© Borgis - Postępy Nauk Medycznych 11/2016, s. 846-851
*Michał A. Skrzypczyk1, Damian Sujecki1, Łukasz Nyk2, Maciej Zbrzeźniak1, Stanisław Szempliński1, Jakub Dobruch1, 2
Artificial urinary sphincter – new devices in male urinary incontinence treatment
Nowe konstrukcje zwieraczy hydraulicznych wykorzystywane w leczeniu nietrzymania moczu u mężczyzn
12nd Unit of Didactics, Department of Urology, Centre of Postgraduate Medical Education, Professor W. Orłowski Independent Public Teaching Hospital, Warsaw
Head of Department: Jakub Dobruch, MD, PhD
21st Unit of Didactics, Department of Urology, Centre of Postgraduate Medical Education, European Health Centre Otwock
Head of Department: Jakub Dobruch, MD, PhD
Streszczenie
Częstość występowania nietrzymania moczu (ang. urinary incontinence – UI) wśród mężczyzn wynosi od 4,81 do 32,17% i wzrasta wraz z wiekiem. UI może być następstwem leczenia chirurgicznego mężczyzn dotkniętych łagodnym rozrostem gruczołu krokowego (ang. benign prostate hyperplasia – BPH) i/lub rakiem gruczołu krokowego (ang. prostate cancer – PCa). Najczęściej stosowanym i do niedawna jedynym sposobem leczenia nietrzymania moczu u mężczyzn była implantacja sztucznego zwieracza cewki moczowej (ang. artificial urinary sphincter – AUS) typu AMS 800 (American Medical System). Ze względu na różnice w stopniu nasilenia nietrzymania moczu, niemałą liczbę powikłań oraz koszty związane ze wszczepieniem AUS, w ostatnich latach powstało szereg nowych urządzeń dedykowanych chorym dotkniętym UI. Konstrukcje te posiadają nowe rozwiązania technologiczne, które powinny zapewnić co najmniej podobne wyniki czynnościowe i doprowadzić do zmniejszenia liczby powikłań towarzyszących wszczepieniu AUS. W opracowaniu przedstawiono przegląd nowych urządzeń stosowanych w leczeniu mężczyzn chorych na wysiłkowe nietrzymanie moczu.
Summary
The incidence of male stress urinary incontinence (UI) ranges from 4.81 to 32.17% and usually increases with age. UI can be a consequence of surgical treatment of benign prostate hyperplasia (BPH) and/or prostate cancer (PCa). The American Medical System type 800 (AMS800) has been the most common and, until recently, the only artificial urinary sphincter (AUS) available for UI surgical treatment. Due to differences in UI grades and a considerable number of complications as well as costs associated with AUS implantation, several new devices for UI treatment have been introduced in the recent years. These devices offer novel technological solutions, which in theory should provide at least similar functional outcomes and lower complications associated with the classical AMS sphincter. The study provides a review of new devices for male stress UI treatment.

Introduction
Male urinary incontinence (UI) is a rare condition. Depending on the characteristics of patients, the incidence of male stress urinary incontinence ranges from 4.81 to 32.17% (1) and usually increases with age (2, 3).
UI can be a consequence of surgical treatment of benign prostate hyperplasia (BPH). In patients treated with transurethral resection of the prostate (TURP), transurethral incision of the prostate (TUIP) or open enucleation of adenoma (OEA), a low-grade urinary incontinence or total urinary incontinence develop in 2.2 and 1%, 1.8 and 0.1% as well as 1.9 and 0.5% of cases, respectively (4).
Patients treated with radical prostatectomy (RP) due to prostate cancer (PCa) develop UI more frequently. The incidence of UI after RP, irrespective of the technique adopted (open, laparoscopic or robotic), is similar and ranges from 1 to 40%, but discrepancies between subsequent series result from differences in defining UI and the length of the follow-up (5-7).
If a PCa patient undergoes external beam radiotherapy (EBRT) or brachytherapy (BT), UI occurs in 0-18.8% and 0-13% of patients, respectively (8-11).
Irrespective of the UI cause, 6-9% of cases are managed surgically (12-15).
Artificial urinary sphincter (AUS) implantation is the basic treatment method. Until recently, the only device used in such cases was American Medical System type 800 (AMS800). It was introduced to common practice in 1983 and has been used ever since in a nearly identical form (16). AMS800 guarantees full continence and/or quality of life improvement in 79% (61-100%) of patients. In long-term follow-up, effects are permanent. The re-intervention rate resulting from AUS infection or urethral erosion ranges from 3.3 to 27.8% (17).
