*Andrzej W. Szawłowski
The use of the large bowel for reconstruction of other organs**
Wykorzystanie jelita grubego do rekonstrukcji innych narządów**
Klinika Chirurgii Szpitala MEDICOVER, Warszawa
Streszczenie
W artykule przedstawiono możliwości wykorzystania jelita grubego do odtworzenia ciągłości przewodu pokarmowego po resekcjach innych niż resekcje jelita grubego i wykorzystanie jelita grubego do wytworzenia substytutu narządu po jego wycięciu lub z powodu jego braku. Praktyka kliniczna wykazała, że różne odcinki jelita grubego, poza odbytnicą, czyli okrężnica, mogą być dobrym przeszczepem do odtworzenia ciągłości przewodu pokarmowego głównie po resekcji przełyku, w mniejszym stopniu po resekcji żołądka (gastrektomia) i w przypadku operacji paliatywnych jako zespolenia omijające w nowotworach przełyku. Jako substytut narządu okrężnica może być wykorzystywana głównie w urologii przy rekonstrukcji pęcherza moczowego po jego wycięciu (cystektomia) i w ginekologii przy rekonstrukcji pochwy. Decyzja, który z odcinków okrężnicy może być wykorzystany jako przeszczep do odtworzenia ciągłości przewodu pokarmowego lub jako substytut pęcherza moczowego albo pochwy, zapada śródoperacyjnie i zależy od jakości ukrwienia poszczególnych odcinków okrężnicy przez tętnicę krezkową górną i dolną oraz dobrze wykształconego naczyniowego łuku Riolana, a w drugiej kolejności od długości poszczególnych odcinków okrężnicy. Najczęściej wykorzystywanym odcinkiem jelita grubego do odtworzenia ciągłości przewodu pokarmowego lub jako substytut pęcherza moczowego jest prawa połowa okrężnicy, zaś jako substytut pochwy – esica.
Summary
The paper presents the possibilities of using the large intestine to restore the continuity of the gastrointestinal tract after resections other than large bowel resections and to produce a substitute for a resected or missing organ. Clinical practice has shown that various segments of the large intestine, excluding the rectum, i.e. the colon, can be a good transplant to restore the continuity of the gastrointestinal tract, mainly after oesophagectomy, but also, though to a lesser extent, after gastrectomy, as well as in palliative surgeries as bypass anastomoses in oesophageal cancer. As a substitute, the colon can be used mainly in urology for the reconstruction of the urinary bladder after cystectomy and as a vaginal substitute in gynaecology. The decision which colonic segment can be used as a graft to restore gastrointestinal continuity or as a substitute for the urinary bladder or vagina is made intraoperatively and depends on the quality of blood supply to individual colonic segments through the superior and inferior mesenteric arteries and the well-developed arc of Riolan, as well as on the length of each segment of the colon. The right half of the colon is most commonly used to restore the gastrointestinal continuity or as a urinary bladder substitute, whereas the sigmoid colon is usually used for vaginal replacement.
Key words: large intestine, gastrointestinal continuity restoration, bladder/vaginal substitute

Introduction
Large bowel (colorectal) surgery is mainly used in cancer (a growing epidemiological problem in Poland), inflammatory disorders (e.g. Crohn’s disease, ulcerative colitis, diverticulitis of the large intestine) and, to a lesser extent, developmental disorders (e.g. Hirschsprung’s disease), but also in emergencies associated with abdominal trauma. In selected cases, the large intestine can be used for the reconstruction of other organs, taking advantage of its length (average: 1.5 meters, width: approx. 7.5 cm) as well as the quality of its blood supply, mainly arterial. Table 1 shows the anatomical division of the large intestine, including the length of its individual segments. Figures 1-3 show its arterial blood supply (1).
