© Borgis - New Medicine 3/2011, s. 99-102
*Aranka Kovács1, Csilla Nagy2, Attila Juhász2, Zoltán Papp3
Territorial inequalities in premature mortality in Józsefváros (district VIII. of Capital City Budapest), 2006-2008 (level of blocks of flat)
1Semmelweis Egyetem Egészségtudományi Kar Egészségfejlesztési és Klinikai Módszertani Intézet Epidemiológiai Tanszék Budapest
Head of the Department: Dr. Domján Gyula CSs
2Budapest Főváros Kormányhivatala Népegészségügyi Szakigazgatási Szerve
Director: Dr. Zsuzsanna Homor MD
3Heves megye Kormányhivatala Népegészségügyi Szakigazgatási Szerve
Director: Dr. Róbert Vernigg MD
Summary
Background: It is well known that the state of health of the population in Józsefváros is extremely bad. The literature already mentioned in the mid-80′s that the average life expectancy at birth in Józsefváros was 12 years less than in District XII, on the right bank of Danube. Unfortunately, the situation today is still similar, but the district is not homogeneous at all: the state of health of inhabitant groups with different historical and socio-economic background within the district differs at least as much from each other as the indicators of the whole district VIII differ from the capital′s typical results.
Method: In our study we used the Rapid Inquire Facility and for the cluster analysis we used the SatScan program. We reviewed the demographic data of district′s VIII population and – using Standardised Mortality Ratio – the mortality rate of the population aged 30-69 between 2006 and 2008. The effects of the well-known distorting factor (the large number of deaths, homeless shelters in certain areas and among the residents registered at the same address) were eliminated from the study.
Results: The results of the analysis performed by residential quarters showed a significant 1.5 fold excess mortality in Magdolna, Szigony and Orczy quarters compared to the rate of the entire city of Budapest. The significantly high mortality rates in the blocks of Magdolna and Orczy quarters were confirmed by the inspection on the level of blocks and by the results of cluster analysis as well.
Conclusions: The results of this study clearly define areas with a high death-risk in district VIII, even on the level of blocks, which constitutes a targeted information to the local decision-makers for developing a health promotion plan in order to reduce the existing disparities.
Introduction
In the mid-70′s, the average life expectancy at birth (LEB) in Hungarian population was of few years less compared to many European countries (1), and the increase rate of this indicator has not reached that of other European countries during the past 20 years. In 2005 Hungary′s LEB indicator was 7 years less compared to that of the old member countries of the European Union, and what is sadder, there are still significant differences within the countries (2). The highest level of LEB among men (70,5 years) was noted in Budapest, the worst was observed in Borsod-Abaúj-Zemplén County (66.03 years), giving the difference of more than 4 years. Budapest is in the best place regarding LEB if we consider it as a whole. Using higher territorial resolution outlines the differences in LEB indicators, and the district in the centre of Budapest, with great historical and architectural values, Józsefváros has a worse LEB than the counties with the worst LEB in the country. This district gives home not only for a memorial place of historic turning points, but also for health care and higher education institutions – the medical university of the capital among others – and is also centre of transportation and cultural institutions (4). The LEB and other indicators of health status show however that people of most disadvantageous situation live in the District VIII (4-5). Thus the study was designed to analyze the death rates in the historical quarters of Józsefváros.
Methods
In this descriptive epidemiological study we investigated premature mortality data (age group 20-59 years) between 2006 and 2008 on the level of quarters and blocks. District VIII in Budapest has 11 historical quarters, with an average population of 7950 each, and 185 blocks of flats with average population of 400 each.
Data
Mortality and population data for the years 2006-2008 in 10-year age bands were obtained from the National Institute of Environmental Health. The data was originally derived from the Hungarian Central Statistical Office.
Disease mapping
The disease mapping was carried out using the Rapid Inquiry Facility (RIF 3.12) software (6). Using the disease mapping option within the RIF, territorial patterns of premature mortality in District VIII of Budapest were investigated in both quarter and block levels.
Indirectly standardized (standard: age-specific death rates of population of Budapest) and smoothed relative risks (Smoothed Relative Risk) were calculated using full hierarchical Bayesian methods. The WinBUGS (7) smoothing algorithm was linked directly to RIF.
