Tomasz Lis, *Lidia Zawadzka-Głos
Adenoidectomy and adenotonsillotomy in patients treated in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw in 2018 – a retrospective analysis
Adenotomia i adenotonsillotomia u pacjentów Kliniki Otolaryngologii Dziecięcej Warszawskiego Uniwersytetu Medycznego w 2018 roku ? analiza retrospektywna
Department of Paediatric Otorhinolaryngology, Medical University of Warsaw
Head of Department: Lidia Zawadzka-Głos, MD, PhD
Streszczenie
Wstęp. Adenotomia i adenotonsillotomia są jednymi z najczęściej wykonywanych zabiegów chirurgicznych na świecie. Dwie główne kategorie wskazań do adenotomii i adenotonsillotomii stanowią zaburzenia oddychania w czasie snu oraz nawracające infekcje górnych dróg oddechowych.
Cel pracy. Celem tej pracy była analiza wykonanych zabiegów adenotomii i adenotonsillotomii w Klinice Otolaryngologii Dziecięcej Warszawskiego Uniwersytetu Medycznego w 2018 roku.
Materiał i metody. Badaniem objęto grupę 474 pacjentów w wieku od 11 miesięcy do 18 lat, których poddano leczeniu operacyjnemu adenotomii i adenotonsillotomii w Klinice Otolaryngologii Dziecięcej Warszawskiego Uniwersytetu Medycznego w 2018 roku. Zgromadzone dane objęły: wiek, płeć, czas pobytu na oddziale oraz diagnozy dodatkowe rozpoznania przerostu migdałka gardłowego lub migdałka gardłowego i migdałków podniebiennych. Przeanalizowano również mniejsze zabiegi, które towarzyszyły usunięciu migdałków.
Wyniki. W 2018 roku 472 pacjentów poddano adenotomii lub adenotonsillotomii. Zabieg adenotonsillotomii był wykonywany prawie dwukrotnie częściej. U niemal 1/3 dzieci przerostowi migdałków towarzyszyło wysiękowe zapalenie uszu, a u około 1/5 konieczny był drenaż wentylacyjny uszu. Średni czas pobytu na oddziale wyniósł 4,19 ± 1,44 dnia.
Wnioski. Wykazaliśmy, że większość zabiegów przeprowadzonych w Klinice Otolaryngologii Dziecięcej to adenotonsillotomie. Najczęstszą diagnozą dodatkową było wysiękowe zapalenie uszu, a zabiegiem towarzyszącym drenaż wentylacyjny. Zazwyczaj czas hospitalizacji ograniczał się do 3 dni.
Summary
Introduction. Adenoidectomy and adenotonsillotomy are among the most common surgical procedures worldwide. Sleep-related breathing disorders and recurrent upper respiratory tract infections are two primary categories of indications for adenoidectomy and adenotonsillotomy.
Aim. The aim of this study was to analyse selected adenoidectomy and adenotonsillotomy procedures performed in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw in 2018.
Material and methods. A total of 474 patients aged between 11 months and 18 years, who underwent adenoidectomy and adenotonsillotomy in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw in 2018, were included in the study. Data on age, gender, length of hospital stay, as well as additional diagnoses in adenoid hypertrophy or adenoid and palatine tonsil hypertrophy were collected. Minor surgeries performed in addition to tonsillectomy were also evaluated.
Results. A total of 472 patients underwent adenoidectomy and adenotonsillotomy in 2018. Adenotonsillotomy was almost twice more common. Tonsillar hypertrophy was accompanied by exudative otitis media in almost 1/3 of children, and ear ventilation tubes were needed in almost 1/5 of children. Mean hospital stay equaled 4.19 ± 1.44 days.
Conclusions. We have shown that adenotonsillotomy was the most common procedure in the Department of Paediatric Otorhinolaryngology. Exudative otitis media was the most common concomitant diagnosis, and middle ear ventilation was the most common additional procedure. Hospital stay usually lasted 3 days.
Introduction
Adenoidectomy (with or without tonsillectomy) is one of the most common surgeries, with about 43,192 procedures performed annually in Poland (latest data) (1). Sleep-related breathing disorders and recurrent upper respiratory tract infections are two primary categories of indications for adenoidectomy and adenotonsillotomy (2). Adenoidectomy may be performed independently of or in combination with tonsillectomy or other procedures, such as middle ear ventilation tube placement, nasal surgeries, tonsillectomy (3-5).