Tab. 1. Anatomical division of the large bowel
| Anatomical segment | Mean length (cm) |
| Caecum with appendix (appendix vermiformis) | 10 |
| Ascending colon | 15 |
| Transverse colon | 45 |
| Descending colon | 20 |
| Sigmoid colon | 38 (range: 13-60 cm) |
Rectum1:
– lower rectum: up to 5-7 cm
– middle rectum: 7-12 cm
– upper rectum: from 12-18 cm | 18 |
1Division based on endoscopic assessment (rectoscopy) from the anal verge
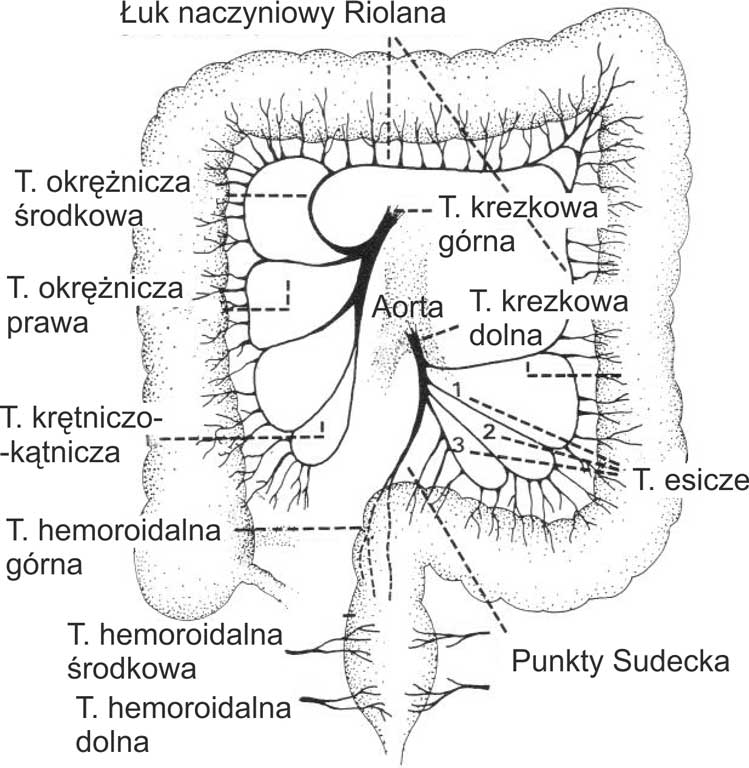
Figure 1 shows the vascular anatomy of the large intestine, which is of key importance in colorectal resection and when planning the use of this organ for the reconstruction of other organs. The large bowel is supplied by two main vascular trunks: the superior mesenteric artery (SMA), which supplies the right half of the large intestine (including the proximal 2/3 of the transverse colon), and the inferior mesenteric artery (IMA), which supplies the left half of the colon (including the distal 1/3 of the transverse colon). Both these vascular trunks arise from the abdominal aorta at different levels. The rectum is supplied by the middle and inferior rectal arteries, on the right and left side, respectively, branching from the internal iliac artery, and the superior rectal artery branching from the inferior mesenteric artery.
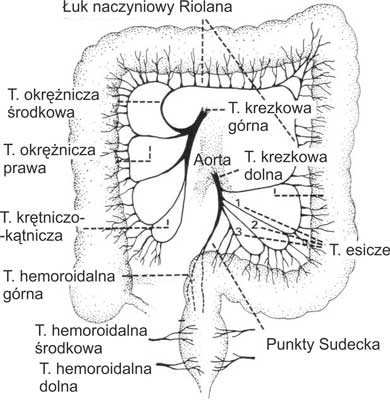
Fig. 1. Arterial supply of the large bowel
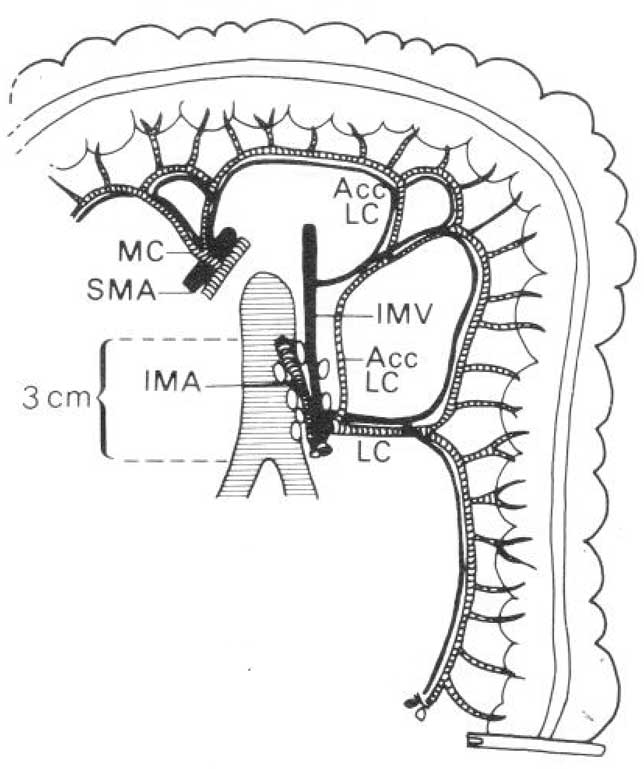
Figure 2 shows the inferior mesenteric vascular system. Its main trunk is approximately 3 cm long from the origin of the abdominal aorta to the origin of the left colic artery. Along its course there are the so-called main lymph nodes, which should be removed during anterior rectal resection in rectal cancer. The main trunk of the inferior mesenteric artery may be spared during large bowel resection due to inflammatory diseases (e.g. inflammatory tumour of the sigmoid colon in the course of diverticulitis), or must be spared when the left half of the colon is intended for use as a substitute to restore gastrointestinal (GI) continuity after oesophageal resection. In the latter case, the quality of blood supply to the graft created from the left half of the colon depends on the ascending branch of the left colic artery and the arc of Riolan extending to the right towards the marginal artery, which runs parallel to the mesenteric edge of the descending colon. This arc connects the superior and inferior mesenteric arteries.
