© Borgis - Postępy Nauk Medycznych 6/2013, s. 420-427
*Piotr Zakrzewski, Daniel Kowalski, Andrzej Boszczyk, Mariusz Urban, Marcin Błoński, Stanisław Pomianowski
Złamania bliższego końca kości piszczelowej u chorych w wieku podeszłym
Proximal tibial fractures in elderly patients
Department of Traumatology and Orthopaedics, The Medical Centre of Postgraduate Education, prof. Adam Gruca Hospital, Otwock
Head of Department: prof. Stanisław Pomianowski, MD, PhD
Streszczenie
Złamania bliższego końca kości piszczelowej, jako złamania stawowe kolana, mogą powodować trwałe następstwa w postaci ograniczenia zakresu ruchu, bólów czy wysięków stawu. U ludzi starszych najczęstszą przyczyną złamania jest uraz niskoenergetyczny. Wystarczy upadek z własnej czy niewielkiej wysokości, co przy często osteoporotycznej kości doprowadza do jej złamania. Badania RTG i CT pozwalają określić typ złamania i stopień uszkodzenia tkanki kostnej. Badanie MRI pozwala ocenić stopień uszkodzenia chrząstki stawowej oraz ewentualnie współistniejące uszkodzenia łąkotek i więzadeł stawu kolanowego. Złamania bez przemieszczenia lub z niewielkim przemieszczeniem powinny być leczone zachowawczo, złamania z dużym przemieszczeniem operacyjnie. Leczenie operacyjne powinno dążyć do anatomicznego odtworzenia powierzchni stawowych i tak stabilnego zespolenia odłamów, aby nie było konieczności unieruchomienia starszego pacjenta w opatrunku gipsowym.
Summary
Most proximal tibial fractures involve the articular surface and may lead to permanent consequences as limitation in range of movement, pain and intra-articular effusion. The most common cause of fractures in elderly persons is low-energy injury. In osteoporotic bone, even a fall from a standing position or insignificant height may lead to fracture. X-rays and CT-scans are useful in classifying the type of the fracture and assessing its extent, whereas MRI visualizes chondral lesions and potential concomitant meniscal and ligamentous injuries in the knee joint. Non-displaced or minimally displaced fractures should be treated with immobilization alone, while severely displaced fractures require surgical treatment. The purpose of surgical treatment in elderly patients is to reconstruct the articular surface and perform fixation stable enough to make plaster immobilization redundant.

Introduction
Proximal tibial fractures constitute approximately 7% of lower limb fractures. A vast majority includes fractures involving the articular surface, the so-called tibial plateau. The degree of damage of the articular cartilage surface and the bone tissue is crucial for prognosis. In the case of severe damages, the most frequently in the case of severe damages (ie. split-depression fractures), the injury may lead to rapid development of the degenerative disease of the knee joint – gonarthrosis (1, 2). Obviously, the treatment outcome is affected by the knee condition before the accident, previous problems with the menisci, degree of use of the articular cartilage, existing limitation of movement range, and perhaps past surgeries, which are factors worsening the prognosis.
Diagnosis
In elderly people, a fracture (fig. 1) is frequently caused by a fall as a result of a stumble or injury resulted from a fall from a small height, e.g. from a chair, windowsill, table, etc. Small forces are necessary to create a fracture in weak osteoporotic bone.

Fig. 1. Split depression fracture of the proximal tibia.
Basic components of the fracture include edema of the knee joint, severe pain at pressure and during movement attempt, and frequently valgus deformation of an axis. Puncture of the knee joint reveals the presence of hematoma and frequently, fat droplets. Basic evaluation consists of X-rays in two projections (fig. 2).

Fig. 2. Type IV fracture according to Schatzker criteria. Figures a and b – initial X-ray. Visible fracture of a large fragment of the medial condyle, including the intercondylar eminence. Figure c – X-ray performed after 4 days of functional treatment with supramalleolar skeletal traction. It seems that the normal position of the bone fragments has been achieved.
Evaluation includes fracture type, degree of depression and displacement of the bone fragments as well as the bone quality. However, very often an X-ray image is not sufficient in fracture evaluation and it is not able to support a decision on the treatment method. The most useful evaluation method is computed tomography (CT-scan) and magnetic resonance imaging (MRI) (fig. 3). While computed tomography image, especially 3D, perfectly visualizes the degree of bone fragments depression and displacement, the MRI evaluation is irreplaceable in the evaluation of soft tissue damage, mainly the menisci and the ligaments, which may accompany the fracture (fig. 4).

Fig. 3 a, b, c. CT scan of the fracture seen in radiograms in fig. 2. Performed CT-scan showing secondary reconstruction in the frontal and the sagittal planes and 3D images visualize actual, large displacement of the bone fragments in this fracture and 3-cm depression of the articular surface of the medial condyle of the tibia, which significantly changes qualification for treatment method from conservative to surgical therapy.

