*Maciej Dudek1, Lukasz Szarpak1, Kacper Kranc1, Michal Pruc1, Marek Dabrowski2, Beata Zwolinska1
Focused Assessment with Sonography in Trauma as a diagnostic procedure in prehospital medicine
Badanie ultrasonograficzne FAST jako procedura diagnostyczna w medycynie przedszpitalnej
1Lazarski University, Warsaw, Poland
2Chair and Department of Medical Education, Poznan University of Medical Sciences, Poznan, Poland
Streszczenie
Ultrasonografia jest narzędziem diagnostycznym wykorzystywanym zarówno w medycynie ratunkowej, intensywnej terapii, jak i chirurgii. Postęp technologiczny oraz minimalizacja urządzeń przenośnych spowodowały możliwość wykonywania ultrasonografii poza szpitalem, w tym także w warunkach zespołów wyjazdowych ratownictwa medycznego.
Umiejętność rozpoznawania krwawienia wewnętrznego u pacjentów z obrażeniami ciała stanowi jeden z kluczowych elementów diagnostycznych. Wykonanie ultrasonografii w oparciu o protokoły FAST, BLUE czy też FEEL w warunkach zespołów ratownictwa medycznego może znacząco skrócić czas diagnostyki, kierując pacjenta bezpośrednio na salę zabiegową. Dzięki postępowi techniki medycznej możliwe jest wykonywanie ultrasonografii z wykorzystaniem mobilnych urządzeń. W coraz większej liczbie zespołów ratownictwa medycznego dostępne są przenośne urządzenia do ultrasonografii. W celu efektywnego wykorzystania tych urządzeń niezbędna jest wiedza dotycząca protokołu badania i interpretacji obrazu ultrasonograficznego. Niniejszy artykuł krok po kroku opisuje procedurę badania FAST.
Celem procedury FAST jest wykrycie wolnego płynu w jamie otrzewnowej oraz osierdziu. Kiedy u pacjenta obserwujemy niestabilność hemodynamiczną z oznakami anemizacji, możemy przyjąć, że nastąpił krwotok wewnętrzny. Dzięki temu badaniu pacjent może zostać szybko zdiagnozowany i przetransportowany bezpośrednio z karetki czy oddziału SOR na blok operacyjny, gdzie zostanie natychmiast zoperowany, bez niepotrzebnej straty czasu, który jest tak istotny dla zdrowia i życia pacjenta.
Wykonanie badania FAST w praktyce zespołu wyjazdowego ratownictwa medycznego może przyspieszyć decyzje dotyczące transportu pacjenta do centrum urazowego, a tym samym zwiększyć szanse pacjenta w przypadku krwawienia wewnętrznego.
Summary
Ultrasonography is a diagnostic tool used in emergency medicine, intensive care or surgery. Technological progress and the minimization of portable devices has made it possible to perform ultrasound examinations outside the hospital, including in emergency medical teams.
The ability to diagnose internal bleeding in patients with injuries is one of the key diagnostic elements. Performing ultrasound based on F.A.S.T., BLUE or FEEL protocols in the conditions of medical rescue teams can significantly shorten the time of diagnostics by directing the patient directly to the emergency room. Thanks to the progress in medical technology it is possible to perform ultrasonography with the use of mobile devices. In an increasing number of medical rescue teams, portable ultrasound devices are available. In order to use these devices effectively, it is necessary to know the protocol of examination and interpretation of ultrasound image. This article describes the F.A.S.T. procedure.
The purpose of the procedure is to detect free fluid in the peritoneal cavity and pericardium. When we observe hemodynamic instability with signs of anemia, we may assume that there has been internal hemorrhage. Thanks to this examination, the patient can be quickly diagnosed and transported directly from the ambulance or emergency department to the operating theatre, where he or she will be operated on immediately, without wasting unnecessary time, which is so important for the patient's health and life.
Performing the F.A.S.T. examination in the practice of the emergency medical team may speed up decisions regarding transporting the patient to the trauma center, thus increasing the chances of the patient in the case of internal bleeding.

