobility of the central incisors in the maxilla following dental injury on the day of reporting. Written consent from subject’s parents/subject’s legal guardians was obtained. The mother of the child reported that the injury was caused by falling to the floor while playing at home. A first aid in the form of stopping of bleeding from the injured upper lip was given immediately after the trauma. Intraoral examination revealed upper lip edema and the presence of a wound of the upper lip, but no suturing was required. In the intraoral examination, hematoma of the alveolar mucosa in the region of primary tooth 51, extrusion and palatally displacement of the tooth were found. The right central maxillary incisor exhibited vertical and horizontal mobility > 2 mm (class III mobility). Also, fracture of the crown, involving enamel, and increased mobility of the left maxillary incisor, 61 were found. Radiographic examination revealed a horizontal fracture on the left central incisor at the apical third of the root, increased periodontal ligament space apically due to severe extrusion of tooth 51 and shortening of the tooth on X-ray due to its palatal displacement (fig. 1). Since severe displacement in the fully formed primary tooth 51, extraction was the treatment of choice, what was in accordance with IADT (The International Association of Dental Traumatology) guidelines for management of traumatic injuries to primary teeth (1).
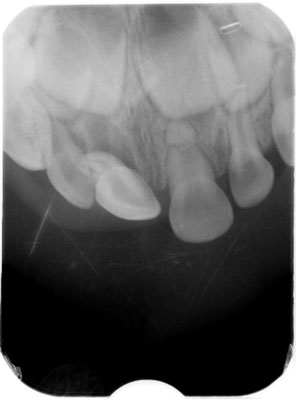
Fig. 1. Initial radiograph of teeth 51 and 61, showing extrusion of tooth 51 and a horizontal root fracture of tooth 61 at the apical third
The patient was referred to the Surgical Department, where the tooth 51 was extracted. Due to the extensive mobility and extrusion, the procedure was performed under topical anesthesia.
A follow-up appointment was set, the patient was instructed to remain on a soft diet for 2 weeks and a gentle brushing with a soft brush was recommended. During the control visit on 24th November, 2014 the tooth mobility was reduced, crown color was normal and there were no changes on alveolar mucosa in the region of tooth 61. The patient’s mother was informed about the need of clinical and radiological follow up. Also, at 8 weeks, the tooth 61 was asymptomatic, physiological mobility and no crown discoloration and normal oral mucosa were noted. Radiographic examination showed resorption on distal surface of apical fragment, rounded margins of coronal fragment of the root, and no evidence of any inflammatory process in the affected tooth (fig. 2). Presence of root fracture healing with calcified tissue was found at the 8 month follow-up (fig. 3).
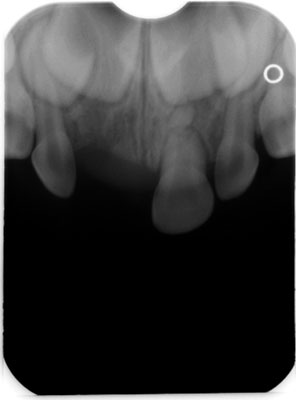
Fig. 2. Periapical radiograph at 8 week follow-up showing atypical resorption of apical fragment, and rounded margins of coronal fragment of the root 61

Fig. 3. Radiograph after 8 months showing presence of root fracture healing with calcified tissue
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Malmgren B, Andreasen JO, Flores MT et al.: International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent Traumatol 2012; 28: 174-182.
2. Andreasen JO, Bakland LK, Flores MT et al.: Traumatic dental injuries – a manual. 3rd ed. Blackwell Munksgaard, Oxford 2011.
3. Jasińska-Piętka J, Pypeć LJ: Urazowe uszkodzenia zębów mlecznych na podstawie piśmiennictwa. Nowa Stomatol 2009; 1-2: 36-39.
4. Walczak M, Turska-Szybka A, Olczak-Kowalczyk D: Przyczyny i rodzaje pourazowych uszkodzeń zębów mlecznych u pacjentów zgłaszających się do leczenia w Zakładzie Stomatologii Dziecięcej Warszawskiego Uniwersytetu Medycznego w latach 2001-2013. Dent Med Probl 2014; 51(4): 498-505.
5. Steciuk A, Emerich K: Urazy zębów – przegląd wytycznych postępowania na podstawie piśmiennictwa oraz opisu przypadków. Ann Acad Med Gedan 2016; 46(1): 65-74.
6. Andreasen JO, Andreasen FM: Essentials of traumatic injuries to the teeth. Munksgaard, Copenhagen 1990.
7. Andreasen FM, Andreasen JO, Cvek M: Root fractures. [In:] Andreasen JO, Andreasen FM, Andersson L (eds.): Textbook and color atlas of traumatic injuries to the teeth. 4th ed. Blackwell Munksgaard, Oxford 2007: 337-367.
8. Kaczmarek U: Diagnostyka i postępowanie lecznicze w uszkodzeniach pourazowych zębów mlecznych według Andreasena. [W:] Olczak-Kowalczyk D, Szczepańska J, Kaczmarek U (red.): Współczesna stomatologia wieku rozwojowego. Wyd. I. Med Tour Press International, Otwock 2017: 569-589.
9. Liu X, Huang J, Bai Y et al.: Conservation of root-fractured primary teeth: report of a case. Dent Traumatol 2013; 29(6): 498-501.
10. Needleman HL: The art and science of managing traumatic injuries to primary teeth. Dent Traumatol 2011; 27: 295-299.
11. Gadicherla P, Devi MM: Root fracture in primary teeth. J Dent Oro Facial Res 2016; 12(1): 33-35.
12. Richa, Kumar N: Management of intra alveolar root fracture in primary incisor: A conservative approach and review of literature. Case Report. J Dent Specialities 2017; 5(2): 156-159.
13. Nam OH, Kim MS, Kim GT, Choi SC: Atypical root resorption following root fractures in primary teeth. Quintessence Int 2017; 48(10): 793-797.
14. Rubel I: Atypical root resorption of maxillary primary central incisors due to digital sucking: a report of 82 cases. ASDC J Dent Child 1986; 53: 201-204.
15. Holan G, Yodko E, Sheinvald-Shusterman K: The association between traumatic dental injuries and atypical external root resorption in maxillary primary incisors. Dent Traumatol 2015; 31: 35-41.
16. Mortelliti GM, Needleman HL: Risk factors associated with atypical root resorption of the maxillary primary central incisors. Pediatr Dent 1991; 13(5): 273-277.