Fig. 4. X-ray and MRI images of the same knee joint. MRI undoubtedly shows how serious this injury is and it allows performing its detailed evaluation.
One should remember that just as in the case of the spine, elderly people with advanced osteoporosis may suffer from invisible fractures. The patient reports to the doctor pain in the knee joint lasting for some time, and frequently associated with progressing deformity of the limb axis, but the patient does not remember any injury.
Pathomechanism of the injury
Intra-articular fractures of the proximal tibia occur as a result of not only indirect, but also direct injuries. In elderly patients, there are mainly indirect injuries resulted from a fall on the knee in a slightly valgus position. In general, direct injuries accompany car accidents or result from direct impact on the tibial epiphysis. The important role in the mechanism of fractures is played by the anatomical structure of the femoral and tibial condyles as well as the physiological valgus position of the knee joint. If the force during the injury acts on the lateral surface of the knee joint, the strong and hard femoral condyle crushes and splits the more fragile lateral condyle of the tibia (fig. 5). Damage of the tibial lateral collateral ligament may also occur in such case. If the force comes from the medial direction, the medial femoral condyle, which is also stronger, crushes or splits the more fragile medial condyle of the tibia (fig. 6), and in addition, lateral ligament structures may be damaged. In the case of a fall from a height on an extended limb, the femoral condyles, acting as a ram, may crush and split the tibial condyles (fig. 7). Fracture lines, which are occurring in this case, resemble reversed letters “V”, “T” and “Y”.
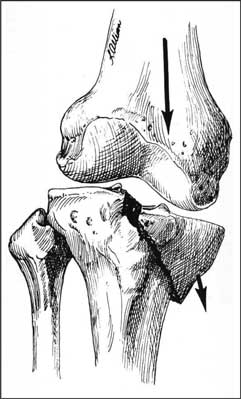
Fig. 5. Injury of the external articular surface, abduction mechanism.
Fig. 6. Injury of the internal articular surface, adduction mechanism.
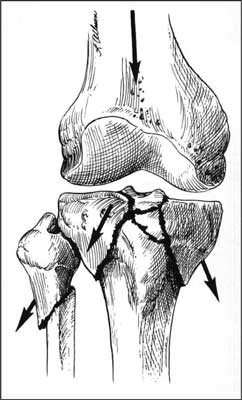
Fig. 7. Injury acting along the limb axis, fall from height.
Pathomechanism of fracture of the lateral tibial condyle according to Trickey, who was one of the pioneers noticing possible coexistence of injuries of the menisci and ligaments (fig. 8):

Fig. 8 a – the lateral tibial condyle, which was broken off, is pressed by the lateral femoral condyle, b – the lateral tibial condyle, which was broken off, is moved by the edge of the lateral femoral condyle (18).
a) tears of the tibial collateral ligament and frequent tears of the anterior cruciate ligament usually occur in both types of fractures,
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Aubriot JH: Post-traumatic knee degeneration. Rev Prat 1998; 15, 48(16): 1799-1804.
2. Stevens DG, Beharry R, McKnee MD et al.: The long-term fuctional outcome of operatively treated tibial plateu fractures. 5: Orthop Trauma 2001 Jun-Jul; 15(5): 312-320.
3. Godde S, Rupp S, Dienst M et al.: Fracture of the proximal tibia six months after Fulkerson osteotomy. A raport of two cases. J Bone Joint Surg Br 2001 Aug; 83(6): 832-833.
4. Kurt C, Tad L, Taskiran E: Tibial plateu fractures following oblique osteotomy of the tibial tubercle: a case report. 1: Acta Orthop Traumatol Turc 2002; 36(4): 362-365; Chir Narz Ruchu Ortop Pol 1975, XL, 1.
5. Stetson WB, Friedman MJ, Fulkerson JP et al.: Fracture of the proximal tibia with immediate weight bearing after a Fulkerson osteotomy. Am J Sports Med 1997 Jul-Aug; 25(4): 570-574.
6. Delcogliano A, Chiossi S, Caporaso A et al.: Tibial plateau fractures after arthroscopic anterior cruciate ligament reconstruction. Arthroscopy 2001 Apr; 17(4): E16.
7. El-Hage ZM, Mohammed A, Griffiths D, Richardson JB: Tibial plateau fracture following allograft anterior cruciate ligament reconstruction. Injury 1998 Jan; 29(1): 73-74.
8. Mueller ME, Allgower M, Schneider R, Willenegger H: Manual of Internal Fixation. Springer-Verlag, Berlin 1979.
9. Schatzker J: The Tibial Plateau Fractures: The Toronto Expirience Clinical Orthop 1979; 138: 94.
10. Honkonen SE: Indication for surgical treatment of tibial condyle Clinical Orthop 1994; 302: 199-205.
11. Lachiewicz P, Funcik T: Factors influencing the results of open reduction and internal fixation of tibial plateau fractures. Clinical Orthop 1990; 254: 210-215.
12. Bennett WF, Browner B: Tibial plateau fractures – a study of associated soft tissue injures. J Orthop Trauma 1994; 8(3): 183-188.
13. Schulak DF, Gunne D: Fractures of Tibial Plateau. A reviev of literarure. Clinical Orthop 1975; 109: 166-177.
14. Attmanspacher W, Dittrich V, Staiger M, Stedtfeld HW: Arthroscopic management of tibial plateu fractures. 1: Zentralbl Chir 2002 Oct; 127(10): 828-836.
15. Jubel A, Andermahr J, Mairhofer J et al.: Use of the injectable bone cement Norian SRS for tibial plateau fractures. Results of a prospective 30-month follow-up study. Orthopade 2004 Aug; 33(8): 919-927.
16. Schwarz N, Buchinger W, Mähring M et al.: Knee arthroplasty as primary therapy for proximal tibial fracture. Unfallchirurg 2008 Nov; 111(11): 928-932.
17. Messmer P, Regazzoni P, Gross T: New stabilization techniques for fixation of proximnpal tibial fractures (LISS / LCO). Ther Umsch 2003 Dec; 60(12): 762-767.
18. Haidukewych G, Sems SA, Huebner D et al.: Results of polyaxial locked-plate fixation of periarticular fractures of the knee. Surgical technique. J Bone Joint Surg Am 2008; 90 (suppl. 2): 117-134.
19. Haidukewych G, Sems SA, Huebner D et al.: Results of polyaxial locked-plate fixation of periarticular fractures of the knee. J Bone Joint Surg Am 2007; 89: 614-620.