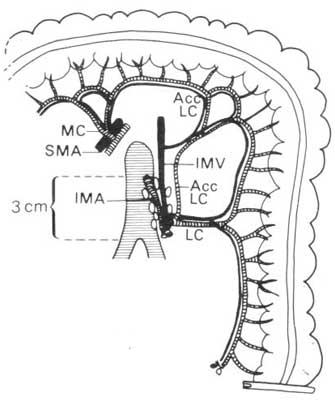
Fig. 2. Large bowel: vascular system of IMA – blood circulation after ligation of IMA with spared left colic artery
IMA – inferior mesenteric artery; SMA – superior mesenteric artery; MCA – middle colic artery; LCA – left colic artery; AscLCA – ascending branch of the left colic artery; IMV – inferior mesenteric vein
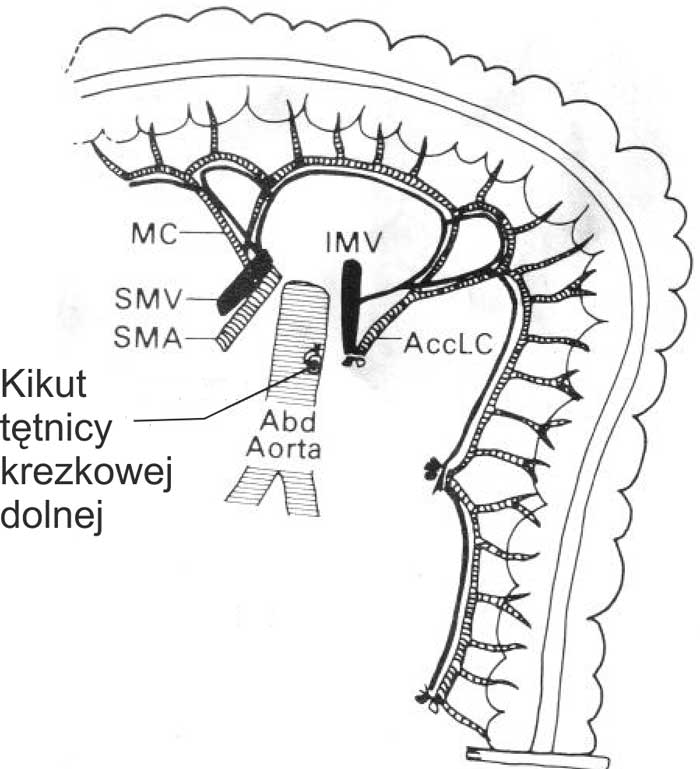
Figure 3 shows the vascular system in the case of high ligation of IMA at its origin from the abdominal aorta. Here, the left half of the colon is supplied by SMA via the arc of Riolan, mainly through the middle colic artery. This variant of high IMA ligation is used when planning to use the left half of the large intestine to restore GI continuity, e.g. after oesophagectomy.
