Maria Wolniewicz, *Lidia Zawadzka-Głos
Indications for tympanostomy tube insertion in children
Wskazania do drenażu wentylacyjnego u dzieci
Department of Paediatric Otorhinolaryngology, Medical University of Warsaw
Head of Department: Lidia Zawadzka-Głos, MD, PhD
Streszczenie
Wstęp. Drenaż wentylacyjny jest jednym z podstawowych zabiegów z zakresu laryngologii dziecięcej. Podstawowe wskazanie do planowej kwalifikacji do zabiegu stanowi wysiękowe zapalenie ucha środkowego (OME). Nie ma aktualnie zaleceń, które propagowałyby farmakologiczne metody leczenia wysięku. W przypadkach nawracających zapaleń ucha środkowego czy ostrych powikłaniach zapalenia ucha środkowego często jest to procedura wykonywana z wyboru jako uzupełnienie antybiotykoterapii ogólnoustrojowej.
Cel pracy. Celem głównym pracy była analiza wskazań do zabiegu drenażu wentylacyjnego, natomiast cele wtórne stanowiły charakterystyka badanej populacji oraz ocena kondycji błony bębenkowej w momencie wykonywania zabiegu.
Materiał i metody. Przeanalizowano retrospektywnie procedury drenażu wentylacyjnego przeprowadzone w Klinice Otolaryngologii Dziecięcej WUM od 1 stycznia do 31 grudnia 2018 roku.
Wyniki. W 2018 roku w Klinice Otolaryngologii Dziecięcej WUM zabiegowi drenażu wentylacyjnego zostało poddanych 213 dzieci (wiek od 2. miesiąca życia do 18 lat) i założono 368 drenów, głównie z powodu wysiękowego zapalenia ucha środkowego. Zabiegi planowe stanowiły 69,48%. Na drugim miejscu znalazły się nawracające stany zapalne ucha środkowego (22,07%) oraz powikłania ostrego zapalenia ucha środkowego, przede wszystkich ostre zapalenie wyrostka sutkowatego (23,33% zabiegów w trybie pilnym). W przeważającej większości umieszczano w błonie bębenkowe dreny typu Mikołów, w pojedynczych przypadkach dreny długoterminowe (14 drenów typu T, 7 drenów typu Paparella). Dominujący charakter wysięków stanowił wysięk śluzowy (62,44%). W ponad połowie przypadków (62,44%) przeprowadzono drenaż jako samodzielną procedurę, natomiast prawie 1/3 zabiegów była wykonana wraz z adenotomią. U 28 pacjentów (13,14%) w momencie zabiegu stwierdzono mikroskopowo zmiany w obrębie błony bębenkowej świadczące o zaawansowaniu przewlekłego stanu zapalnego.
Wnioski. Zabieg drenażu, choć powszechnie akceptowalny, nie jest procedurą pozbawioną negatywnych konsekwencji. Możliwe powikłania obejmują: przetrwałą perforację błony bębenkowej, tympanosklerozę, przedwczesne wypadnięcie drenu wentylacyjnego, wyciek z ucha, zaburzenia drożności drenu, czasami konieczność operacyjnego usunięcia drenu. Zatem wykonanie zabiegu wymusza stałą i regularną opiekę laryngologiczną.
Summary
Introduction. Tympanostomy tube insertion is one of the basic paediatric otolaryngological procedures.
Otitis media with effusion (OME) is the primary indication for elective qualification for this procedure. Currently, there are no recommendations suggesting pharmacotherapy for effusion. In cases of recurrent otitis media or acute complications of otitis media, tube insertion is a method of choice to support systemic antibiotic therapy.
Aim. The main aim of this study was to evaluate indications for tympanostomy tube insertion. Secondary aims included characteristics of the study population and an intraoperative assessment of the tympanic membrane.
Material and methods. We conducted a retrospective analysis of ear tube placement procedures performed in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw between January 1, 2018 and December 31, 2018.
Results. A total of 213 children (aged between 2 months and 18 years) underwent tympanostomy tube insertion and a total of 368 tubes were placed due to otitis media with effusion in 2018 in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw. Elective tube insertion accounted for 69.48% of procedures. Recurrent otitis media (22.07%), complications of acute otitis media and, most of all, acute mastoiditis (23.33% of urgent procedures) came second. In a large majority of cases, Mikolow tympanostomy tubes were placed; in isolated cases, long-term tympanostomy tubes were used (14 T-tubes, 7 Paparella tubes). Mucous effusion dominated (62.44%). Ear tube placement alone was performed in more than half of cases (62.44%), while in 1/3 of patients the procedure was combined with adenoidectomy. Microscopically confirmed tympanic lesions indicative of advanced inflammation were found in 28 patients (13.14%).