Aim
The aim of this study was to analyse selected adenoidectomy and adenotonsillotomy procedures performed in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw in 2018.
Material and methods
A total of 474 patients aged between 11 months and 18 years, who underwent adenoidectomy and adenotonsillotomy in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw in 2018, were included in the study. This was a retrospective study. The surgeries were performed by a laryngologist or a paediatric laryngologist, separately or in combination with other minor laryngological procedures. One of the patients undergoing an additional major surgery and one patient undergoing adenotonsillectomy were excluded from the study; therefore, the final sample size was 472 patients. Patients undergoing tonsillectomy for other indications were not included. Patients subject to isolated tonsillotomy were also excluded due to their low number (5) and the fact that tonsillotomy was performed additionally to other, more extensive procedures as a result of contraindicated simultaneous removal of the adenoid due to a submucous cleft palate.
Data on age, gender, length of hospital stay, as well as additional diagnoses other than adenoid hypertrophy or adenoid and palatine tonsil hypertrophy were collected. Minor surgeries performed in addition to tonsillectomy were also analysed.
Results
A total of 472 patients underwent adenoidectomy or adenotonsillotomy procedures performed by 17 laryngologists or paediatric laryngologists between January 1, 2018 and December 31, 2018. The adenoid was removed in 162 (34.32%) children, while 310 (65.68%) patients underwent adenoid surgery accompanied by partial resections of palatine tonsils. There were 175 girls and 297 boys aged between 11 months and 16 years (5.83 ± 2.77) in the study group.
No additional diagnoses were made in 180 (38.14%) patients. Data for the remaining 292 (61.86%) patients is summarised in table 1. Most of these patients were co-diagnosed with exudative otitis media (148, 31.36%) and conductive hearing loss (33, 6.99%) (tab. 1).
Tab. 1. Concomitant diagnoses (10 most common)
| Diagnosis | ICD-10 code | Number of patients | % |
| Nonsuppurative otitis media | H65 | 148 | 31.36 |
| Conductive and sensorineural hearing loss | H90 | 33 | 6.99 |
| Other coagulation defects | D68 | 29 | 6.14 |
| Other congenital malformations of tongue, mouth and pharynx | Q38 | 21 | 4.45 |
| Other and unspecified disorders of nose and nasal sinuses | J34 | 20 | 4.24 |
| Sleep disorders | G47 | 14 | 2.97 |
| Chronic rhinosinusitis | J32 | 11 | 2.33 |
| Other specified diseases of upper respiratory tract | J39 | 7 | 1.48 |
| Diseases of vocal cords and larynx, not elsewhere classified | J38 | 5 | 1.06 |
| Asthma | J45 | 4 | 0.85 |
Minor procedures performed in addition to adenoidectomy or adenotonsillotomy are summarised in table 2. These mainly included ventilation tube placement in 88 (18.64%) patients, and tongue frenulum repair in 18 (3.81%) patients.
Tab. 2. Minor procedures performed in addition to adenoidectomy or adenotonsillotomy
| Additional procedures | Number of patients | % |
| Ventilation tubes placement | 88 | 18.64 |
| Tongue frenulum repair | 18 | 3.81 |
| Turbinate surgery | 1 | 0.21 |
| Resection of preauricular sinus and cyst | 1 | 0.21 |
Mean duration of hospital stay was 4.19 ± 1.44 days. The shortest and the longest hospital stay were 2 and 10 days, respectively. The largest number of children, i.e. 218 (46.19%), were hospitalised in the Department for 3 days.
Discussion
The adenoid (pharyngeal tonsil) and palatal tonsils make up a part of the Waldeyer’s lymphatic ring and play an important role in the development of the immune memory in young children (6). Adenoid hypertrophy occurs during the first 4 years of life, and undergoes atrophy between 6 and 16 years of age (7). Palatal tonsils also involute during adolescence.
Adenoid hypertrophy is one of the most common paediatric health problems requiring surgical management (fig. 1-3) (8). It is accompanied by the hypertrophy of the palatal tonsils in a large proportion of patients. Our study showed that adenotonsillotomy was twice more common.
