© Borgis - New Medicine 1/2014, s. 26-28
*Konrad Wroński1,2
Prophylactic gastroenterostomy in patient with unresectable pancreatic head cancer – case report
1Faculty of Medicine, Department of Oncology, University of Warmia and Mazury, Olsztyn, Poland
Head of Department of Oncology: prof. Sergiusz Nawrocki, MD, PhD
2Department of Surgical Oncology, Hospital Ministry of Internal Affairs with Warmia and Mazury Oncology Centre, Olsztyn, Poland
Head of Department of Surgical Oncology: Andrzej Lachowski, MD
Summary
Optimal treatment patients with unresectable pancreatic head cancer is still a matter of debate for several reasons. The number of patients with unresectable pancreatic head cancer is increasing and their optimal treatment is a growing economic problem for health care. In this article the author presented a case of a man who was admitted to the hospital because of unresectable pancreatic head cancer. The patient underwent prophylactic gastroenterostomy and in the fifth day after surgery was discharged home.
INTRODUCTION
Optimal treatment patients with unresectable pancreatic head cancer is still a matter of debate for several reasons (1, 2). First reason: it is difficult to predict the number of patients who will suffer from duodenal obstruction, and second reason is possible complications after gastroenterostomy (1-5). The number of patients with unresectable pancreatic head cancer is increasing and their optimal treatment is a growing economic problem for health care (4-7).
CASE REPORT
A 58-year-old man, Caucasian race, was admitted to the Department of Surgical Oncology because of pancreatic head tumor. The patient did not eat the food for last 10 days, drank only water. Within a month, he lost about 10 kg. He had history of alcohol consumption about 80-120 gram/day for 10 years and he was heavy smoker – 15 cigarette/day for 20 years. In the past the patient have had pancreatitis twice and did not claim any additional diseases.
Blood examination of the patient showed raised results of amylase and lipase results and low levels of albumin and total protein. Other laboratory tests were normal.
On physical examination, in the epigastrium area a tumor was palpable. CT examination showed a pathological mesogastric lumpy mass in the region of the descending duodenum and the head of the pancreas, the size of tumor was approximately 50 x 58 x 42 mm, with cystic spaces and small, individual calcifications. The rest of the pancreas was not enlarged, even atrophic, but with a prominent extended to approximately 6 mm pancreatic duct in the stem of the pancreas and less clearly in its tail (fig. 1). A tumor of the pancreatic head infiltrated and compressed the duodenum causing obstruction of the upper gastrointestinal tract (fig. 2).
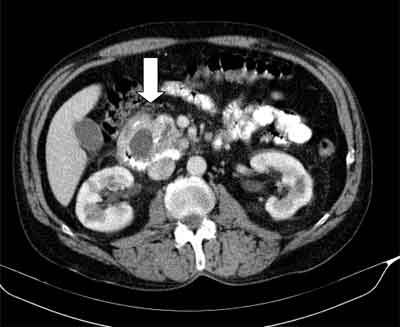
Fig. 1. CT image showed the large pancreatic tumor (diameter 50 x 58 x 42 mm) infiltrating and compression of the duodenum.
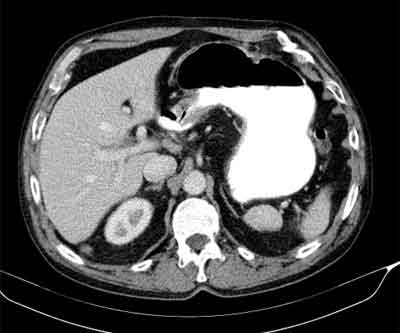
Fig. 2. CT image showed the residual contents of the stomach caused by obstruction of the duodenum. Duodenal obstruction was caused by infiltration and compression of the duodenum by the pancreatic tumor.
The patient was qualified for surgery. After opening the abdomen and reaching the pancreas, surgeons found a large tumor of the pancreatic head diameter about 60 mm infiltrating on celiac trunk and superior mesenteric artery. The case was considered as an inoperable. Tumor stage was assessed on: cT4NXM0. From pancreatic tumor samples were collected for intra histopathological examination. Histopathological examination revealed the presence of cancer cells The patient had performed prophylactic gastroenterostomy (fig. 3, 4). The duration of surgery was 60 minutes. Patient after surgery felt good and did not complain of pain. The postoperative period was uncomplicated and the patient left the ward in the fifth day after operation. The patient is in the care of outpatient surgical oncology and was pre-qualified for palliative chemotherapy.