Due to differences in UI grades and a considerable number of complications as well as costs associated with AUS implantation, several new devices for UI treatment have been introduced in the recent years.
Suburethral slings
High efficacy of suburethral slings in female UI made this technique also used in male patients. They create a subcystic barrier that improves continence and guarantees efficient micturition. These implants can be divided into two basic types: non-adjustable and adjustable tapes with adjustable pressure on the urethra.
Suburethral non-adjustable slings
The first tape of this type, which currently is no longer used, is the InVance tape.
A transobturator suburethral non-adjustable AdVance (American Medical Systems) (fig. 1) sling is a monofilament and polypropylene mesh. It is implanted transperineally. The main part of the mesh (the suburethral one) is fitted on the ventral surface of the proximal bulbous urethra, and the tape arms are passed through the obturator foramina. The AdVance system ensures full continence or guarantees considerable improvement in 62-77% of patients in a 3-year follow-up. The implantation technique is relatively simple, which makes the complication rate rather low (18, 19).

Fig. 1. Suburethral AdVance sling (American Medical Systems)
I-STOP TOMS (CL Medical) (fig. 2) is another tennon-adjustable suburethral sling. It differs from the previous model in construction and location under the urethra, but the principle underlying its action seems to be similar. Grise et al., in the first study on safety and efficacy of the I-STOP TOMS system, report that 60/69 patients (87%) experienced continence improvement after a year of follow-up. In the investigated group, 41 (59.4%), 14 (20.3%) and 5 (7.3%) patients did not use any pads, used 1 pad or more than 1 pad, respectively. No severe complications were noted. The cavernous bodies were damaged during implantation in 4% of patients. Generally, 91% of patients were satisfied or very satisfied after the procedure (20).

Fig. 2. I-STOP TOMS system (CL Medical)
Suburethral tension adjustable slings (devices)
In the case of first-generation slings, patients observed gradual deterioration in continence with time. Another problem was hypercontinence in the initial period post-surgery, which occurred in 12-21% of patients (19, 21).
Factors that might be responsible for these phenomena include the lack of a standardized way of adjusting tension during the procedure and post-surgery. The introduction of new-generation devices, characterized by a possibility to regulate pressure on the urethra, was supposed to solve the problem.
Argus system (Promedon)
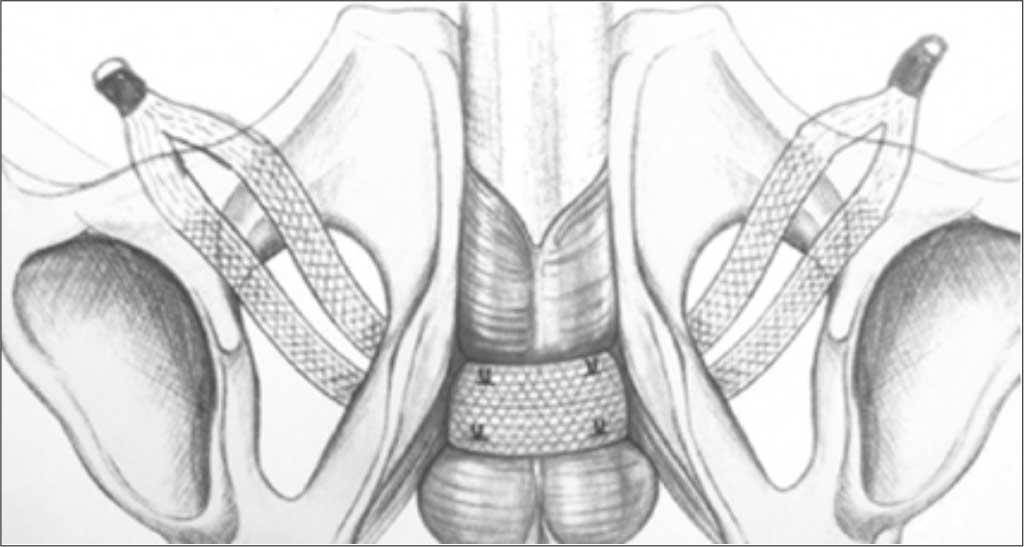