INTRODUCTION
Ultrasonography allows to examine the patient without prior preparation and without any serious complications (1, 2). It is the fastest and one of the most accurate diagnostic forms (3). Such an examination can be performed in any place: street, ambulance, home of the injured person or emergency department.
Ultrasonography POC (Point of Care) is a relatively young field of ultrasonography, but the usefulness of protocols and research in this field is invaluable (4). Especially when the patient is unconscious, and it is impossible to collect an interview (5, 6). Intervention and Emergency Ultrasonography is not only for diagnostic purposes, it also allows to monitor the injured person’s condition by performing tests such as optic nerve shield control, which gives information about intracranial pressure (7).
The aim of POC ultrasonography is for medical staff to perform examinations in order to assess the current condition of the patient and, on the basis of the results of this examination, to take medical action (8). We must distinguish between these procedures and normal ultrasound examinations. In these procedures, we must treat the ultrasound machine as a “stethoscope” (3). And, as it is well known the stethoscope serves all medical personnel, not just physicians (9-13).
Focused Assessment with Sonography in Trauma (F.A.S.T.)
The purpose of the procedure is to detect free fluid (blood) in the peritoneal cavity and pericardium. When we observe hemodynamic instability with signs of anemia, we may assume that there has been internal hemorrhage (14). The quickest way to confirm this diagnosis is to perform the F.A.S.T. procedure. Thanks to this examination, the patient can be quickly diagnosed and transported directly from the ambulance or emergency department to the operating theatre, where he or she will be operated on immediately, without wasting unnecessary time, which is so important for the patient’s health and life (15, 16).
The F.A.S.T. (extended) examination is an extended examination of the chest area and is intended to check whether there is a fluid (blood) or pneumothorax (17).
The detection rate of free fluid in the abdominal cavity in patients after injuries by ultrasonography is about 75% (up to 95%). The specificity of the method is estimated at 98%. While physical examination is characterized by only 50-60% sensitivity.
It should be remembered that ultrasound examination in a patient after an injury is not used to assess the extent of injuries. The information from the examination is binary 0 – there is no liquid/air or 1 – there is liquid/air.
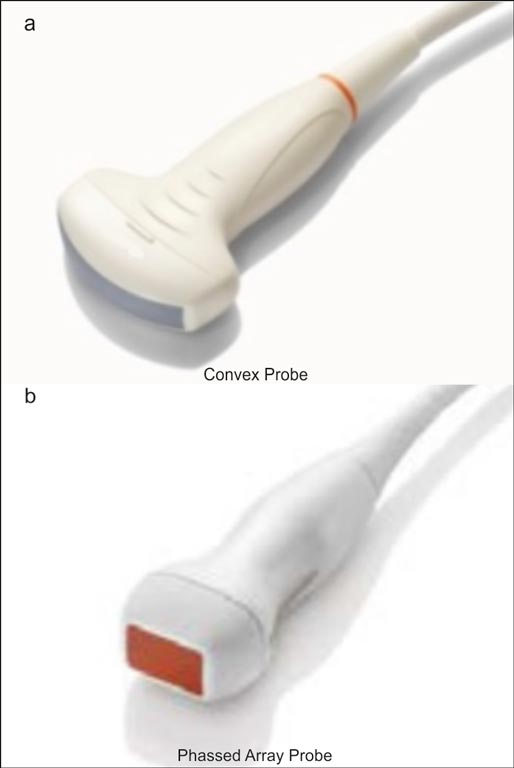
When performing the examination, we usually use a Convex-type transducer, commonly known as the abdominal transducer. If we do not have such a transducer, we can use a Phased Array transducer, i.e. a transducer known in Poland as a sectorial or cardiological transducer.
