© Borgis - Postępy Nauk Medycznych 6/2013, s. 396-399
*Filip Kucharczyk, Waldemar Rylski, Rafał Kamiński, Stanisław Pomianowski
Destabilizacja śródszpikowego zespolenia gwoździem Gamma złamań przezkrętarzowych z migracją śruby doszyjkowej do stawu biodrowego
Destabilization of intramedullary fixation with Gamma nail for intertrochanteric fractures with sliding screw cut out
Department of Orthopaedics and Traumatology, The Medical Centre of Postgraduate Education, prof. Adam Gruca Hospital, Otwock
Head of Department: prof. Stanisław Pomianowski, MD, PhD
Streszczenie
Wstęp. Złamania przezkrętarzowe są złamaniami bliższego końca kości udowej, lokalizują się pozatorebkowo, sięgając do 5 centymetrów poniżej krętarza mniejszego (3). W naszej Klinice od wielu lat stosujemy niemalże wyłącznie technikę osteosyntezy śródszpikowej przy zaopatrywaniu tego typu złamań. Najczęstsze mechaniczne powikłanie dla zespolenia śródszpikowego metodą gwoździa Gamma to destabilizacja zespolenia z migracją śruby doszyjkowej poza głowę kości udowej z towarzyszącym przemieszczeniem odłamów i szpotawą deformacją (4). Najczęstsze powody destabilizacji zespolenia to: niestabilny typ złamania, nieanatomiczne nastawienie złamania, nieprawidłowa pozycja śruby doszyjkowej (4, 6).
Cel pracy. Celem pracy jest udowodnienie związku pomiędzy destabilizacją gwoździa gamma z migracją śruby doszyjkowej a błędami w technice operacyjnej.
Materiał i metody. Praca obejmuje 842 chorych, którzy zostali przyjęci z rozpoznaniem złamania przezkrętarzowego w latach 2008-2012 oraz zaopatrzeni metodą osteosyntezy śródszpikowej. Chorzy ze złamaniem przezkrętarzowym operowani są najczęściej we wczesnych dobach po przyjęciu do szpitala i postawieniu rozpoznania. Ocena zespolenia prowadzona jest pod kątem: prawidłowego nastawienia złamania, lokalizacji i położenia śruby doszyjkowej w płaszczyźnie AP i osiowej z podziałem głowy kości udowej na 4 części w projekcji AP i 3 części w pozycji osiowej. Migracja śruby definiowana jest jako przemieszczenie jej o więcej niż 1 mm poza obrys głowy kości udowej. W materiale przeanalizowano 842 chorych przyjętych do Kliniki z rozpoznaniem złamania przezkrętarzowego, spośród których 763 poddano zabiegowi operacyjnemu.
Wyniki. Powikłanie polegające na destabilizacji zespolenia z migracją śruby doszyjkowej do stawu biodrowego zaobserwowaliśmy wśród 12 chorych.
Wnioski. Powikłanie zgodnie z doniesieniami spotykanymi w literaturze związane było z: trudnym, wielofragmentowym, niestabilnym charakterem złamania, nieanatomicznym nastawieniem złamania lub nieprawidłowym umieszczeniem śruby doszyjkowej.
Summary
Introduction. Intertrochanteric fractures are located in the proximal upper part of the femur, extracapsulary and extend up to 5 cm under the minor trochanter (3). Intramedullary fixation is used almost exclusively for this kind of fractures in our department for many years. The most common mechanical complication of intramedullary fixation is the cut out of the sliding screw trough the femoral head. The most common reasons for fixation instability are unstable type of fracture, not anatomic fracture reduction and abnormal position of the sliding screw (4, 6). Patients with intertrochanteric fractures are usually operated in the early days of the hospital admission and diagnosis. Cut out of the screw is defined as the displacement of more than 1 mm beyond the contour of the femoral head.
Aim. In our analysis we prove that destabilisation of gamma nail with cut out of sliding screw is caused by technical mistakes made during the surgical procedure.
Material and methods. The analysis includes 763 patients who were operated with intramedullary fixation among 842 patients with a diagnosis of intertrohanteric fracture between 2008-2012.
Results. Complication involving migration of the sliding screw was observed among the 12 patients.
Conclusions. Complication according to literature was associated with: difficult, unstable type of the fracture, non anatomical reduction of the fracture and non-optimal position of the sliding screw.