The BYM model employed by RIF takes into account both the heterogeneity effect (smoothing toward the capital mean) and the territorial autocorrelation component (smoothing toward the local mean) (8). Uncertainty is shown by the posterior probability of an excess risk for areas where the residual risk was above 1 and the posterior probabilities were greater than 0.8 (9).
Cluster detection
Areas with high, age-adjusted death rate (clusters) were defined with scan statistics (10, 11). The SatScan algorithm was also linked directly to RIF. Elliptical window shape was used and the maximum spatial cluster size was 15% of the population at risk.
Results
The study carried out in Budapest, Hungary, in an internal district, called Józsefváros where there are approx. 80 thousand inhabitants and it is well known that the people living here are in very poor health condition, as it has been indicated by the high rate of premature mortality for years (12, 13).
The district is situated in the centre of the capital with a population of two million, in the middle of the left bank of the Danube River. The district is a traffic hub, and is in a close vicinity of the capital′s downtown rich in beauty and pride.
The district as a whole, belongs to the most densely populated parts of the capital, at the same time the majority of the quarters – except for Józsefváros Centre and Palace quarter – were sparsely populated compared to the whole District VIII (table 1).
Table 1. Density of population in Districts of Budapest and in quarters of District VIII.
| District/Quarter | Density of population (person/km2) |
| District I | 7599,4 |
| District II | 2546,0 |
| District III | 3315,8 |
| District IV | 5499,0 |
| District V | 11176,8 |
| District VI | 18545,0 |
| District VII | 30687,6 |
| District VIII | 11939,0 |
| District IX | 5027,5 |
| District X | 2487,8 |
| District XI | 4315,5 |
| District XII | 2315,8 |
| District XIII | 8508,4 |
| District XIV | 6812,5 |
| District XV | 3162,6 |
| District XVI | 2119, |
| District XVII | 1458,9 |
| District XVIII | 2495,5 |
| District XIX | 6802,8 |
| District XX | 5360,8 |
| District XXI | 3144,9 |
| District XXII | 1534,2 |
| District XXIII | 507,5 |
| VIII. /Kerepesi | 1347,7 |
| VIII. /Százados út | 1759,3 |
| VIII. /Ganz | 3270,0 |
| VIII. /Szigony | 10386,9 |
| VIII. /Orczy | 14569,7 |
| VIII. /Tisztviselőtelep | 18194,5 |
| VIII. /Népszínház | 20028,5 |
| VIII. /Palota | 22116,1 |
| VIII. /Józsefváros központ | 27181,6 |
| VIII. /Csarnok | 32151,2 |
| VIII. /Magdolna | 36025,4 |
Compared to the average of Budapest, a significantly higher death rate was observed in certain Józsefváros quarters, Magdolna, Szigony, and Orczy quarters and in the centre of the district (fig. 1). In these quarters there was a significant excess of mortality by about 1.5 fold of the Budapest average (table 1).
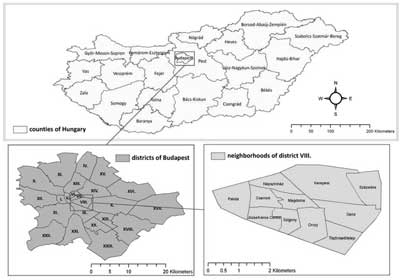
Figure 1. Administrative units in Hungary and in its capital, Budapest.
Our results show that also on the level of blocks a flats, areas with high mortality-risk could be observed in Magdolna, Szigony and Orczy quarters (fig. 2A).
Contiguously high risk of death characterized the middle two thirds of the Magdolna quarter, and some areas neighbouring the Magdolna quarter in the Szigony and the Orczy quarter (fig. 2.).
The results of the cluster analysis determined even more clearly the blocks of Magdolna and Orczy quarter as high death-risk areas during the study period (fig. 2B.)
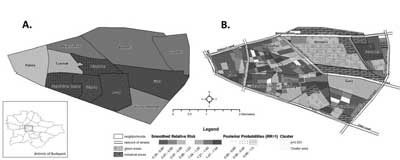
Figure 2. Territorial distribution of premature (20-59 years) mortality in District VIII of Budapest. A.: on the level of quarters B.: on the level blocks of flats
Discussion
Our results show that the death rate is extremely poor in the middle part of the District VIII, which is the cause of extremely unfavourable premature mortality indicators in Józsefváros (District VIII) (12-13).
