Jacek Smereka1, *Lukasz Szarpak2, Elzbieta Makomaska-Szaroszyk2, Antonio Rodriguez-Nunez3, Sandra Pyda4, Izabela Sztybor2, Klaudia Wlodarska2, Klaudia Kulak2, Karol Bielski2, Kurt Ruetzler5
Comparison of two chest compression techniques during infant resuscitation. A randomized, cross-over study
Porównanie dwóch technik uciskania klatki piersiowej podczas resuscytacji niemowlęcia. Badanie randomizowane krzyżowe
1Department of Emergency Medical Service, Wroclaw Medical University, Poland
2Lazarski University, Warsaw, Poland
3Paediatric Emergency and Critical Care Division, Clinical University Hospital, University of Santiago de Compostela, Santiago de Compostela, Institute of Research of Santiago (IDIS) and SAMID Network, Spain
4Polish Society of Disaster Medicine, Warsaw, Poland
5Department of Outcomes Research, Anesthesiology Institute, Cleveland Clinic, Cleveland, USA; Department of General Anesthesiology, Anesthesiology Institute, Cleveland Clinic, Cleveland, USA
Streszczenie
Wstęp. Wysokiej jakości uciski klatki piersiowej stanowią nieodłączny element resuscytacji krążeniowo-oddechowej wpływający bezpośrednio na jej skuteczność, a tym samym powrót spontanicznego krążenia. Wytyczne Amerykańskiego Towarzystwa Kardiologicznego zalecają prowadzenie resuscytacji noworodków i niemowląt jedną z dwóch technik: techniką dwóch palców (TFT) bądź techniką dwóch kciuków (TTHT), w której dwa kciuki oparte są o mostek, zaś pozostałe palce obejmują klatkę piersiową, stanowiąc podporę dla pleców dziecka. Jednakże jak wskazują liczne badania, każda z tych technik ma zarówno plusy, jak i minusy.
Cel pracy. Celem pracy była ocena jakości wybranych technik uciskania klatki piersiowej podczas symulowanej resuscytacji krążeniowo-oddechowej niemowlęcia prowadzonej przez studentów ostatniego roku medycyny.
Materiał i metody. Badanie zostało zaprojektowane jako randomizowane krzyżowe. W badaniu udział wzięło 41 studentów ostatniego roku medycyny. Uczestnicy badania wykonywali 2-min cykl resuscytacji krążeniowo-oddechowej niemowlęcia w oparciu o schemat 15 uciśnięć klatki piersiowej: 2 oddechy ratownicze. Uciśnięcia klatki piersiowej były prowadzone dwiema technikami: TTHT oraz nowatorską techniką dwóch kciuków (NTTHT). Analizie poddano jedynie parametry dotyczące jakości uciśnięć klatki piersiowej.
Wyniki. Prowadzenie uciśnięć klatki piersiowej w oparciu o NTTHT w porównaniu z TTHT wiązało się z wyższym odsetkiem uciśnięć klatki piersiowej wykonanych na odpowiednią głębokość (94% (IQR: 87-96) vs. 92% (IQR: 88-95); p = 0,003), lepszą relaksacją klatki piersiowej (94% (IQR: 92-99) vs. 13% (IQR: 9-18); p < 0,001), bardziej poprawnym ułożeniem rąk na klatce piersiowej (98% (IQR: 98-100) vs. 95% (IQR: 89-97); p = 0,045) oraz niższym czasem bez uciśnięć klatki piersiowej (4,5 s (IQR: 3-5) vs. 5,5 s (IQR: 4-6); p = 0,038). Głębokość uciśnięć klatki piersiowej z wykorzystaniem TTHT wynosiła 42 mm (IQR: 39-44), zaś w przypadku NTTHT – 41 mm (IQR: 39-42).
Wnioski. W przeprowadzonym badaniu symulacyjnym stosowanie nowatorskiej metody uciskania klatki piersiowej wiązało się z wyższej jakości uciśnięciami klatki piersiowej niemowlęcia w porównaniu z rekomendowaną przez wytyczne Amerykańskiego Towarzystwa Kardiologicznego czy też Europejskiej Rady Resuscytacji.