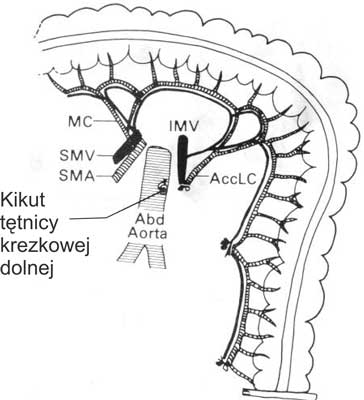
Fig. 3. Large bowel: vascular system of IMA – blood circulation after high ligation of IMA at its origin from the abdominal aorta
Abd. aorta – abdominal aorta; SMA – superior mesenteric artery; SMV – superior mesenteric vein; MCA – middle colic artery; IMV – inferior mesenteric vein; AscLCA – ascending branch of the left colic artery
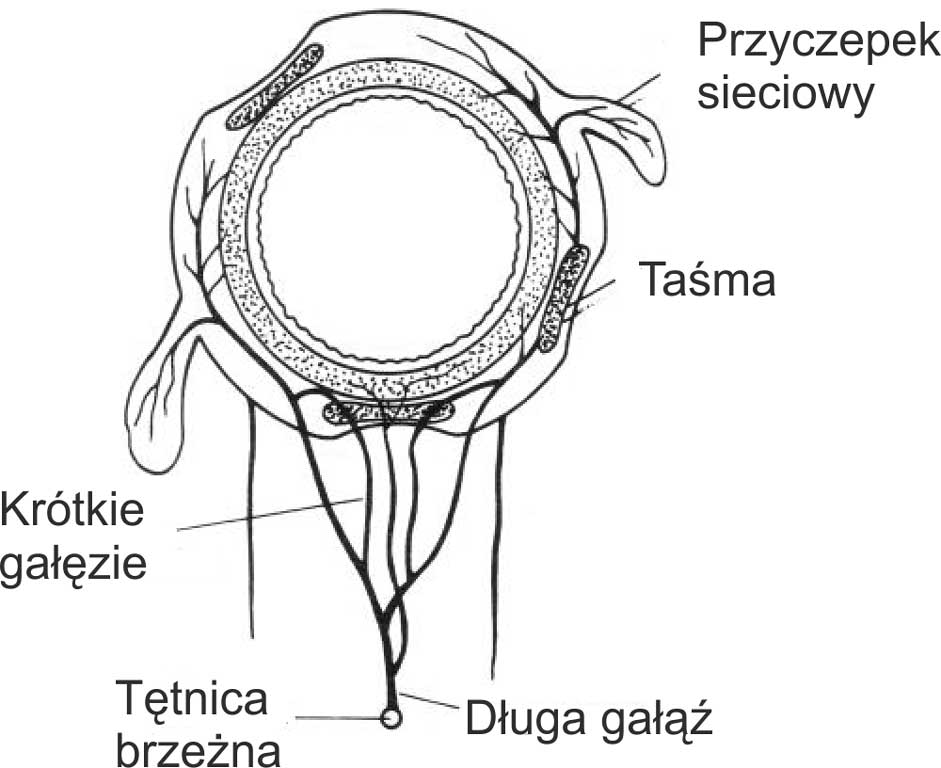
Sparing resection of the omental appendices to clear the intestinal wall is an important detail in order not to disturb the local blood supply to the large bowel wall. If the omental appendage is ligated too close to the intestinal wall, then the short branches arising from the long branches in the intestinal mesentery, and those arising from the marginal artery are simultaneously ligated, which may cause local ischemia of the anastomosed large bowel wall, resulting in anastomotic leakage. The vascular network of the marginal artery and its impact on blood supply to the large bowel wall are shown in figure 4.
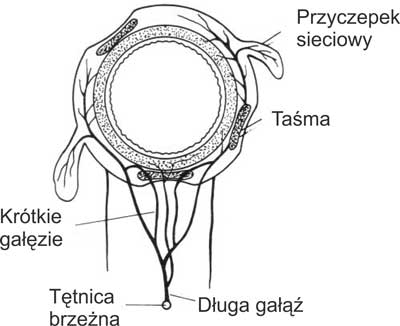
Fig. 4. Vascular anatomy of the large bowel wall
Possible uses of the large bowel for reconstruction of other organs
The use of large bowel for GI continuity restoration after non-large-bowel resections
Restorations of GI continuity after resections other than those of the large intestine mainly use large bowel for oesophageal resections (subtotal oesophgectomy/pharyngo-laryngo-oesophagectomy), when the preferred organ for oesophageal reconstruction, i.e. the stomach, cannot be used (e.g. after previous partial or total gastrectomy). Figures 5-12 show different variants of the use of the large intestine depending on the quality of blood supply to its individual segments (well-developed arc of Riolan in particular) and the length of the intestinal graft needed to perform a tension-free anastomosis. Methods involving the use of the large bowel for bypass anastomoses in palliative (decompressive) surgeries in unresectable oesophageal cancer are presented in figure 13.