Conclusions. Although commonly accepted, tympanostomy tube insertion is not devoid of negative consequences. Possible complications include persistent tympanic perforation, tympanosclerosis, premature extrusion of an ear tube, ear discharge, tube obstruction and, in some cases, the need for surgical tube removal. Therefore, the procedure requires permanent and systematic otolaryngological care.
Introduction
Tympanostomy tube insertion (grommets) is one of the basic otolaryngological procedures performed in children (1). Otitis media with effusion (OME), which is defined as fluid retention behind the eardrum for at least 3 months, accompanied by 25-30 dB hearing loss, is the primary indication for elective tube insertion (2, 3). A more individual approach is needed in children with Down syndrome or craniofacial defects, including cleft palate, due to an increased predisposition to fluid secretion and its long-term persistence (2, 3).
OME is diagnosed annually in about 2.2 million children in the USA (2). It affects about 50-90% of children < 5 years of age (2), and 667 000 children below 15 years of age undergo ear tube insertion (1).
Fluid retention behind the eardrum is due to Eustachian tube dysfunction and occurs in upper respiratory tract infections or as an inflammatory response to previous inflammation, representing a residual phase of acute otitis media. However, fluid retention should last no longer than 3 months, which is considered a persistent condition, and which may consequently lead to permanent remodelling of the tympanic membrane and cavity. Such a conductive hearing loss (0-50 dB, 28 dB on average) is believed to affect child’s development, causing ear discomfort, sleeping disorders, worse speech development, poor learning results compared to healthy peers, or behavioural problems, such as problems with balance (2). This is currently the most common cause of hearing loss in developed countries (2).
Both US and UK guidelines recommend careful observation and, optionally, surgical intervention instead of pharmacologic management of effusion (steroids, antibiotics, antihistamines, mucosal decongestants, antireflux therapy) (2, 3). As outlined in the US guidelines, adenoidectomy with or without grommets is recommended for children aged > 4 years, while tympanostomy tube insertion is recommended in younger children unless there is clinical evidence of adenoid hypertrophy. British guidelines recommend concurrent adenoidectomy in children with persistent and/or frequent upper respiratory tract infections (URTIs) (3).
Recurrent acute otitis media (rAOM), usually defined as 4 inflammatory episodes within 12 months or 3 episodes within 6 months, is another indication for grommets (4). It may be performed in an elective mode, during subsequent recurrent AOT and indicated myringotomy, or as the final stage of treatment for recurrent otitis media.
Tympanostomy tube insertion in rAOM is a more debatable issue. The therapeutic effect is less clear and, according to multiple analyses, including the Cochrane database, further research to assess its efficacy is needed (5).
Urgent procedures due to complications of acute suppurative otitis media are the third group of indications.
Although commonly accepted, tympanostomy tube insertion is not devoid of negative consequences. Possible complications include persistent tympanic perforation, tympanosclerosis, premature extrusion of an ear tube, ear discharge, tube obstruction and, in some cases, the need for surgical tube removal.
Aim
The main aim of this study was to evaluate indications for tympanostomy tube insertion. The characteristics of study population and an intraoperative assessment of the tympanic membrane were secondary aims.
Material and methods
We performed a retrospective analysis of ear tube placement procedures performed in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw between January 1, 2018 and December 31, 2018, using the CGM Clininet system. Data on indications for the procedure, mode of procedure (elective vs. urgent), otolaryngological history, and the course of procedure, including the state of the tympanic membrane, and the presence/properties of fluid behind the membrane, were analysed. Microsoft Excel was used for data collection and analysis.
Results
A total of 213 children aged between 2 months and 18 years (mean age about 4.5 years, SD about 2.8 months) and median age 4 years and 1.5 months underwent tympanostomy tube insertion in 2018 in the Department of Paediatric Otorhinolaryngology of the Medical University of Warsaw. Boys accounted for 63.38%. A total of 368 tubes were inserted in the eardrum, including 177 in the right and 191 in the left ear. Otitis media with effusion (fig. 1), accounting for 59.15%, alone or in combination with rOM (7.98%), was the primary indication for the procedure. Recurrent AOM came second (22.07%).