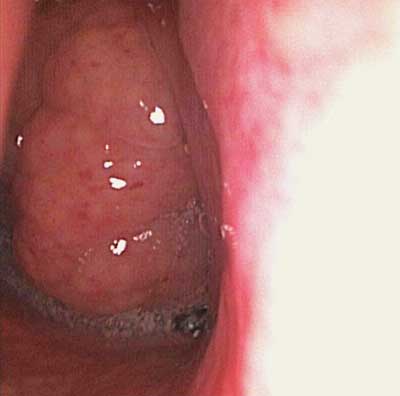
Fig. 1. Pharyngeal tonsil hypertrophy. The pharyngeal tonsil obscures over 90% of the nasopharynx

Fig. 2. Pharyngeal tonsil not hypertrophed

Fig. 3. Palatal tonsils hyperthrophy
A hypertrophied adenoid causes compression of the pharyngeal opening of the auditory tube, thereby blocking it. This impairs normal ventilation of the middle ear and predisposes to exudative otitis media. This is a common symptom seen in patients with adenoid hypertrophy, which was also demonstrated in our study. Resection of the adenoid as the cause of exudative otitis media should lead to the resolution of inflammatory lesions in the tympanic cavity (9). However, since the lesions are very advanced in some cases, adenoidectomy is accompanied by ventilation tube placement to prevent exudate accumulation in the middle ear and ensure ventilation. Our study showed that ventilation tube placement was the most common additional procedure accompanying adenoidectomy or adenotonsillotomy.
Resection of a hypertrophied adenoid requires postoperative monitoring due to the risk of possible post-operative complications. Symptoms which may prolong hospital stay include, among others, bleeding, insufficient pain control, nausea and vomiting, as well as difficulty eating (10). Haematological disorders, complications after anaesthesia and social reasons may also prolongate hospital stay.
The study’s limitations include the fact that tympanocentesis, which is a common concomitant surgery, was not considered as a common additional procedure due to its absence in the IT system. Hospital stay may also fail to reflect the actual and clinically justified length of hospitalisation due to the nature of the Department (admission on the day before the procedure) or possible delay due to the organisation in the operating block.
Conclusions
We demonstrated that adenotonsillotomy is the most common surgery performed in the Department of Paediatric Otorhinolaryngology. Exudative otitis media was the most common co-diagnosis, and ventilation tube placement was the most common additional procedure. Hospital stay was usually limited to 3 days.
Piśmiennictwo
1. https://statystyki.nfz.gov.pl z 2017 roku.
2. Rosenfeld RM, Green RP: Tonsillectomy and adenoidectomy: changing trends. Ann Otol Rhinol Laryngol 1990; 99: 187-191.
3. Marcus CL, Moore RH, Rosen CL et al.: A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med 2013; 368: 2366-2376.
4. Van Den Akker EH, Hoes AW, Burton MJ, Schilder AG: Large international differences in (adeno)tonsillectomy rates. Clin Otolaryngol Allied Sci 2004; 29: 161-164.
5. Haapkylä J, Karevold G, Kvaerner KJ, Pitkäranta A: Trends in otitis media surgery: a decrease in adenoidectomy. Int J Pediatr Otorhinolaryngol 2008; 72: 1207-1213.
6. Wysocka J, Hassmann E, Lipska A, Musiatowicz M: Naive and memory T cells in hypertrophied adenoids in children according to age. Int J Pediatr Otorhinolaryngol 2003; 67: 237-241.
7. Brodsky L, Koch RJ: Bacteriology and immunology of normal and diseased adenoids in children. Arch Otolaryngol Head Neck Surg 1993; 119: 821-829.
8. Darrow DH, Siemens C: Indications for tonsillectomy and adenoidectomy. The Laryngoscope 2002; 112: 6-10.
9. Paradise JL, Bluestone CD, Rogers KO et al.: Efficacy of adenoidectomy of recerrent otitis media in children previously treated with tympanostomy-tube placement: results of parallel randomized and nonrandomized trials. JAMA 1990; 263: 2006-2073.
10. Drake-Lee A, Stokes M: A prospective study of the length of stay of 150 children following tonsillectomy and/or adenoidectomy. Clin Otolaryngol 1998; 23: 491-495.



