© Borgis - New Medicine 4/2013, s. 129-131
Jolanta Jadczyszyn, Lechosław P. Chmielik, *Lidia Zawadzka-Głos
Otitis externa induced by a foreign body – a case report
Department of Pediatric Otolaryngology, Medical University of Warsaw, Poland
Head of Department: Lidia Zawadzka-Głos, MD, PhD
Summary
Foreign body is a rare cause of otitis externa. Foreign bodies which clog the auditory canal completely cause a sensation of a blocked ear, pain, hearing loss and tinnitus. Small inorganic bodies can induce no symptoms. Two patients with severe inflammation of the ear canal, which was caused by a foreign body, were hospitalized at The Department of Paediatric Otolaryngology in 2012 years.
INTRODUCTION
Otitis externa may be restricted to one section or comprise the entire ear canal. The major etiological factors are bacteria, fungi and viruses. Skin injuries caused by cleaning the ear, skin maceration secondary to chronic discharge from the ear, diabetes, and immunodeficiency disorders predispose to the infection development. Rare causes of the otitis externa also include foreign bodies inserted into the ear for fun and curiosity. Foreign bodies can be inorganic (hollow beads, buttons, paper balls) or organic (a peas, beans, seeds, fruits, catkins) (1-3). Rarely do we find the foreign bodies in a form of vexing insects, which are alive and move along the ear. Foreign bodies which clog the auditory canal completely cause a sensation of a blocked ear, pain, hearing loss and tinnitus. Small inorganic body can cause no symptoms.
CASE STUDY 1
A 2-year-old girl was admitted because of severe pain in her right ear which had persisted for 5 days. The anamnesis revealed that six days before the admission, the area the right ear pinna had been injured. Therefore, the child remained without an outpatient treatment. She was in a good general condition and had no fever. The laryngology examination revealed a very narrow auditory meatus which prevented an otoscopic evaluation of the tympanic membrane. The examination findings included also a reddening and protruding of the auricle with swelling and redness of the skin covering the soft tissues behind the ear. There was no pathological discharge in the auditory meatus. The results of laboratory tests were as followed: the elevated inflammatory markers, without signs of anaemia, coagulation profile was normal (tab. 1).
Table 1. Laboratory tests.
| WBC | RBC | HGB | HCT | LYMPH | NEUT | OB | CRP | APTT | INR |
| 15.4 thous. | 4.07 mln | 10.5 g/dl | 32.7% | 44.9% | 46% | 58 mm/h | 2.7 mg/dl | 33.6 sec. | 0.94 |
The girl was diagnosed with otitis externa. Swabs from the right ear were obtained and the culture revealed Staphylococcus aureus (MSSA).
The topical treatment with and intravenous administration of antibiotics (a third-generation cephalosporin) was commenced. Due to the lack of significant results of the treatment and resolution of symptoms, temporal bone CT was performed on the second day of hospitalization.
The CT revealed occlusion of the right auditory meatus, presence of the metallic foreign body in the final section („plug of an earring”), swelling of the external auditory meatus walls. Tympanic membrane was dislocated towards the tympanic cavity and its perforation had to be considered. Also some artefacts associated with the foreign body were visible. The tympanic cavity was partially airless. The articulation of the auditory ossicles was normal. The left ear remained unchanged (fig. 1).
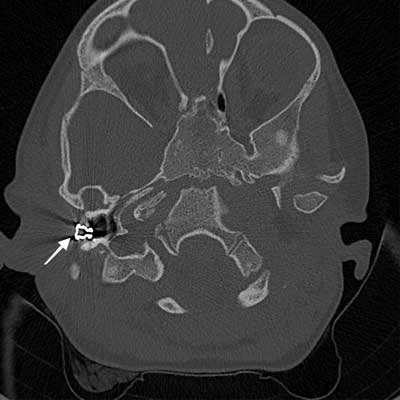
Fig. 1. The temporal bone CT scan – a foreign body is visible in the right external auditory meatus.
The patient was immediately qualified for a surgery.
The metallic foreign body was removed under a general anaesthesia (fig. 2).

Fig. 2. A metallic plug of an earring.
No complications developed in the postoperative period. The otoscopic evaluation showed a preserved tympanic membrane and the perforation was excluded.
CASE STUDY 2
A 4-year-old girl was referred to ENT clinic due to purulent and sanguineous discharge from the right ear which was present four days. She was on an antibiotic (Augmentin) for 3 days, however no improvement was recorded. The anamnesis revealed an inhalation allergy, the state after adenotonsillectomy and ventilation drainage (two years earlier). On admission, the patient was in a good general condition and had no fever. The results of the laboratory tests were normal (tab. 2).