The decision as to what part of the large intestine will be used to reconstruct GI continuity after oesophagectomy and/or gastrectomy is made intraoperatively and depends primarily on the quality of blood supply to the section of the large intestine intended for use, with particular emphasis on the quality of the arc of Riolan and the length of individual large bowel segments, which show interindividual variation. The right half of the colon is most frequently used, followed by the transverse colon and the left half of the colon.
The use of the large bowel for oesophageal reconstruction (1-4)
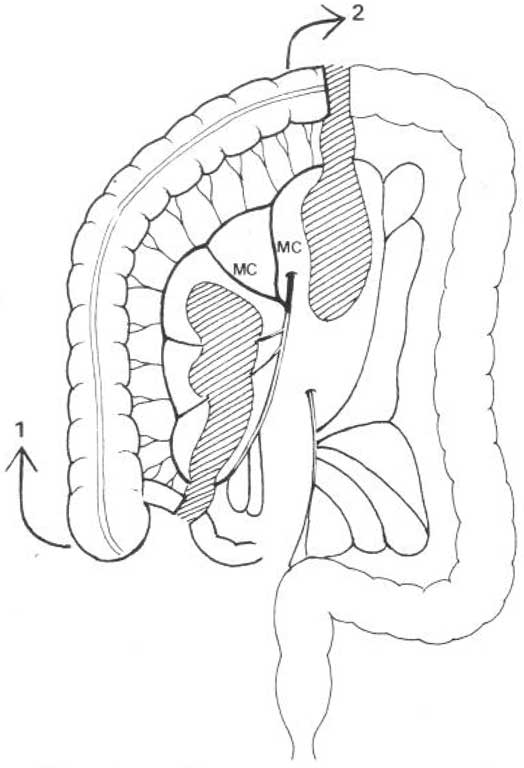
Figure 5 shows the isoperistaltic variant using the right half of the colon with the Bauhin’s valve and approximately 5 cm of the terminal ileum. In this variant, the graft is supplied by SMA via the middle colic artery. The following arteries are ligated: ileocolic and right colic as well as the marginal arteries of the arc of Riolan at the intersection of the transverse colon in front of the splenic flexure of the colon. GI continuity is restored by anastomosing the end of the cervical oesophageal stump on the left side of the neck to the antimesenteric side of the ileum (end-to-side oesophagoileostomy) – the free end of the ileum is closed with an invagination suture to maintain a distance of approximately 2 cm from the oesophageal anastomosis. The transverse colon of the graft is anastomosed either to the anterior wall of the stomach (anterior cologastrostomy) or antecolonically to the first loop of the jejunum (fig. 11) with Braun’s interloop anastomosis (end-to-side antecolic colojejunostomy, side-to-side Braun’s enteroenterostomy) in cases of extending the resection procedure to include gastrectomy. This variant of restoring GI continuity is not used after pharyngo-laryngo-oesophagectomy.