Summary
Introduction. High quality chest compressions are an inherent element of cardiopulmonary resuscitation that directly influences its effectiveness and thus the return of spontaneous circulation. The guidelines of the American Society of Cardiology recommend conducting resuscitation of newborns and infants with one of two techniques: two-finger technique (TFT) or two thumbs technique (TTHT) in which two thumbs are placed on the sternum and the other fingers cover the chest supporting the child’s back. However, as numerous studies indicate, each of these techniques has its own advantages and disadvantages.
Aim. The aim of the study was to assess the quality of selected chest compression techniques during simulated cardiopulmonary resuscitation of an infant conducted by final-year medical students.
Material and methods. The consent of the Institutional Review Board of the International Institute of Rescue Research and Education, as well as written consent from all the parents were obtained. The study was designed as a randomized, cross-over study. The study was attended by 41 students in their final year of medicine. Participants of the study performed a two-minute cycle of cardiopulmonary resuscitation on an infant based on a schedule of 15 chest compressions: 2 rescue breaths. Chest compressions were carried out by two techniques: TTHT and the innovative technique of two thumbs (NTTHT). Only the parameters concerning the quality of chest compressions were analyzed in the study.
Results. Chest compressions based on NTTHT compared with TTHT were associated with a higher percentage of chest compressions performed at the appropriate depth (94% (IQR: 87-96) vs. 92% (IQR: 88-95); p = 0.003), better chest relaxation (94% (IQR: 92-99) vs. 13% (IQR: 9-18); p < 0.001), more correct positioning of the hands on the chest (98% (IQR: 98-100) vs. 95% (IQR: 89-97); p = 0.045) and less time without chest compressions (4.5 s (IQR: 3-5) vs. 5.5 s (IQR: 4-6); p = 0.038). Depth of chest compressions using TTHT was 42 mm (IQR: 39-44) and 41 mm (IQR: 39-42) for NTTHT.
Conclusions. In the conducted simulation study, students in their final year of medicine using an innovative method of chest compressions were associated with higher-quality compressions of the infant’s chest compared to the recommendations by the American Society of Cardiology or the European Resuscitation Council.

INTRODUCTION
Sudden cardiac arrest in pediatric patients, including infants and newborns, occurs relatively less frequently than in adults (1, 2). Also, the main cause of cardiac arrest in children is different than in adults (3). In the case of adults, the main cause of cardiac arrest is cardiovascular dysfunction, while in the case of pediatric patients, airway obstruction and progressive hypoxia result in cardiac arrest (4).
Guidelines for cardiopulmonary resuscitation recommended by the European Resuscitation Council (ERC) as well as the American Heart Association (AHA) recommend two techniques for chest compressions for infants and newborns (5-8). In the case where resuscitation is carried out by one rescuer, the recommended chest compression method is the two-finger technique (TFT), during which chest compressions are performed using two fingers of one hand at right angles to the chest. In the case when resuscitation is carried out by two rescuers, the recommended technique is based on two thumbs (TTHT), during which the thumbs are located on the patient’s bridge, and the other fingers, including the chest scaffold, constitute a kind of support for the patient’s back. Both techniques have their pros and cons. In the TFT technique, studies indicate much better chest relaxation than in the case of TTHT, however TFT is characterized by chest compressions at a more shallow depth.
Considering the above assumption, it is important to look for new techniques of chest compressions, which will be associated with a higher compression technique. One such technique is a technique developed by the team of Smereka et al. (9, 10) during which chest compressions are performed using two thumbs set perpendicular to the chest, so that they constitute a kind of extension of the forearms.
AIM
The aim of the study was to evaluate the chest compression technique prescribed by the guidelines using the two-thumb method and the author’s two-thumb method during simulated cardiopulmonary resuscitation of an infant conducted by final year medical students.
MATERIAL AND METHODS
The consent of the Institutional Review Board of the International Institute of Rescue Research and Education, as well as written consent from all the parents were obtained. The study is a continuation of the authors’ research cycle on the evaluation of the author’s method of chest compressions in newborns and infants (9-14). Students in their final year of medicine who qualified for the study successfully completed the training module in the field of emergency medicine. The inclusion criterion in the study was the 6th year of medical studies student status and the voluntary willingness to participate in the study. Exclusion criterion from the study was failure to meet the inclusion criteria, back pain or pain in the upper limb that prevents chest compressions. Prior to the study, all participants expressed their willingness to participate in the study.