Fig. 3. Photo taken while performing prophylactic gastroenterostomy.

Fig. 4. Prophylactic gastroenterostomy.
DISCUSSION
Pancreatic neoplasms account for 3% of all cancers in Poland (8). The risk of pancreatic carcinoma is greater in men, the elderly, obese and lack of physical activity (2, 4, 5, 8). Tumors around the so-called field of pancreatic-duodenal originate mainly from the head of the pancreas. Early pancreatic cancer is usually detected incidentally during a CT done accidentally (5, 6, 8). Most patients seeking treatment of large unresectable tumors of the pancreas (4).
A large number of patients with unresectable pancreatic head cancer is a growing challenge for health care. Recent articles suggest that effective treatment of such patients should consist of the performance of prophylactic gastroenterostomy in order to improve the quality of life in the final days (3, 4).
One of the unfavorable symptoms after gastroenterostomy is the occurrence delay gastric emptying (DGE). It is estimated that the DGE occurs in 9% to 26% of patients after such treatment (9). Delay gastric emptying is defined by the International Study Group of Pancreatic Cancer as a problem, which has been linked to tumor involvement of the coeliac axis and interruption of splachnic innervations (1, 5, 6, 9). According to the author of this article correct technique of gastroenterostomy helps to reduce to a minimum of DGE.
Some authors recommend performing laparoscopic gastroenterostomy or Roux gastrojejunostomy in unresectable tumors of the pancreas (5, 10). Supporters of this technique believe that the efficacy and safety for the patient of this method are high and period to recovery faster than after open surgery (10).
CONCLUSIONS
The author of this article, having an experience in the treatment of patients with unresectable cancer of the pancreatic head believes, that prophylactic gastroenterostomy should be „the gold standard” in the treatment of such patients. Gastroenterostomy is easy, cheap and safely procedure, and reduces costs of health care. The author of this article believes that patients with unresectable pancreatic head cancer should be treatment in highly specialized oncological surgery wards.
Piśmiennictwo
1. Sarr MG, Cameron JL: Surgical management of unresectable carcinoma of the pancreas. Surgery 1982; 91: 123-133. 2. Jacobs PP, van der Sluis RF, Wobbes T: Role of gastroenterostomy in the palliative surgical treatment of pancreatic cancer. J Surg Oncol 1989; 42: 145-149. 3. Hwang SI, Kim HO, Son BH et al.: Surgical palliation of unresectable pancreatic head cancer in elderly patients. World J Gastroenterol 2009; 15: 978-982. 4. Huser N, Michalski CW, Schuster T et al.: Systematic review and meta-analysis of prophylactic gastroenterostomy for unresectable advanced pancreatic cancer. Br J Surg 2009; 96: 711-719. 5. Shyr YM, Su CH, Wu CW, Lui WY: Prospective study of gastric outlet obstruction in unresectable periampullary adenocarcinoma. World J Surg 2000; 24: 60-64. 6. Lillemoe KD, Cameron JL, Hardacre JM et al.: Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer? A prospective randomized trial. Ann Surg 1999; 230: 322-338. 7. van der Schelling GP, van den Bosch RP, Klinkenbij JH et al.: Is there a place for gastroenterostomy in patients with advanced cancer of the head of the pancreas? World J Surg 1993; 17: 128-132. 8. Krzakowski M, Warzocha K: Zalecenia postępowania diagnostyczno-terapeutycznego w nowotworach złośliwych 2013 rok. Gdańsk 2013. 9. Horstmann O, Kley CW, Post S, Becker H: Cross-section gastroenterostomy in patients with irresectable periampullary carcinoma. HPB (Oxford) 2001; 3: 157-163. 10. Muniraj T, Barve P: Laparoscopic staging and surgical treatment of pancreatic cancer. N AM J Med Sci 2013; 5: 1-9.