Fig. 1. Indications for tympanostomy tube insertion
There were 69.48% of elective procedures, 28.17% urgent and 2.35% accelerated urgent procedures as the final stage of treatment of recurrent inflammation (fig. 2).
Fig. 2. Mode of procedure
Indications were dominated by otitis media and its complications, usually in the form of acute mastoiditis (23.33%): bilateral in 1 patient, concomitant with nerve VII paresis in 1 case and concomitant with thrombosis of the sigmoid sinus in 1 patient. Other complications included isolated labyrinthitis (6.67%), including 1 bilateral; and peripheral nerve VII paresis (5.00%). In one case, grommet insertion was performed due to sudden hearing loss and identification of mucous effusion behind the eardrum, which was successfully treated with an additional use of hyperbaric oxygen therapy and vitamin supplementation.
The vast majority of tubes used in our center are Mikolow tympanostomy tubes (94.32%). We also used long-term ear tubes: 14 T-tubes and 7 Paparella tubes. They were placed in children with a history of several otolaryngological interventions (AT and/or tympanocentesis and/or grommet(s) (50.00%; 30% for repeated tube insertion) or with submucous cleft palate (30.00%).
Tympanic tube insertion was performed as an independent intervention in more than half of cases (62.44%). Adenoidectomy, optionally with tonsillotomy, was the most common additional procedure (repeated procedure in 2.35%), accounting for 32.39%. In some acute cases, concurrent antromastoidectomy was performed ? about 5.16% of complex procedures. Eleven patients received an indication for adenoidectomy within a follow up of 5 months to 1 year and 5 months.
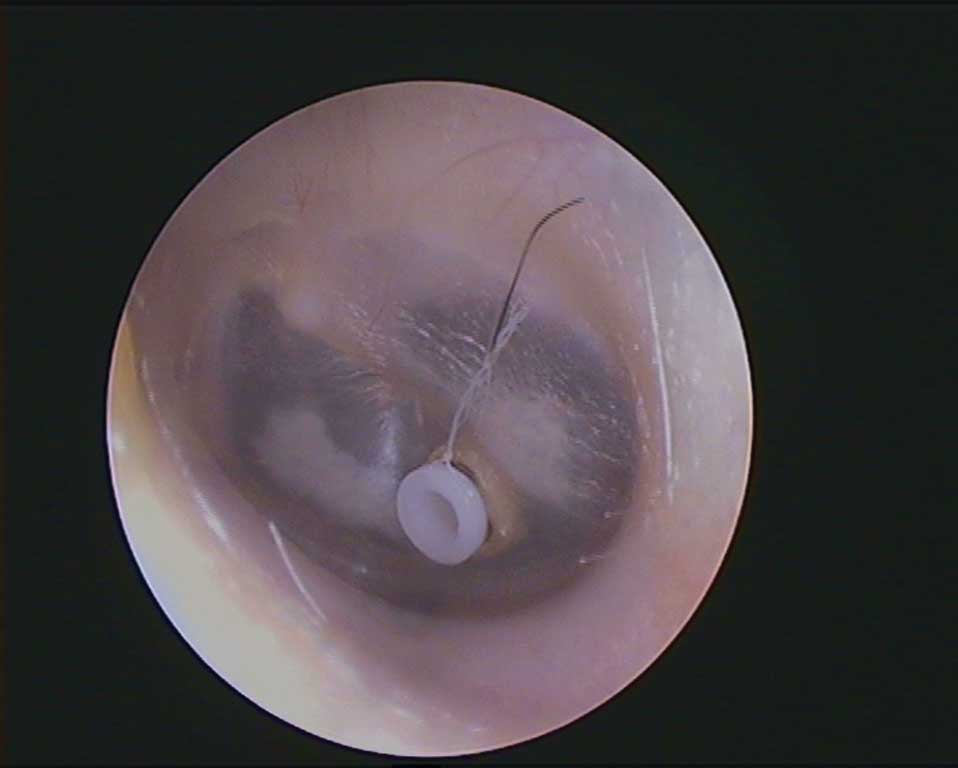
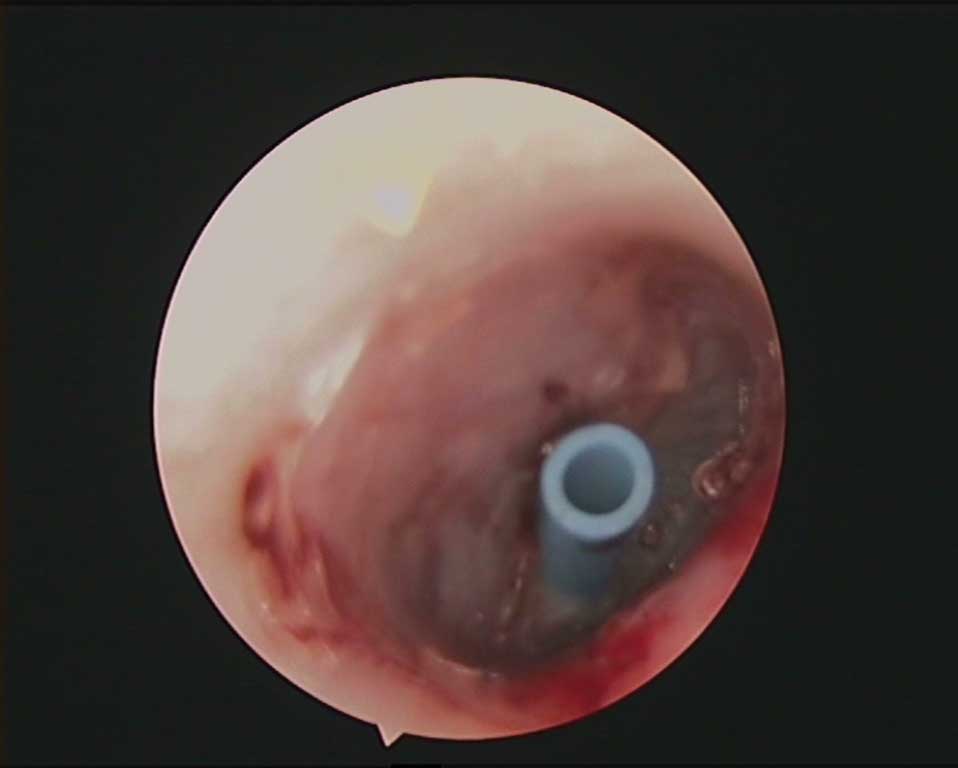
Among 285 ears with nonsuppurative effusion, there were 107 mucous effusions for the right ear and 104 for the left ear (mucous effusions accounted for 74.03%), and 37 cases of serous effusion for both right and left ear (serous effusions accounted for 25.96%) (fig. 3-5). Single cases of Eustachian tube obstruction in patients with grommets were reported (fig. 6).

Fig. 3. Leaft ear/eardrum, tympanovstomy tube type Mikołów (about 1 month after insertion)

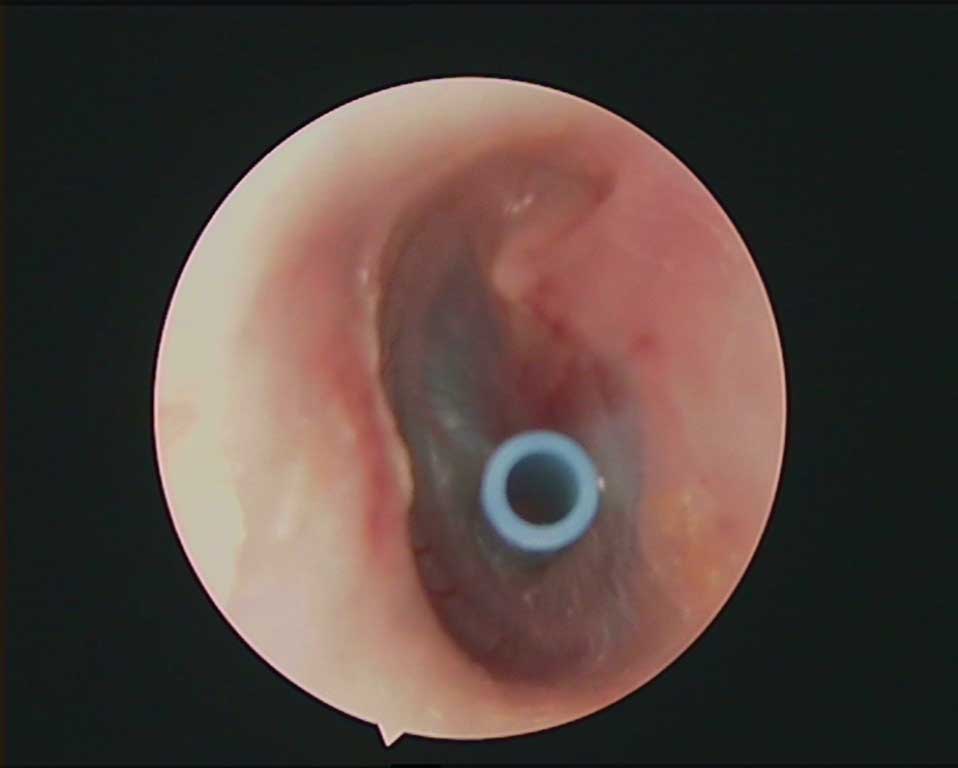
Fig. 4. Left ear/eardrum, tympanovstomy tube type T

Fig. 5. Right ear/eardrum, tympanovstomy tube type T
Fig. 6. Type of effusion
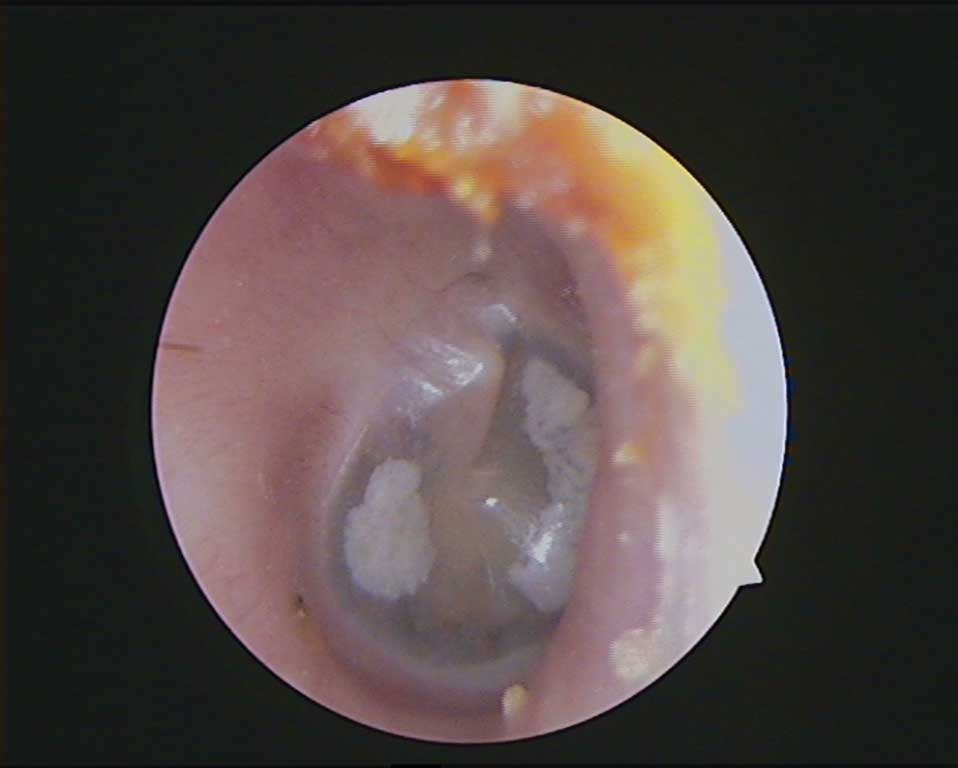
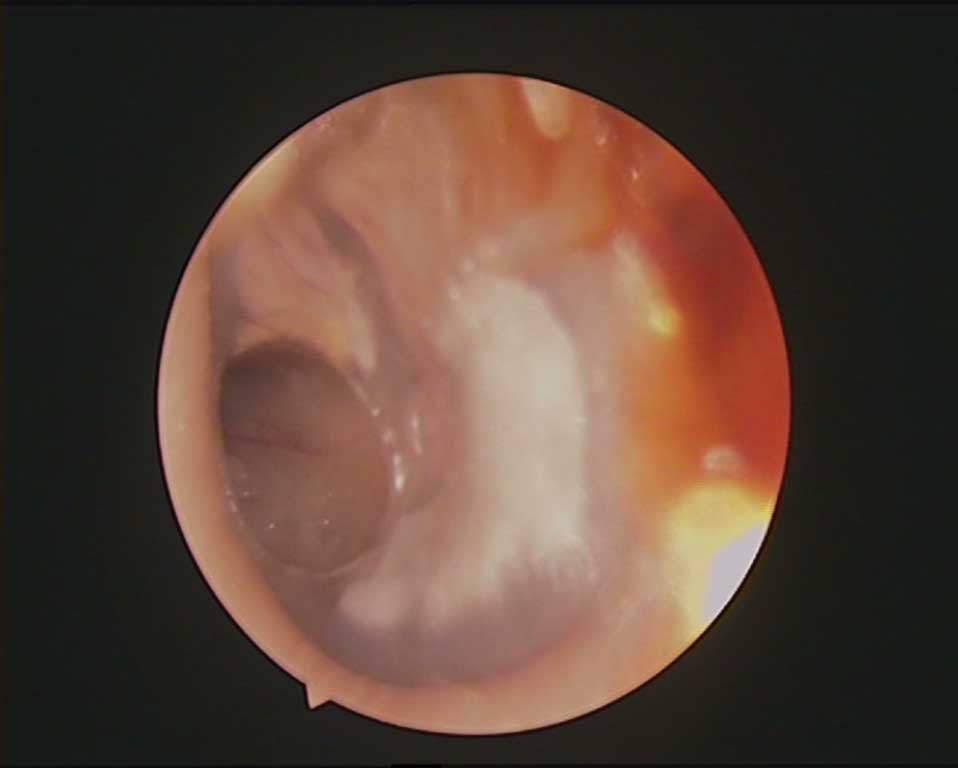
Microscopically confirmed tympanic lesions indicative of an ongoing chronic inflammation, which most of all included retraction pockets and severe eardrum retraction (with the signs of adhesion to the promontorium) were reported