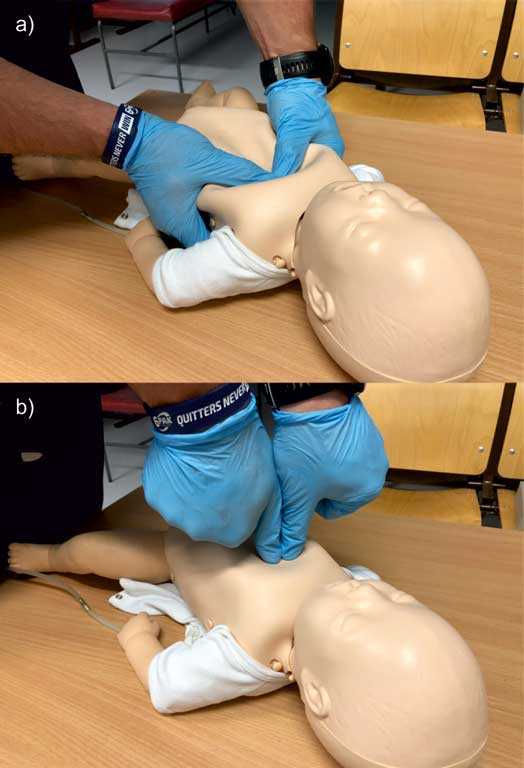
Prior to the study, all participants took part in training in the field of cardiopulmonary resuscitation including demonstrations in the field of standard chest compressions in infants – TTHT, as well as demonstrations in the field of chest compressions developed by Smereka et al. (9, 10), during which the thumbs are directed perpendicular to the chest, constituting a specific prolongation of the forearms (fig. 1a, b). Then they had the opportunity to practice the tested techniques using an infant simulator. To this end, SimBaby™ was used (Laerdal, Stavanger, Norway).

Fig. 1a, b. Chest compression techniques used in the study: a) standard two thumb technique (TTHT); b) novel two thumb technique (NTTHT)
The final study was performed the next day after the demonstrations. During the test, the baby simulator was placed on the floor in a well-lit room. Participants of the study were tasked with performing a two-minute cycle of CPR based on the standard of 15 chest compressions and 2 rescue breaths based on three tested techniques of chest compressions. Both the order of study participants and methods of chest compressions were randomized. For this purpose, the Research Randomizer program was used, with which participants were divided into three groups. The first group began resuscitation based on the TTHT technique and the second group used the NTTHT method. After, the participants had a 10-minute break and then chest compressions were performed using a different technique. A detailed randomization procedure is shown on figure 2.
Fig. 2. Consolidated standards of reporting trials flow chart diagram
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Bielski K, Szarpak L, Smereka J et al.: Comparison of four different intraosseous access devices during simulated pediatric resuscitation. A randomized crossover manikin trial. Eur J Pediatr 2017; 176(7): 865-871.
2. Semsarian C, Ingles J, Wilde AA: Sudden cardiac death in the young: the molecular autopsy and a practical approach to surviving relatives. Eur Heart J 2015; 36(21): 1290-1296.
3. Jo CH, Cho GC, Lee CH: Two-Thumb Encircling Technique Over the Head of Patients in the Setting of Lone Rescuer Infant CPR Occurred During Ambulance Transfer: A Crossover Simulation Study. Pediatr Emerg Care 2017; 33(7): 462-466.
4. Park JW, Jung JY, Kim J et al.: A Novel Infant Chest Compression Assist Device Using a Palm Rather Than Fingers: A Randomized Crossover Trial. Prehosp Emerg Care 2018; 17: 1-9.
5. Wyllie J, Bruinenberg J, Roehr CC et al.: European Resuscitation Council Guidelines for Resuscitation 2015: Section 7. Resuscitation and support of transition of babies at birth. Resuscitation 2015; 95: 249-263.
6. Maconochie IK, Bingham R, Eich C et al.; Paediatric life support section Collaborators: European Resuscitation Council Guidelines for Resuscitation 2015: Section 6. Paediatric life support. Resuscitation 2015; 95: 223-248.
7. Wyckoff MH, Aziz K, Escobedo MB et al.: Part 13: Neonatal Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132(18 suppl. 2): S543-560.
8. Atkins DL, Berger S, Duff JP et al.: Part 11: Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132(18 suppl. 2): S519-525.