Table 2. Laboratory tests.
| WBC | RBC | HGB | HCT | LYMPH | NEUT | OB | CRP | APTT | INR |
| 8.1 thous. | 4.46 mln | 12.5 g/dl | 37.5% | 51.9% | 38.6% | 11 mm/h | < 0.5 mg/dl | 39.5 sec. | 1.06 |
The laryngological examination revealed a collapsed upper and posterior wall of the external auditory canal and the ear canal filled with sanguineous and purulent discharge. After cleaning the ear, the inflammatory granulation tissue was found in the external auditory canal and it was obscuring the lower part of the posterior tympanic membrane. The other part of the membrane was matt. Treatment with intravenous Amoksiklav was started. On the 4th day of hospitalization discharge in the right ear disappeared. The temporal bone CT scan was performed on the 8th day of hospitalization.
It showed a small soft-tissue lesion – a granulation tissue, 5 x 2.7 mm in size – in the right external auditory canal which was located right by the tympanic membrane. Besides, the mastoid process and temporal cavities were aerated on both sides. Order of the ossicles was preserved. The inner ear structures did not show any abnormalities on any side. The external auditory canal of the left ear was also normal (fig. 3).

Fig. 3. An inflammatory granulation tissue in the right ear.
The granulation tissue and a foreign body were removed from the right auditory canal and a ventilation drain was placed under a general anaesthesia on the 10th day of treatment. Perforation of the right tympanic membrane was diagnosed. The postoperative period was uneventful. The performed tympanic membrane finally was healed and the follow-up examination showed no abnormalities.
DISCUSSION
Two patients with severe inflammation of the ear canal, which was caused by a foreign body, were hospitalized at The Department of Paediatric Otolaryngology in 2012 years. Children usually put foreign bodies into the ear by accident. Parents are often unaware of the presence of a foreign body in the ear, so they may come to a doctor only after the lapse of time. In most cases, foreign bodies can be easily removed. It is sometimes necessary to postpone a surgery, even though it seems urgent, due to the severe inflammation of the external auditory canal or a delayed visit in the hospital (4). In some cases foreign bodies are a difficult clinical problem due to the possibility that the ear has been damaged in the injury or a risk of damaging the ear during the procedure.
A foreign body can induce a severe infection and even lead to intratemporal complications of otitis media (4). Careful imaging examination and observation of the patient are therefore crucial. A computed tomography (CT) is the basic imaging procedure in such cases.
In cases of resistant otitis externa in children, examination with a surgical microscope under general anaesthesia is recommended. It is essential to start antibiotherapy with broad-spectrum antibiotics. The treatment should be started immediately because a progressive swelling and inflammation of the meatus skin can make the foreign body removal more complicated. A foreign body should be removed by an experienced laryngologist equipped with all the required instruments (5-7). It also reduces the risk of complications associated with the very procedure (8). Improper performance of the procedure in a restless child may pose a considerable hazard. It may lead to pushing the foreign body deeper into the meatus, behind the isthmus, the external auditory canal or tympanic membrane injury, dislocation of the ossicles, the facial nerve damage or acute purulent otitis media (5, 9). In about 96% of the cases, it is possible to remove the foreign from the external auditory canal without anaesthesia. In approximately 4% of the cases, it is required to perform the procedure under general anaesthesia in an operating theatre (9). If a foreign body cannot be removed from the meatus, then the procedure should be performed from the side of the mastoid process (5, 10).
CONCLUSIONS
1. The discussed cases illustrate rare causes of otitis media in children.
2. The out-patient setting can make the diagnosis of otitis media difficult.
3. In every case of resistant otitis, a specific inflammation or a foreign body presence should be considered.
4. Patients after the ventilation drainage, require a very careful postoperative follow-up until the moment when the drain falls out.
Piśmiennictwo
1. Janczewski G, Goździk-Żołnierkiewicz T: Konsultacje otolaryngologiczne. PZWL; Warszawa 1990. 2. Ansley JF, Cunningham MJ: Treatment of aural foreign bodies in children. Pediatrics 1998; 101(4 Pt 1): 638-641. 3. Baker MD: Foreign bodies of the ears and nose in childhood. Pediatr Emerg Care 1987; 3(2): 67-70. 4. Burke RT, Gatton B, Melville LD: Mastoiditis and meningitis complicating an aural foreign body. Pediatr Emerg Care 2012; 28(10): 1070-1071. 5. Otolaryngologia dziecięca, red. M. Chmielik, PZWL; Warszawa 2001. 6. Szmeja Z: Ciała obce ucha, nosa, gardła, krtani, dolnych dróg oddechowych i przełyku. Przew. Lek. 2002, 9(45): 94-96. 7. Bressler K, Shelton C: Ear foreign-body removal: a review of 98 consecutive cases. Laryngoscope 1993; 103(4 Pt 1): 367-370. 8. Olajide TG, Ologe FE, Arigbede OO: Management of foreign bodies in the ear: a retrospective review of 123 cases in Nigeria. Ear Nose Throat J 2011; 90(11): 16-19. 9. Ologe FE, Dunmade AD, Afolabi OA: Aural foreign bodies in children. Indian J Pediatr 2007; 74(8): 755-758. 10. Piromchai P, Srirompotong S, Lertchanaruengrith P, Mills R: A child presenting with a bullet in the middle ear: case report. Clin Med Insights Case Rep 2012; 5: 1-4.