in 28 patients and for 35 ears, accounting for 36.84 and 26.31% of the described ear lesions, respectively (fig. 7). Tympanosclerosis and tympanic atrophy were also common, with each lesion reported for almost 16% of children (15.79%). Tympanosclerosis occurred in 4 children, 50% of whom had a history of repeated surgical interventions for the treatment of tympanic membrane, and 25% of whom had recurrent otitis media with effusion. Although no recurrent otitis media or tympanic interventions were reported for the fourth child, the patient had a history of early-childhood asthma diagnosed at the age of 4 months (fig. 8, 9).

Fig. 7. Tympanic lesions

Fig. 8. Right ear/eardrum, tympanosclerosis
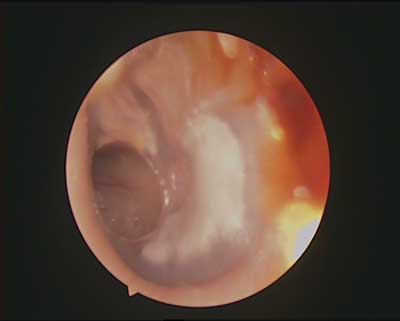
Fig. 9. Left ear/eardrum, permanent perforation after tympanovstomy tube placement
Discussion
The collected data on study population correspond to other population data from the Swedish grommet register, where the mean age at surgery is 4 years, male gender predominates (60%), and OME is the primary indication (6). Recently, two articles (2016 and 2017), presenting recurrent otitis media as the most common indication for ear tubes, were published. However, it can be noticed that, as in the Swedish population, recurrent otitis media is a more common indication for tympanostomy tube insertion in the younger age group (mean 3.29 ± 1.78; even 2.6 years in the Swedish population) than otitis media with effusion (mean 4.83 ± 2.46) (6).
According to an analysis of Cochrane database, hearing improvement in OME is evident 6-9 months after the surgery; however, the improvement becomes less pronounced within 12 and 18 months after the procedure (8). Due to the lack of continued postoperative care provided by a hospital outpatient clinic, it was not possible to evaluate the outcome of implemented treatment for chronic ear conditions. Also, the lack of electronic records of objective hearing examinations made it impossible to verify qualification criteria or therapeutic outcomes. In the Swedish registry, pure tone audiometry was possible in 51% of patients, including 53% of patients meeting the criteria for tube insertion (7).
Increasing attention is now being drawn to the involvement of bacterial biofilm in the pathomechanism of OME. In our Department, effusion fluids are routinely sent for bacteriological testing. However, literature reports show that despite negative bacterial cultures in most patients, a more detailed analysis of effusion often reveals bacterial genetic material: up to 94.5-100% for positive cultures about 19-60% (9, 10, 11), including DNA and mRNA, indicating metabolic activity, as well as bacterial proteins alone (9, 10, 12).