Projections in the F.A.S.T. examination
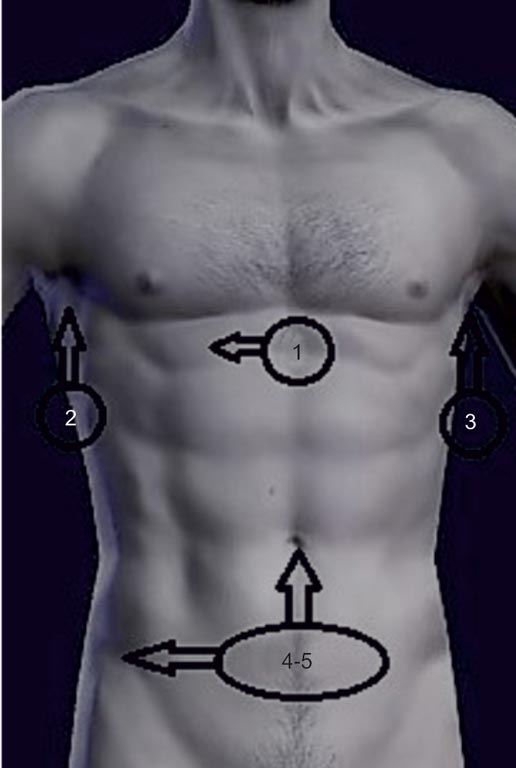
The entire procedure consists of 4 positions and 5 transducer positions in the abdomen, chest and pelvis (fig. 1). To perform the examination, we can use a Convex-type transducer or Phased Array transducer, i.e. a cardiologic transducer with positioning for abdominal application (fig. 2a, b). There are also devices that have dedicated settings for POC procedures (18).

Fig. 1. Locations of ultrasound transducer application during F.A.S.T. examination

Fig. 2a, b. Examples of probes: (a) Convex Probe; (b) Phased Array Probe
During the examination, the patient lies on a flat surface so that the fluid (blood) flows gravitationally into the free space.
The procedure begins with a subcostal projection in which the heart and pericardium are evaluated. We start with this position, because if we do not observe the movement of the heart, it does not make sense to continue the procedure.
Subcostal projection
Position of the transducer and test space: beneath the spinous process in a transverse plane with the probe marker facing right (right side of the patient). The probe is at a large angle and faces the left side of the chest. We increase the depth of penetration of the device so that the image shows the whole heart, part of the liver, diaphragm and lungs (19). During this projection we have to use the appropriate pressure force to obtain the image of the heart from under the ribs. In the absence of the desired image, gentle fan and left-right movements are performed.
Powyżej zamieściliśmy fragment artykułu, do którego możesz uzyskać pełny dostęp.
Mam kod dostępu
- Aby uzyskać płatny dostęp do pełnej treści powyższego artykułu albo wszystkich artykułów (w zależności od wybranej opcji), należy wprowadzić kod.
- Wprowadzając kod, akceptują Państwo treść Regulaminu oraz potwierdzają zapoznanie się z nim.
- Aby kupić kod proszę skorzystać z jednej z poniższych opcji.
Opcja #1
29 zł
Wybieram
- dostęp do tego artykułu
- dostęp na 7 dni
uzyskany kod musi być wprowadzony na stronie artykułu, do którego został wykupiony
Opcja #2
69 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 30 dni
- najpopularniejsza opcja
Opcja #3
129 zł
Wybieram
- dostęp do tego i pozostałych ponad 7000 artykułów
- dostęp na 90 dni
- oszczędzasz 78 zł
Piśmiennictwo
1. Whitson MR, Mayo PH: Ultrasonography in the emergency department. Crit Care 2016; 20(1): 227.
2. Marin JR, Lewiss RE; American Academy of Pediatrics, Committee on Pediatric Emergency Medicine; Society for Academic Emergency Medicine, Academy of Emergency Ultrasound; American College of Emergency Physicians, Pediatric Emergency Medicine Committee; World Interactive Network Focused on Critical Ultrasound: Point-of-care ultrasonography by pediatric emergency medicine physicians. Pediatrics 2015; 135(4): e1113-1122.
3. Sekiguchi H: Tools of the Trade: Point-of-Care Ultrasonography as a Stethoscope. Semin Respir Crit Care Med 2016; 37(1): 68-87.
4. Bøtker MT, Jacobsen L, Rudolph SS et al.: The role of point of care ultrasound in prehospital critical care: a systematic review. Scand J Trauma Resusc Emerg Med 2018; 26(1): 51.