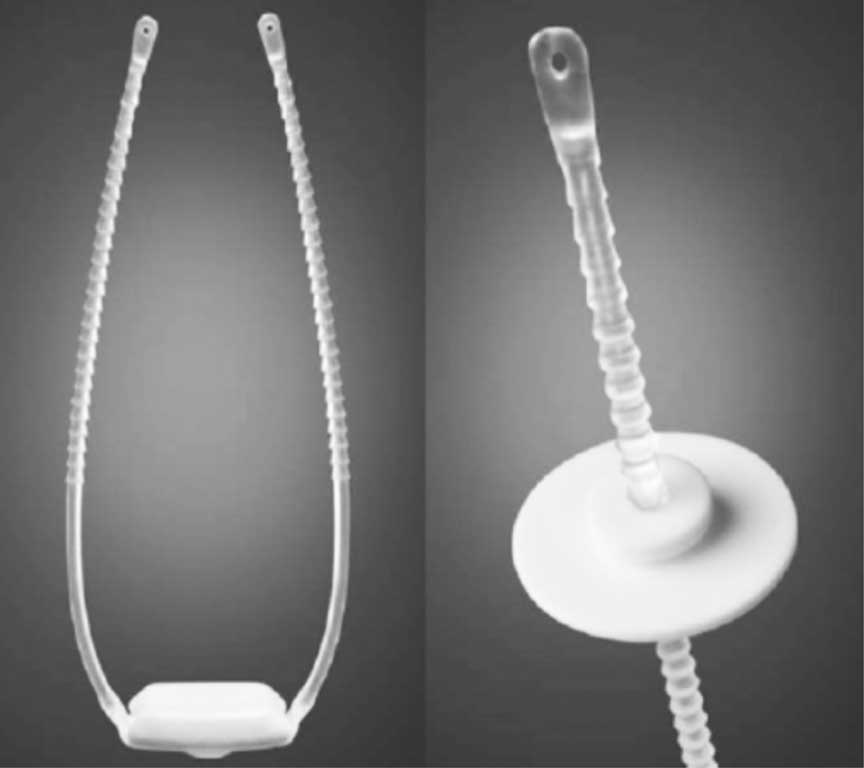
One of the first devices of this type was Argus (fig. 3) in which a silicone pad placed suburethrally could be pulled up postoperatively thanks to arms inserted using the retropubic approach. The blocking mechanism was fixed in the rectus fascia. The Argus sling was implanted in 101 patients. After a median follow-up of 2.2 years, the rate of fully dry patients was 79.2% (80/101). Tape adjustment was necessary in 39 cases (38.6%) approximately 104.3 days after the initial implantation. Twenty-nine patients required sling tightening, which was conducted under regional anaesthesia, whereas 10 patients had it loosened under general anaesthesia. The sling had to be removed in 16 patients (15.8%) due to urethral erosion or infection.

Fig. 3. Argus system (Promedon)
Phorbas system (Promedon)
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Shamliyan TA, Wyman JF, Ping R et al.: Male urinary incontinence: prevalence, risk factors, and preventive interventions. Rev Urol 2009; 11(3): 145-165.
2. Thom D: Variation in estimates of urinary incontinence prevalence in the community: effects of differences in definition, population characteristics, and study type. J Am Geriatr Soc 1998 Apr; 46(4): 473-480.
3. Koyama W, Koyanagi A, Mihara S et al.: Prevalence and conditions of urinary incontinence among the elderly. Methods Inf Med 1998 Jun; 37(2): 151-155.
4. McConnell JD, Barry MJ, Bruskewitz RC: Benign prostatic hyperplasia: diagnosis and treatment. Agency for Health Care Policy and Research. Clin Pract Guidel Quick Ref Guide Clin 1994 Feb; 8: 1-17.
5. Rodriguez E, Skarecky DW, Ahlering TE: Post-robotic prostatectomy urinary continence: characterization of perfect continence versus occasional dribbling in pad-free men. Urology 2006; 67: 785-788.
6. Krupski TL, Saigal CS, Litwin MS: Variation in continence and potency by definition. J Urol 2003; 170: 1291-1294.
7. Olsson LE, Salomon L, Nadu A et al.: Prospective patient-reported continence after laparoscopic radical prostatectomy. Urology 2001; 58: 570-572.
8. Lawton CA, Won M, Pilepich MV et al.: Long-term treatment sequelae following external beam irradiation for adenocarcinoma of the prostate: analysis of RTOG studies 7506 and 7706. Int J Radiat Oncol Biol Phys 1991 Sep; 21(4): 935-939.
9. Wallner K, Roy J, Zelefsky M et al.: Fluoroscopic visualization of the prostatic urethra to guide transperineal prostate implantation. Int J Radiat Oncol Biol Phys 1994 Jul 1; 29(4): 863-867.
10. Blasko JC, Ragde H, Luse RW et al.: Should brachytherapy be considered a therapeutic option in localized prostate cancer? Urol Clin North Am 1996 Nov; 23(4): 633-650.