This bacterial microstructure is likely to be responsible for antibiotic resistance in chronic otitis. Standard therapy kills bacteria present in the structure periphery, but it does not reach the entire core, which is still able to restore the partially destroyed structure (12). Based on the analysis, about 1000-fold increase in resistance vs. independently functioning bacteria is reported (1).
The literature model of biofilm formation in chronic otitis media was induced in the chinchilla (12). New and promising studies focus on the analysis of extracellular polymeric substances (EPM), which have a protective function for residual bacteria by maintaining biofilm integrity, and which help adhere to the extracellular environment: eDNA (extracellular DNA), DNABII (a family of DNA-binding proteins), IHF (integration host factor), HU (histone-like protein) (9), as well as on the efficacy of monoclonal antibodies directed against DNABII in biofilm destabilisation (9). Bacterial biofilm components have been also identified in ear discharge following tube insertion (DNABII in particular) (1).
Therapeutic options for recurrent otitis media usually proposed by authors include antibiotic prophylaxis, adenoidectomy, tympanostomy tube insertion or their combination. Comparison of different approaches proposed by different centres is also difficult due to the large variation of qualification criteria for this procedure, patients’ age, the course of procedure and the follow-up period. One meta-analysis assessed the effects of each intervention at 3 levels: recurrence of otitis media, the rate of recurrence of otitis media and the total period of recurrent otitis media during follow-up. Antibiotic prophylaxis had the greatest impact on reduced recurrences, followed by adenoidectomy, whereas tympanostomy tube insertion seemed to increase the incidence. The rate of episodes was also reduced most effectively by antibiotic prophylaxis, followed by tube insertion. For total duration of the disease, the majority of positive reports concerned tympanostomy tubes, followed by antibiotic therapy. As shown in the presented papers, adenoidectomy showed varying and difficult to interpret effects in terms of both recurrence rates and total duration of the disease (6).
Antibiotic prophylaxis seems to be even more debatable considering that viral upper respiratory tract infections are a prerequisite for the development of otitis media despite bacterial aetiology (4). Comparison of studies assessing antibiotic prophylaxis is additionally difficult due the use of various substances. Some studies used fluoroquinolones, which are contraindicated in children and adolescents until the end of the growing period. One study (2011) presented promising findings for amoxicillin/clavulanic acid prophylaxis in extremely severe AOM in children less than 2 years of age. However, such treatment was inevitably associated with increased adverse effects (4, 13, 14).
There is a strong genetic background for rAOM expressed as familial predisposition to inflammation. However, the exact genes responsible for this tendency remain unknown. Attending daycare facilities (nurseries, kindergartens) is an unquestionable risk factor due to higher exposure to upper respiratory tract infections (4, 8).
Substances such as xylitol (a substitute for natural sugar which reduces bacterial protein adherence to nasopharyngeal cells in vitro and in some in vivo studies), sprays containing Streptococcus salivarius and dornase alfa (used experimentally as a potential factor preventing biofilm formation) are under experimental investigation for preventing recurrences (4).
Tympanostomy tube insertion requires continuous, systematic otolaryngological care. Important is an assessment of tube function, i.e. its proper location and patency. An assessment of the state of tympanic membrane and the impact of the reverse of presurgical lesions, which often indicate chronic inflammation, such as retraction, retraction pockets or tympanic membrane atrophy; as well as differential diagnosis for secondary lesions after tube insertion, such as formation of granulation tissue around a “foreign body”, i.e. the tube, or tympanosclerosis, is also necessary (8, 13). Routine check-ups are performed every 4-12 weeks (7, 8). It is believed that grommets are associated with tympanosclerosis in about 1/3 of cases (8). In the MRC: TARGET 2001 study, tympanosclerosis was reported for 27% of ears after tube insertion vs. 0% of ears with no intervention during a 24-month follow-up period (15). As in our study, tympanosclerotic membranes were more common in children with previous ear interventions. Although the development of tympanosclerotic lesions is not fully understood, one of the concepts suggests that these lesions reflect tympanic repair processes (13). In a long-term follow-up, attention is also paid to the period of tube retention, tympanic membrane recovery after tube evacuation and potential signs indicative of recurrent inflammation. Persistent eardrum perforation usually occurs in children with a tendency to recurrent OME, particularly in younger children (under 3 years of age) (8). Any changes in the tympanic membrane may lead to conductive hearing loss (8).