5. Bhagra A, Tierney DM, Sekiguchi H et al.: Point-of-Care Ultrasonography for Primary Care Physicians and General Internists. Mayo Clin Proc 2016; 91(12): 1811-1827.
6. Moore CL, Copel JA: Point-of-care ultrasonography. N Engl J Med 2011; 364(8): 749-757.
7. Lee SW, Tiu T, Roberts J et al.: Point-of-Care Ultrasonography Findings and Care Use Among Patients Undergoing Ultrasound-Guided Shoulder Injections. Am J Phys Med Rehabil 2018; 97(1): 56-61.
8. Fornell Pèrez R: Focused assessment with sonography for trauma (FAST) versus multidetector computed tomography in hemodynamically unstable emergency patients. Radiologia 2017; 59(6): 531-534.
9. Merlini DA, Castoldi M, Pisoni L et al.: F.A.S.T. Ultrasound for emergency surgeon. Ann Ital Chir 2007; 78(2): 141-144.
10. Marsh-Feiley G, Eadie L, Wilson P: Paramedic and physician perspectives on the potential use of remotely supported prehospital ultrasound. Rural Remote Health 2018; 18(3): 4574.
11. McCallum J, Vu E, Sweet D et al.: Assessment of Paramedic Ultrasound Curricula: A Systematic Review. Air Med J 2015; 34(6): 360-368.
12. Szarpak L, Truszewski Z, Kurowski A et al.: Knowledge, attitude, and practices of paramedics regarding optic nerve sheath diameter ultrasonography. Am J Emerg Med 2016; 34(6): 1160-1161.
13. Oliveira L, Lawrence M: Ultrasound-Guided Peripheral Intravenous Access Program for Emergency Physicians, Nurses, and Corpsmen (Technicians) at a Military Hospital. Mil Med 2016; 181(3): 272-276.
14. Kim CH, Shin SD, Song KJ et al.: Diagnostic accuracy of focused assessment with sonography for trauma (FAST) examinations performed by emergency medical technicians. Prehosp Emerg Care 2012; 16(3): 400-406.
15. Richards JR, McGahan JP: Focused Assessment with Sonography in Trauma (FAST) in 2017: What Radiologists Can Learn. Radiology 2017; 283(1): 30-48.
16. Savatmongkorngul S, Wongwaisayawan S, Kaewlai R: Focused assessment with sonography for trauma: current perspectives. Open Access Emerg Med 2017; 9: 57-62.
17. Calder BW, Vogel AM, Zhang J et al.: Focused assessment with sonography for trauma in children after blunt abdominal trauma: A multi-institutional analysis. J Trauma Acute Care Surg 2017; 83(2): 218-224.
18. Patel NY, Riherd JM: Focused assessment with sonography for trauma: methods, accuracy, and indications. Surg Clin North Am 2011; 91(1): 195-207.
19. McMurray J, Boysen S, Chalhoub S: Focused assessment with sonography in nontraumatized dogs and cats in the emergency and critical care setting. Vet Emerg Crit Care (San Antonio) 2016; 26(1): 64-73.
20. Sue K: The occasional ED ultrasound: focused assessment with sonography for trauma (FAST). Can J Rural Med 2015; 20(1): 33-39.
21. O’Brien KM, Stolz LA, Amini R et al.: Focused Assessment With Sonography for Trauma Examination: Reexamining the Importance of the Left Upper Quadrant View. J Ultrasound Med 2015; 34(8): 1429-1434.
22. Sauter TC, Hoess S, Lehmann B et al.: Detection of pneumothoraces in patients with multiple blunt trauma: use and limitations of eFAST. Emerg Med J 2017; 34(9): 568-572.
23. Montoya J, Stawicki SP, Evans DC et al.: From FAST to E-FAST: an overview of the evolution of ultrasound-based traumatic injury assessment. Eur J Trauma Emerg Surg 2016; 42(2): 119-126.
24. Pencil K: eFAST Simulation Training for Trauma Providers. J Trauma Nurs 2017; 24(6): 376-380.