11. Talcott JA, Clark JA, Stark PC, Mitchell SP: Long-term treatment related complications of brachytherapy for early prostate cancer: a survey of patients previously treated. J Urol 2001 Aug; 166(2): 494-499.
12. Penson DF, McLerran D, Feng Z et al.: 5-year urinary and sexual outcomes after radical prostatectomy: Results from the prostate cancer outcomes study. J Urol 2005; 173: 1701-1705.
13. Begg CB, Riedel ER, Bach PB et al.: Variations in morbidity after radical prostatectomy. N Engl J Med 2002; 346: 1138-1144.
14. Steineck G, Helgesen F, Adolfsson J et al.: Quality of life after radical prostatectomy or watchful waiting. N Engl J Med 2002; 347: 790-796.
15. Stanford JL, Feng Z, Hamilton AS et al.: Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: the Prostate Cancer Outcomes Study. JAMA 2000; 283: 354-360.
16. Szopiński T, Chłosta PL, Borówka A: Wyniki leczenia nietrzymania moczu z użyciem sztucznego zwieracza cewki moczowej. Post N Med 2012; 4: 325-334.
17. Van der Aa F, Drake MJ, Kasyan GR et al.: Young Academic Urologists Functional Urology Group. The artificial urinary sphincter after a quarter of a century: a critical systematic review of its use in male non-neurogenic incontinence. Eur Urol 2013 Apr; 63(4): 681-689.
18. Rehder P, Haab F, Comu JN et al.: Treatment of postprostatectomy male urinary incontinence with the transobturator retroluminal repositioning sling suspension: 3-year follow-up. Eur Urol 2012; 62(1): 140-145.
19. Zuckerman JM, Edwards B, Henderson K et al.: Extended outcomes in the treatment of male stress urinary incontinence with a transobturator sling. Urology 2014; 83(4): 939-945.
20. Grise P, Vautherin R, Njinou-Ngninkeu B et al.: HOMme INContinence Study Group. I-STOP TOMS transobturator male sling, a minimally invasive treatment for post-prostatectomy incontinence: Continence improvement and tolerability. Urology 2012; 79: 458-463.
21. Bauer RM, Mayer ME, May F et al.: Complications of the AdVance transobturator male sling in the treatment of male stress urinary incontinence. Urology 2010; 75(6): 1494-1498.
22. Huebner W, Herschorn S, Olmedo T et al.: The phorbas system – a new single incision adjustable male sling. International Continence Society Meeting 2014 Poster no 681.
23. Bauer W, Karik M, Schramek P: The self-anchoring transobturator male sling to treat stress urinary incontinence in men: a new sling, a surgical approach and anatomical findings in a cadaveric study. BJU Int 2005; 95: 1364-1366.
24. Hoda MR, Primus G, Fischereder K et al.: Early results of a European multicentre experience with a new self-anchoring adjustable transobturator system for treatment of stress urinary incontinence in men. BJU Int 2013; 111(2): 296-303.
25. Rouprêt M, Misraï V, Gosseine PN et al.: Management of stress urinary incontinence following prostate surgery with minimally invasive adjustable continence balloon implants: Functional results from a single center prospective study. J Urol 2011; 186: 198-203.
26. Schiavini JL, Damiao R, de Resende Junior JAD et al.: Treatment of post-prostate surgery urinary incontinence with the periurethral constrictor: a retrospective analysis. Urology 2010; 75: 1488-1492.
27. Simone G, Guaglianone S, Papalia R et al.: Periurethral constrictor (Silimed): a new device for treatment of mild urinary incontinence Following radical prostatectomy. J Urol 2009; 181 (suppl. 4): 619.
28. Introini C, Naselli A, Zaninetta G et al.: Safety and efficacy of periurethral constrictor implantation for the treatment of post-radical prostatectomy incontinence. Urology 2012 May; 79(5): 1175-1178.
29. Lima RS, Barros EGC, Souza CA et al.: Periurethral constrictor: late results of the treatment of post prostatectomy urinary incontinence. International Braz J Urol 2011; 37(4): 483-487.
30. Staerman F, G-Llorens C, Leon P et al.: ZSI 375 artificial urinary sphincter for male urinary incontinence: A preliminary study. BJU Int 2013; 111: E202-206.
31. Sandul A, Martins FE, Barros P et al.: The ZSI 375 artificial urinary sphincter: a new device for male urinary incontinence. 7th National Congress of Portuguese Association of Neurourology and Urogynecology, Vilamoura, Portugal, November 2010.
32. Malaeb BS, Elliott SP, Lee J et al.: Novel artificial urinary sphincter in the canine model: the tape mechanical occlusive device. Urology 2011; 77(1): 211-216.