Conclusions
Tympanostomy tube insertion is a basic procedure useful in the treatment of chronic otitis media with effusion. It improves life comfort of a growing child, allowing for normal reception of environmental stimuli, as well as the development of speech and social skills. In the case of elective procedures, an assessment of adenoid hypertrophy should be an inherent element of examination. The location and hyperplasia of the adenoid within the pharyngeal opening of the auditory tube affect middle ear and tympanic membrane condition. When deciding for grommet insertion, it should be remembered that despite its therapeutic role, the procedure is not neutral to the body and devoid of negative consequences. Therefore, appropriate qualification criteria based on clinical evaluation and objective hearing testing are of key importance. Post-operative patient monitoring until tube evacuation and in the later period is also important.
In cases of recurrent otitis media and acute complications of otitis media, this is often treatment of choice to supplement systemic antibiotic therapy. It may be combined with a more extensive procedure, such as antromastoidectomy, or serve as an initial stage of surgical treatment, allowing to avoid more extensive surgeries in some cases.
Current studies focus on biofilm structure, which is involved in the development of chronic and recurrent otitis media, and the associated innovative therapeutic approach. Some of these analyses are promising.
Piśmiennictwo
1. Pandey R, Zhang C, Kang JW et al.: Differential diagnosis of otitis media with effusion using label-free Raman spectroscopy: A pilot study. J Biophotonics 2018; 11(6): e201700259.
2. Rosenfeld RM, Shin JJ, Schwartz SR et al.: Clinical Practice Guideline: Otitis Media with Effusion (Update). Otolaryngol Head Neck Surg 2016; 154(1 suppl.): S1-S41.
3. Surgical management of otitis media with effusion in children. NICE Feb 2008.
4. Granath A: Recurrent Acute Otitis Media: What Are the Options for Treatment and Prevention? Curr Otorhinolaryngol Rep 2017; 5: 93-100.
5. Venekamp RP, Mick P, Schilder AGM, Nunez DA: Grommets (ventilation tubes) for recurrent acute otitis media in children. Cochrane Database of Systematic Reviews 2018; 5. Art. No.: CD012017.
6. Cheong KH, Hussain SSM: Management of recurrent acute otitis media in children: systematic review of the effect of different interventions on otitis media recurrence, recurrence frequency and total recurrence time. J Laryngol Otol 2012; 126: 874-885.
7. Gisselsson-Solen M (on behalf of the Reference group for the National Quality Register for Tympanic Membrane Ventilation Tubes): The Swedish grommet register ? Hearing results and adherence to guidelines. Int J Pediatr Otorhinolaryngol 2018; 110: 105-109.
8. Browning GG, Rovers MM, Williamson I et al.: Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children. Cochrane Database Syst Rev 2010; (10): CD001801.
9. Christine L, Barron BS, Louie B et al.: Identification of essential biofilm proteins in middle ear fluids of otitis media with effusion patients. Laryngoscope 2019.
10. Hall-Stoodley L, Ze Hu F, Gieseke A et al.: Direct detection of bacterial biofilms on the middle-ear mucosa of children with chronic otitis media. JAMA 2006; 296(2): 202-211.
11. Gok U, Bulut Y, Keles E et al.: Bacteriological and PCR analysis of clinical material aspirated from otitis media with effusions. Int J Pediatr Otorhinolaryngol 2001; 60(1): 49-54.
12. Ehrlich GD, Veeh R, Wang X et al.: Mucosal Biofilm Formation on Middle-Ear Mucosa in the Chinchilla Model of Otitis Media. JAMA 2002; 287(13): 1710-1715.
13. Branco C, Monteiro D, Paço J: Predictive factors for the appearance of myringosclerosis after myringotomy with ventilation tube placement: randomized study. Eur Arch Otorhinolaryngol 2017; 274: 79-84.
14. Oktay MF, Tansuker HD, Fukushima H et al.: Histopathology of tympanic membranes from patients with ventilation tubes. Auris Nasus Larynx 2018; 45(3): 427-432.
15. Browning GG: Two?year outcome of ventilation tubes in a randomized controlled trial of persistent childhood otitis media with effusion. Clinical Otolaryngology 2001; 26: 342?343.