Introduction
Intertrochanteric fractures are located in the proximal upper part of the femur, extracapsulary and extend up to 5 cm below the minor trochanter (1). Most often they are caused by low energy trauma or tumor metastases in elderly patients. Among young people they are caused by high energy trauma (3). Intramedullary fixation is used almost exclusively for this kind of fractures in our department for many years. The most common mechanical complication of intramedullary fixation is the cut out of the sliding screw trough the femoral head with destabilization of fixation and fracture displacement (4). The most common reasons for fixation instability are unstable type of fracture, not anatomic fracture reduction and abnormal position of the sliding screw with incorrect TAD index (Tip Apex Distance specifying the sum of distances between the apex of the sliding screw and femoral head in AP and axial projection) less than 25 mm (fig. 1) (4, 6).

Fig. 1. TAD determination method.
AIM
In our analysis we prove that destabilisation of gamma nail with cut out of sliding screw is caused by technical mistakes made during the surgical procedure.
Material and methods
The analysis includes 763 patients who were operated with intramedullary fixation among 842 patients with a diagnosis of intertrochanteric fracture between 2008-2012, analysis is based on all available x-ray scans before surgery, after fixation and late control studies which, were taken between 2008-2012.
All fractures are classified with AO classification (fig. 2).
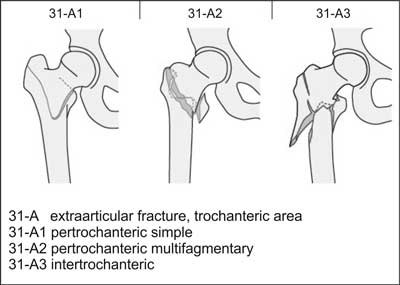
Fig. 2. AO classification (9).
Patients with diagnosed intertrochanteric fracture are operated in firs days after diagnosis. Operations are performed by specialists or residents during specialization, both trained in operation technique. The operation is performed on traction table with fluoroscopic view in spinal or general anesthesia. In most cases procedures are performed after closed reduction, in special situations when closed reduction fails patients undergo open reduction and intramedullary fixation.
Operative treatment allows full weigh bearing on operated limb if the reduction is anatomical and technically correct. In cases of incorrect reduction only partial weigh bearing is allowed until first postoperative visit after 6-8 weeks.
Fixation is assessed in terms of: appropriate and anatomical reduction, sliding screw position in AP and axial x-ray view with division of femoral head into 3 parts in axial view and 4 parts in AP view.
The best positions for sliding screw are central-central or central-inferior positioning of the screw in axial and AP view.
The cut-out effect is defined as migration of screw mare than 1 millimeter outside the femoral head.
Results
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Tylman D, Dziak A: Traumatologia narządu ruchu. Wyd. 2, PZWL, Warszawa 1996; t. 1-2.
2. Canale TS, Beaty JH: Campbell’s Operative Orthopaedics. 11th ed., Philadelphia: Mosby Elsevier 2008; 4311-4344.
3. Bucholz RW, Heckman JD, Court-Brown CM: Rockwood and Green’s Fractures in Adults. 6th ed., Philadelphia: Lippincott Williams & Wilkins 2006; 2147-2247.
4. Bojan AJ, Beimel C, Taglang G et al.: Critical factors in cut-out complication after gamma nail treatment of proximal femoral fractures. BMC Musculoskelet Disord 2013 Jan 2; 14(1): 1.
5. Pascarella R, Cucca G, Maresca A et al.: Methods to avoid gamma nail complications. Chir Organi Mov 2008 Apr; 91(3): 133-139.
6. De Bruijn K, den Hartog D, Tuinebreijer W, Roukema G: Reliability of predictors for screw cutout in intertrochanteric hip fractures. J Bone Joint Surg Am 2012 Jul 18; 94(14): 1266-1272.
7. Andruszkow H, Frink M, Frömke C et al.: Tip apex distance, hip screw placement, and neck shaft angle as potential risk factors for cut-out failure of hip screws after surgical treatment of intertrochanteric fractures. Int Orthop 2012 Nov; 36(11): 2347-2354.
8. Lobo-Escolar A, Joven E, Iglesias D, Herrera A: Predictive factors for cutting-out in femoral intramedullary nailing. Injury 2010 Dec; 41(12): 1312-1326.
9. The Müller AO Classifi cation of Fractures – Long Bones.