In other words, the result found in the middle part affects the district level analyses and the results published in similar studies about Józsefváros of a whole grater part of Józsefváros indicate that the district′s citizen is in a more „favourable” situation than the average citizen of the capital (2-5, 12-13). In earlier studies in the District VIII district population, the high early-death indicators were accompanied with negative socio-economic characteristics (5). Worthy of note is the social change among the most disadvantaged people in Magdolna quarter. Former residents of the internal part of Józsefváros (such as Magdolna quarter) – Gypsy musicians, many of them being the famous artists, member of famous bands and also musical instrument makers, could keep very large families. However, at the end of 20th century the demand for gypsy music declined and they could not get work either in our country or abroad. The population without a future was unable to change, got older, and people who came from the country in socially appalling condition, seeking a better living, moved into the divided civilised homes of the failing ”native” residents. The state of the run-down homes continued to deteriorate, and many of them are now occupied by squatters. The area has two railway stations and is located in the heart of Budapest, probably with the largest through traffic, which also helped the influx of groups of people who wanted to try their luck (2).
Conclusions
As a consequence, the homeless services were best developed in this area in the last decade. The area has four institutions, which provide homeless social services, from low budget social care, through health care to the residential social institutions (2). Moreover, this area was also affected by the fact – which distorted the whole District′s VIII population mortality indicators – that homeless people had to have a reported address to get income, employment, pensions, disability pensions, social assistance. In 2010, there was a block of flats, in which the reported number of people living there was so high that there wouldn′t be enough room for them even if standing fit (2).
This social stratum has a lifestyle, which has disproportionately increased the risk of early mortality, and our cluster analysis on block level has demonstrated the distorting differences.
It is to be regretted that people registered at the building blocks of District VIII – wherever they really live on grounds of their registered addresses, distort the characteristics of the area, and worsen the unfavourable premature death rates of the inhabitants of the eighth district.
Piśmiennictwo
1. European health for all database (HFA-DB) World Health Organization Regional Office for Europe Updated: Jan 2011 http://data.euro.who.int/hfadb/ (Accessed: 2011.02.28.). 2. Csite A, Nemeth N: A születéskor várható élettartam kistérségi egyenlőtlenségei az ezredforduló Magyarországán Kormányzás, Közpénzügyek, Szabályozás II, 2007; 2, 257-289. 3. Uzzoli A-Szilágyi D: Life expectancy and its regional inequalities in Hungary. Geographica Pannonica 2009/4. pp. 127-136. (ISSN 0354-8724) (ISSN 1820-7138). 4. Juhász A, Nagy Cs: Public Health Report for policy makers, 2009. Central Hungarian Regional Institute of Public Health and Medical Officer′ Service′s, 2010. 5. Kovács A, Juhász A, Nagy Cs: A lakosság korai halálozási viszonyai, valamint néhány társadalmigazdasági tényező által meghatározott egyenlőtlenség a Józsefváros negyedeiben élő népesség körében, 2001-2007. Egészségtudomány, LIII. 2009. 2. 6. Beale L, Hodgson S, Abellan JJ et al.: Evaluation of Spatial Relationships between Health and the Environment: The Rapid Inquiry Facility. Environ Health Perspect 2010; 118: 1306-1312. 7. Lunn DJ, Thomas A, Best N et al.: WinBUGS – a Bayesian modelling framework: concepts, structure, and extensibility. Stat Comput 2000; 10: 325-337. 8. Besag J, York J, Mollié A: A Bayesian image restoration with two applications in spatial statistics. Ann Inst Stat Math 1991; 43: 1-59. 9. Richardson S, Thomson A, Best N et al.: Interpreting posterior relative risk estimates in disease-mapping studies. Environ Health Perspect 2004; 112: 1016-1025. 10. Kulldorff M, Nagarwalla N: Spatial disease clusters: detection and inference. Stat Med 1995; 14: 799-810. 11. Kulldorff M and Information Management Services, Inc. SaTScanTM v7.0: Software for the spatial and space-time scan statistics. http://www.satscan.org/, 2006. 12. Józan P: A budapesti halandósági különbségek ökológiai vizsgálata 1980-1983. Demográfia 1986; 29: 193-240. 13. Klinger A: A budapesti kerületek halandósági különbségei. Demográfia 2003; 46: 9-44.