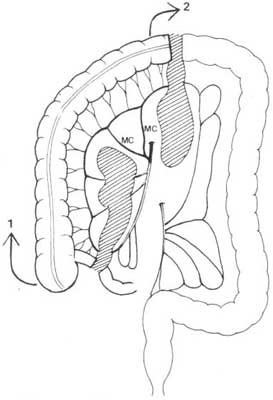
Fig. 5. The use of the right half of the colon to restore GI continuity after oesophageal resection (subtotal oesophagectomy): 1 – segment for anastomosis with the cervical oesophagus after subtotal oesophagectomy (end-to-side oesophago-ileostomy); 2 – segment for anastomosis to the stomach or the jejunum loop
MMA – middle mesenteric artery
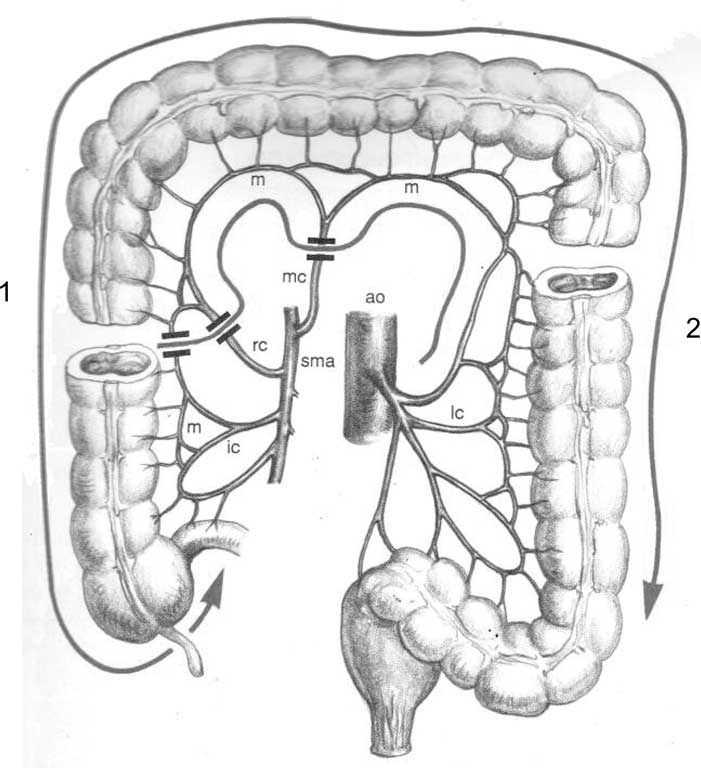
Figure 6 shows the isoperistaltic variant of the use of the transverse colon, provided that the loop of the transverse colon is long, which varies individually. This requires the release of virtually the entire colon from the caecum to the sigmoid colon, with release of both hepatic and splenic flexures of the colon, respectively. The right and middle colic arteries are ligated, thus the graft is supplied by IMA via the ascending branch of left colic artery (ramus ascendens arteriae colicae sinistrae). GI continuity is restored by an anastomosis of the cervical oesophageal stump in the case of subtotal oesophagectomy (end-to-side oesophagocolostomy) or with the laryngeal part of the pharynx (pharyngocolostomy) in the case of pharyngo-laryngo-oesophagectomy to the antimesenteric side of the colon approximately 2 cm from the invaginating suture-closed free proximal end of the colon (fig. 11). The distal end of the colon (descending colon) is anastomosed to the anterior wall of the stomach or antecolically to the first loop of the jejunum (fig. 11), with an additional interloop Braun’s anastomosis if resection is extended to include gastrectomy.
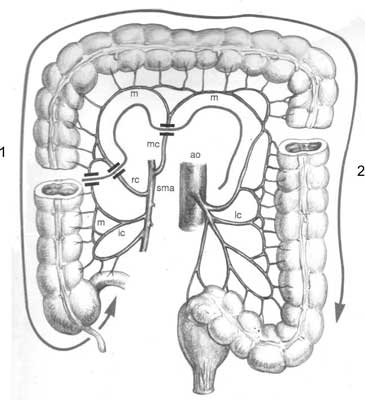
Fig. 6. The use of the transverse colon to restore GI continuity after subtotal oesophagectomy/pharyngo-laryngo-esophagectomy: 1 – segment for anastomosis with the cervical oesophagus after subtotal esophagectomy or with the laryngeal part of the pharynx after pharyngo-laryngo-esophagectomy; 2 – segment for anastomosis with the stomach or jejunum loop
ICA – ileocecal artery; MA – marginal artery; RCA – right colic artery; MCA – middle colic artery; SMA – superior mesenteric artery; LCA – left colic artery; AO – aorta
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Goligher J: Surgery of the anus, rectum and colon. Wyd. V. Wyd. Balliere Tindal, Londyn, Wielka Brytania 1984.
2. Akiyama H: Surgery for Cancer of the Esophagus. Wyd. Williams & Wilkins, Baltimore, USA, 1999.
3. Szawłowski AW, Richter P: Nowotwory układu pokarmowego, otrzewnej i śledziony. [W:] Szawłowski AW, Richter P (red.): Słownik onkologiczny – Mianownictwo stosowane w dyscyplinach onkologicznych z objaśnieniami. Wyd. Wydawnictwo Lekarskie PZWL, Warszawa 2023 (w druku).
4. Szawłowski AW: Nowotwory przełyku. [W:] Jeziorski A, Szawłowski AW, Towpik E (red.): Chirurgia onkologiczna. PZWL, Warszawa 2009, tom 4: 1007-1034.