9. Ladny JR, Smereka J, Rodríguez-Núñez A et al.: Is there any alternative to standard chest compression techniques in infants? A randomized manikin trial of the new “2-thumb-fist” option. Medicine (Baltimore) 2018; 97(5): e9386.
10. Smereka J, Kaminska H, Wieczorek W et al.: Which position should we take during newborn resuscitation? A prospective, randomised, multicentre simulation trial. Kardiol Pol 2018; 76(6): 980-986.
11. Ruetzler K, Smereka J, Szarpak L et al.: Novel method of infant chest compression. Does the arrangement of the thumbs matter? Am J Emerg Med 2018 Aug 8. pii: S0735-6757(18)30665-X.
12. Smereka J, Szarpak L, Ladny JR et al.: A Novel Method of Newborn Chest Compression: A Randomized Crossover Simulation Study. Front Pediatr 2018; 6: 159.
13. Smereka J, Szarpak L, Rodríguez-Núñez A et al.: A randomized comparison of three chest compression techniques and associated hemodynamic effect during infant CPR: A randomized manikin study. Am J Emerg Med 2017; 35(10): 1420-1425.
14. Smereka J, Bielski K, Ladny JR et al.: Evaluation of a newly developed infant chest compression technique: A randomized crossover manikin trial. Medicine (Baltimore) 2017; 96(14): e5915.
15. Bhanji F, Donoghue AJ, Wolff MS et al.: Part 14: Education: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132(18 suppl. 2): S561-573.
16. Pellegrino JL, Bogumil D, Epstein JL et al.: Two-thumb-encircling advantageous for lay responder infant CPR: a randomised manikin study. Arch Dis Child 2018 Jul 14. pii: archdischild-2018-314893.
17. Christman C, Hemway RJ, Wyckoff MH et al.: The two-thumb is superior to the two-finger method for administering chest compressions in a manikin model of neonatal resuscitation. Arch Dis Child Fetal Neonatal Ed 2011; 96(2): F99-F101.
18. Lee SY, Hong JY, Oh JH et al.: The superiority of the two-thumb over the two-finger technique for single-rescuer infant cardiopulmonary resuscitation. Eur J Emerg Med 2018; 25(5): 372-376.
19. Smereka J, Madziala M, Szarpak L: Comparison of two infant chest compression techniques during simulated newborn cardiopulmonary resuscitation performed by a single rescuer: A randomized, crossover multicenter trial. Cardiol J 2018 Aug 29. DOI: 10.5603/CJ.a2018.0090.
20. Jiang J, Zou Y, Shi W et al.: Two-thumb-encircling hands technique is more advisable than 2-finger technique when lone rescuer performs cardiopulmonary resuscitation on infant manikin. Am J Emerg Med 2015; 33(4): 531-534.
21. Lee SH, Ryu JH, Min MK et al.: Optimal chest compression rate in cardiopulmonary resuscitation: a prospective, randomized crossover study using a manikin model. Eur J Emerg Med 2016; 23(4): 253-257.
22. Yannopoulos D, McKnite S, Aufderheide TP et al.: Effects of incomplete chest wall decompression during cardiopulmonary resuscitation on coronary and cerebral perfusion pressures in a porcine model of cardiac arrest. Resuscitation 2005; 64(3): 363-372.
23. Zou Y, Shi W, Zhu Y et al.: Rate at 120/min provides qualified chest compression during cardiopulmonary resuscitation. Am J Emerg Med 2015; 33(4): 535-538.
24. Aleksandrowicz S, Madziala M, Iskrzycki L et al.: Performance of chest compressions with the use of the new mechanical chest compression machine lifeline arm: a randomized crossover manikin study in novice physicians. Disaster Emerg Med J 2016; 1(1): 30-36.
25. Gawlowski P, Smereka J, Madziala M et al.: Comparison of the ETView Single Lumen and Macintosh laryngoscopes for endotracheal intubation in an airway manikin with immobilized cervical spine by novice paramedics: A randomized crossover manikin trial. Medicine (Baltimore) 2017; 96(16): e5873.
26. Majer J, Jaguszewski MJ, Frass M et al.: Does the use of cardiopulmonary resuscitation feedback devices improve the quality of chest compressions performed by doctors? A prospective, randomized, cross-over simulation study. Cardiol J 2018 Aug 29. DOI: 10.5603/CJ.a2018.0091.